Article Text

Abstract
Objectives Early palliative supportive care has been associated with many advantages in patients with advanced cancer. However, this model is underutilised in patients with haematological malignancies. We investigated the presence and described the frequency of quality indicators for palliative care and end-of-life care in a cohort of patients with acute myeloid leukaemia receiving early palliative supportive care.
Methods This is an observational, retrospective study based on 215 patients consecutively enrolled at a haematology early palliative supportive care clinic in Modena, Italy. Comprehensive hospital chart reviews were performed to abstract the presence of well-established quality indicators for palliative care and for aggressiveness of care near the end of life.
Results 131 patients received a full early palliative supportive care intervention. All patients had at least one and 67 (51%) patients had four or more quality indicators for palliative care. Only 2.7% of them received chemotherapy in the last 14 days of life. None underwent intubation or cardiopulmonary resuscitation and was admitted to intensive care unit during the last month of life. Only 4% had either multiple hospitalisations or two or more emergency department access. Approximately half of them died at home or in a hospice. More than 40% did not receive transfusions within 7 days of death. The remaining 84 patients, considered late referrals to palliative care, demonstrated sensibly lower frequencies of the same indicators.
Conclusions Patients with acute myeloid leukaemia receiving early palliative supportive care demonstrated high frequency of quality indicators for palliative care and low rates of treatment aggressiveness at the end of life.
- leukaemia
- end of life care
- hospice care
- quality of life
- supportive care
- pain
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What was already known?
Early palliative supportive care (ePSC) is underutilised in patients with haematological malignancies.
What are the new findings?
Patients with acute myeloid leukaemia receiving ePSC show high frequency of quality palliative care services and very low rates of aggressive treatment near the end of life.
What is their significance?
ePSC is feasible in and should be extended to patients with haematological malignancies.
Introduction
There is now convincing evidence on the benefits associated with the integration of early palliative supportive care (ePSC) to standard oncological care in patients with advanced solid cancers. These include improvement of disabling symptoms and quality of life (QoL), reduced aggressive treatments near the end of life, as well as longer survival and improved caregiver well-being.1–6
However, the potential value of ePSC in patients with haematological malignancies is still debated as there is paucity of evidence-based data. While some reports have shown that ePSC is feasible, only two randomised controlled trials (RCTs) have reported the advantages of an inpatient integrated model in patients with haematopoietic stem cell transplant (HSCT) or acute myeloid leukaemia (AML).7–13 A number of challenges remain to be addressed in patients with haematological malignancies, including the best target populations, misperceptions about the prognostic definition of haematological malignancies and the differences between palliative care and end-of-life care, and the limited availability of specialty palliative care programmes.10–17 Previous studies have found that patients with haematological malignancies have higher rates of cancer-directed care at the end of life and are less likely to be enrolled in hospice or home-care programmes.16 17 In particular, several studies have found that AML, the most common acute leukaemia in adults featuring high mortality rates, is characterised by a high frequency of aggressive end-of-life care, showing the presence of unmet palliative care needs in this population.18–23
The primary objective of this study was to investigate the presence of quality indicators for palliative care and end-of-life care in a series of consecutive patients with AML receiving outpatient ePSC in real life.
Materials and methods
Population
This is an observational, retrospective study based on patients with AML previously enrolled at the ePSC clinic of the Section of Hematology, Azienda Ospedaliero Universitaria Policlinico, University of Modena and Reggio Emilia, Modena, Italy, from 1 January 2014 to 1 September 2019. The team taking care of patients with AML consists of one physician and one fellow responsible for cancer treatment, and of another physician, one fellow and one psychologist with specialised training and expertise in delivering palliative care.
The palliative care team performs all palliative-specific tasks such as assessment and management of symptoms, providing support in decision making and future planning, facilitation of coping, and providing physical and emotional support. They also provide liaison with specific home-care services and regular phone calls to patients who cannot attend scheduled visits.4 24–29 The team also provides assessment of the prognostic awareness of patients, which is considered a fundamental component of the ePSC intervention.25
The ePSC intervention was started on the same day as the very first haematological outpatient visit. The frequency of follow-up encounters was driven by the disease trajectory.4 25–28 The intervention was defined early when provided within 8 weeks from cancer diagnosis.27 28 However, all patients were considered for the analyses.
According to data from the literature and to our previous experience with patients with solid cancer, we considered a full ePSC intervention when patients with AML received three or more visits in the ePSC clinic.25 29 Patients with only one or two visits were considered late referrals (late palliative care). However, we analysed the same indicators of quality for palliative care and of end-of-life aggressiveness in this cohort.
Patients with acute promyelocytic leukaemia and those undergoing allogeneic HSCT were excluded (the former due to an excellent prognosis and the latter because they are followed by the HSCT unit and post-transplant outpatient setting, for which an ePSC programme has not yet been developed at our institution).
Quality indicators for palliative care and indicators of aggressiveness at the end of life
Structured and comprehensive hospital chart reviews were completed for each patient to abstract the presence of indicators of quality for palliative and end-of-life care. The following indicators of quality for palliative care were considered: providing psychological support, assessing and managing pain, discussing goals of care (GOC) and prognosis, promoting an advance care planning (ACP), and accessing home-care service.16 30 31
For the purpose of this analysis psychological support was defined as any of the following: (1) a psychiatric or neurogeriatric consultation; (2) a psychological interview; and (3) a prescription for psychotropic drugs by a specialist. A GOC discussion was considered when the following elements were recorded in the hospital chart: goals and values, prognosis, treatment choices, life-sustaining treatment preferences, and discussion of either hospice or comfort care.31 The promotion of ACP was abstracted from the chart when all the following elements were documented: (1) presence of a written advance directive; (2) documentation of a GOC discussion; and (3) identification of a surrogate decision maker.31 The following indicators of quality of end-of-life care were recorded: (1) no chemotherapy within 14 days before death (the only chemotherapeutic agent allowed in such a period was hydroxyurea with the sole aim to control leukaemic cell count); (2) no intensive care unit (ICU) admission within 30 days before death; (3) fewer than two emergency department (ED) visits within 30 days before death; (4) fewer than two hospitalisations within 30 days before death; (5) no intubation within 30 days before death; (6) no cardiopulmonary resuscitation (CPR) within 30 days before death; (7) not dying in an acute facility; (8) no red cell transfusions within 7 days before death; (9) no platelet transfusions within 7 days before death; and (10) hospice length of stay >7 days before death.16 25 30 32 For the purpose of this analysis, acute facilities were considered as either those wards of the hospitals where chemotherapies are usually administered or those where invasive procedures are performed, namely haematological and oncological units, ICU, and coronary and thoracic care units.16 32
Symptom intensity measurements were considered 1 week (time 1), 4 weeks (time 2) and 12 weeks (time 3) from baseline assessment.
For deceased patients who received ePSC, the following medical and sociodemographic factors were collected: marital status, living circumstances, presence of offspring, education level, income, comorbidities (hypertension, diabetes, heart disease, renal impairment, chronic obstructive pulmonary disease, respiratory failure, other respiratory diseases, malnutrition, dementia, hypercholesterolaemia), age and type of chemotherapy. Their associations with the indicators of end-of-life care were also evaluated.
Statistical analysis
Descriptive statistics of the study variables were calculated as the absolute and percentage frequencies or mean, SD and range. Duration of home care, time from GOC and ACP to death, and overall survival were expressed in days and reported as median time and range.
Comparison of symptom assessments over time was carried out using paired Wilcoxon test. Only observed data were considered, without imputation for missing data.
The binary outcomes were summarised in terms of risks, whereas the mean and median were used for continuous ones. Comparisons between groups for binary outcomes were carried out using risk difference. Risk differences were reported along with their 95% CI. Comparison between medians was performed using Wilcoxon rank-sum test.
Significance level was set at p<0.05 and analyses were performed using R V.3.4.3 statistical software (The R Foundation for Statistical Computing, Wien, Austria).
Results
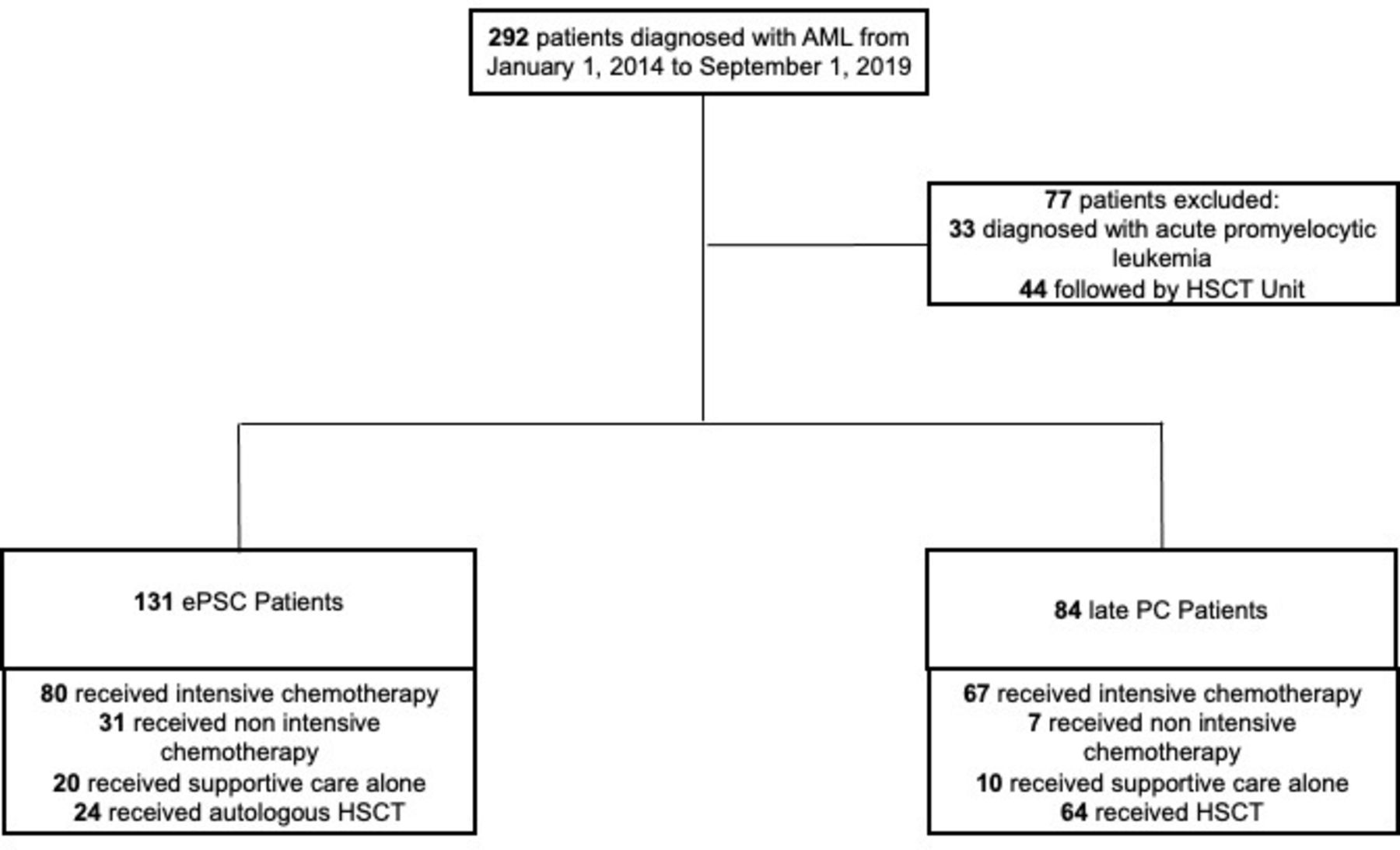
Overall, 131 patients with AML had three or more visits and thus met the inclusion criteria for ePSC, while 84 patients who had one or two visits were considered to have received late palliative care (figure 1).

Study flow chart. AML, acute myeloid leukaemia; ePSC, early palliative supportive care; HSCT, haematopoietic stem cell transplant; late PC, late referral to palliative care.
Patients’ characteristics are reported in table 1.
Characteristics of patients with AML enrolled in the study
The median time from AML diagnosis to first ePSC outpatient visit was 5 weeks (range, 0–21 weeks). Only 13 (10%) out of 131 patients were first referred to ePSC clinic more than 8 weeks from diagnosis.
Seventy-five (57%) ePSC patients out of 131 and 40 (47.6%) out of 84 late palliative care patients died during the follow-up period. The medical and sociodemographic characteristics of the 75 deceased ePSC patients are reported in table 2.
Characteristics of deceased patients with acute myeloid leukaemia receiving early palliative supportive care
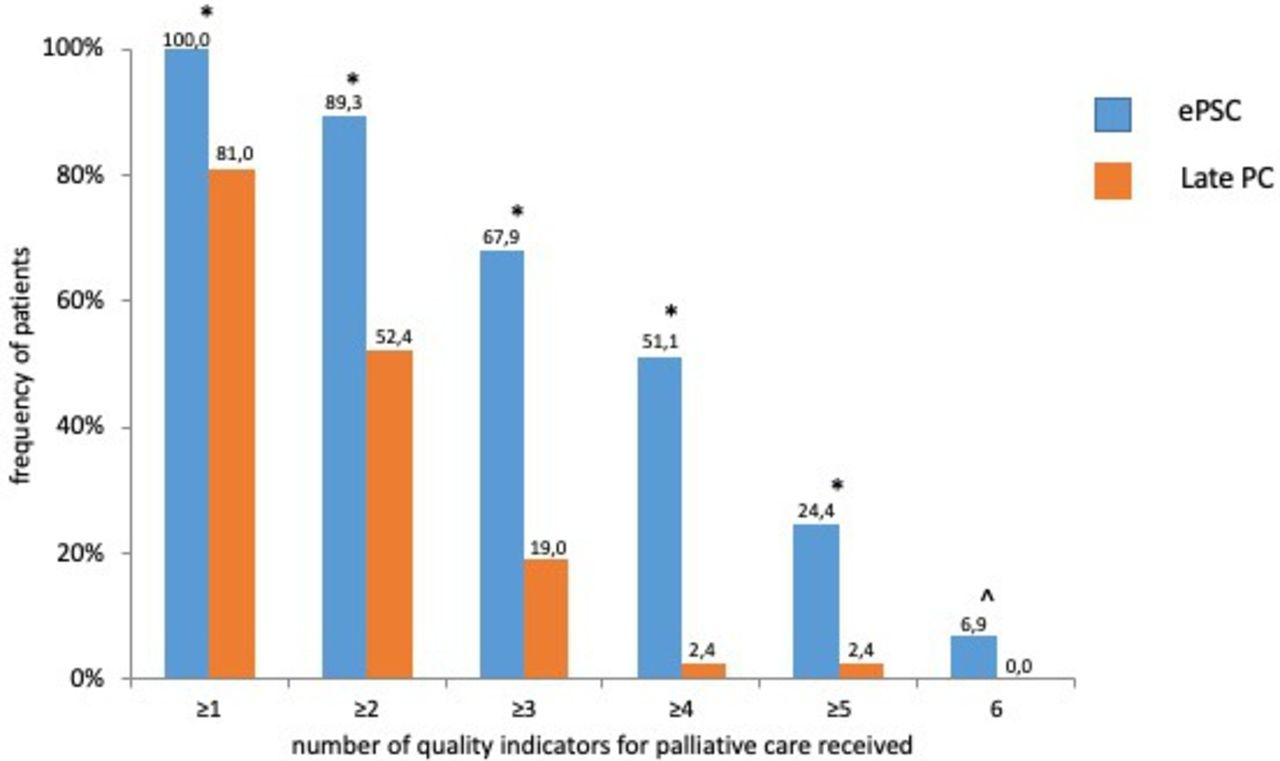
All ePSC patients received at least one, 117 (89.3%) patients at least two and 67 (51.1%) patients at least four indicators of quality for palliative care (table 3 and figure 2). Out of 84 late palliative care patients, 68 (81%), 44 (52.3%) and 2 (2.3%) received at least one, at least two and at least four indicators of quality for palliative care, respectively (table 3 and figure 2).
{kind=link}
{kind=link}
Frequencies of quality indicators for palliative care in patients with AML. Blue bars: patients with AML receiving early palliative supportive care; orange bars: patients with AML referred late to PC. *P<0.00001, ˆP=0.014. AML, acute myeloid leukaemia; ePSC, early palliative supportive care; late PC, late referral to palliative care.
Measures of quality indicators for palliative care in patients with acute myeloid leukaemia receiving ePSC intervention or late referral PC
All ePSC patients underwent assessment and management of physical symptoms and 72 (55.0%) out of 131 received psychological support.
Among the ePSC patients, there was a statistically significant improvement in pain intensity over time across all time points considered (p<0.01) (table 4). Out of 75 decedents, 44 (58.7%) received opiates during the last months of their life.
Pain assessment over time in patients with acute myeloid leukaemia receiving early palliative supportive care intervention
Out of 131 patients, 94 (71.8%) and 75 (57.3%) had GOC and ACP conversations, respectively. These figures were higher for patients who died, being 70 (93.3%) and 64 (85.3%) out of 75, respectively. The median time from GOC discussion and ACP promotion to death was 106 days (range, 4–585) and 25 days (range, 4–401), respectively. Fifty-seven patients (43.5%) received home-care services, with a median duration of 64 days (range, 3–3273) (table 3).
Of the ePSC patients, 2 (2.7%), 7 (9.3%) and 19 (25.3%) received chemotherapy in the last 14, 30 and 90 days of life, respectively. None of the ePSC patients was admitted to ICU, neither received CPR nor intubations within the last month of life. Only three (4%) ePSC patients had either multiple hospitalisations or two or more ED access in the last month of life. Of the ePSC patients, 29 (38.7%) and 20 (26.7%) had any ED access within 30 and 14 days of death, respectively. More than 40% of ePSC patients did not receive either red cell or platelet transfusions in the last 7 days of life (37 (49.3%) and 31 (41.3%), out of 75, respectively).
Of the ePSC patients, 11 (14.7%) and 48 (64.0%) received hospital-based hospice care and home-care service. Among ePSC patients, there were eight patients (10.7%) with a hospice length of stay longer than 1 week. The risk of dying at the hospital was 44.0% in ePSC patients. Of note, out of 75 ePSC patients, 4 (5.3%) and 38 (50.7%) died in an acute facility and either at home or in a hospice, respectively.
The indicators of end-of-life care in late palliative care patients are summarised in table 5.
Measures of aggressiveness of end-of-life care in patients with acute myeloid leukaemia receiving ePSC or late referral PC
The results of the evaluation on the association between end-of-life care and the medical and sociodemographic characteristics of 75 deceased ePSC patients are reported in online supplemental table 1.
Supplemental material
Discussion
In this study we found that ePSC can be delivered to patients with AML in the outpatient setting and that these patients had high rates of quality indicators for palliative care and very low rates of aggressive treatment near the end of life.
So far, current evidence has focused mainly on the feasibility of integrating palliative care in patients with haematological malignancies.7–13 More recently, two RCTs reported beneficial results in patients referred to ePSC during hospitalisations either for HSCT or for AML treatment plans. In the former setting, ePSC resulted in an improvement of major symptoms at 3 and 6 months post-transplant, while in the latter ePSC improved QoL, psychological distress and some end-of-life outcomes.11–13 Our findings support previous data and indicate that ePSC is also feasible in the outpatient setting, along the entire course of the disease in patients with AML.
Recent studies have found that quality measures of care are not uniformly provided to patients with haematological malignancies, that only a minority of them discuss ACP and GOC, and that these conversations are usually conveyed very late during the course of the disease.31 33 Our findings that slightly more than 50% of patients with AML have four or more indicators of quality of care, and even higher percentages that discuss GOC and ACP, support the notion that ePSC guides patients along the entire disease trajectory and that it is also associated with lower rates of cancer-directed therapies at the end of life among haematological patients by promoting prognostic awareness.13 24 Indeed only 2.7% and 9.3% of our patients received chemotherapy in the last 14 and 30 days of life, respectively. Our data are consistent with the findings that only 34.9% of patients with AML receiving ePSC undergo chemotherapy in the last 30 days of life compared with 65.9% patients receiving standard of care (SOC) in the sole multisite randomised trial so far published.13 The lower rates in our study could be related to the fact that ePSC was delivered as outpatient and was directed more frequently to patients undergoing front-line, non-intensive chemotherapy, who had more time to plan the end of anticancer active treatment, due to lack of reliable, standard second-line treatments. Previous reports from the SEER-Medicare database have shown that, among patients with AML, more than 10% and nearly 50% still receive cancer-oriented chemotherapy in the last 14 and 30 days of life, respectively, irrespective of age; nearly 90% are hospitalised within 30 days of death; and 30%–50% are admitted to the ICU within 30 days of death.19–22 Such figures are similar to those of a large cohort of haematological SOC patients with AML (n=1226) treated from 2012 to 2015 in Regione Emilia Romagna (RER), according to data from the ‘Regional Social and Health Agency’ registry.34 Of note, 11.3% and 19.7% of RER patients received chemotherapy in the last 14 and 30 days before death, respectively; 8.2% were admitted to the ICU; 57.9% had access to ED in the last month; 80% were hospitalised at least twice in the same time frame; 58.6% died in a hospital; and only 33.2% and 21.7% received opiates in the last month and home-care assistance, respectively.34 Our findings are also consistent with the data on patients with solid cancer randomised to receive ePSC and strongly support its implementation in AML routine practice to reduce cancer treatment aggressiveness near death.1–3 25 The exclusion of 84 patients from our study due to having less than three visits in the ePSC clinic reinforces the need for more and earlier clinician-based referrals and highlights the importance of timing of palliative care in routine clinical practice.3 7–13 25
A previous study on 43 patients with AML reported that palliative care consultation may reduce to 7% ICU admission in the last 30 days of life and increase home-care service to 30%, but is still associated with high rates of dying in acute facilities (53.5%).21 Our results extend these data by showing that palliative care integrated early in the course of the disease may further improve such figures, resulting in 0%, 64% and 5.3%, respectively. These latter results may be related to the fact that GOC were also discussed by patients’ primary haematologists and well in advance, with a median of 106 days, before death. Indeed, it has been reported that GOC discussions occurring too late and engaging transient members of the medical team were significantly associated with higher rates of intensive medical care close to death.31 33 Our data substantiate previous work from our group and other groups on the prevalence of pain in patients with AML35 36 and show that ePSC is associated with a statistically significant reduction in pain intensity also in this setting. The beneficial effects of a palliative care intervention, within 1 year from diagnosis, on pain management have so far been reported only in 67 patients with multiple myeloma.37
Our study has several limitations. First, the retrospective nature of the study could have affected the results due to unmeasured confounders. Second, incomplete data reporting may have underestimated the quality of care measures. Third, a single-centre study may have limited generalisability to other centres where trained supportive and palliative care teams may be less available. Finally, the lack of a control group of patients not receiving the intervention makes our results preliminary.
Our study also has strengths. It included a sizeable population of patients with AML receiving ePSC as outpatients, which increases the reliability of the results. Moreover, by showing that ePSC may positively influence all indicators of either quality of care or aggressive care near the end of life, recently accepted also by haematologists,16 our study represents one of the most comprehensive descriptions of such a topic in patients with AML treated in a real-life setting.
In conclusion, this study indicates that ePSC is effective in achieving a high frequency of quality palliative care services and low frequency of aggressiveness of end-of-life care in patients with AML. Moreover, it demonstrated the feasibility of ePSC in patients with haematological malignancies. Further prospective studies with a larger sample of patients are needed to confirm the generalisability of our findings.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study has been approved by the local ethics committee (protocol no: CE 833/2018).
Acknowledgments
We are indebted to Dr Maria Luisa Moro and all the staff of Regional Social and Health Agency, Regione Emilia Romagna, for their unceasing commitment and efforts to report and improve end-of-life care of oncological patients in our national area. We are also thankful to all the members of Gruppo Regionale Farmaci Oncologici ed Ematologici (GReFO), Regione Emilia Romagna, for their work on the appropriateness of antineoplastic drug prescribing, also at the end of life, in haematological patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
LP and MS contributed equally.
ML and EB contributed equally.
Contributors LP and MS have full access to all of the data used in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. LP, MS, DF, DG, FBa and RD'A contributed to the acquisition, analysis and interpretation of the data. EC, VP, MM, FF, FBe, AM, RM, AG, EBo, SB, FE, EBr, ML and EBa commented on the manuscript draft and final version and approved the submitted manuscript. DF, FBa and RD'A performed the statistical analysis. LP and ML are the guarantor of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests FF: advisory boards for Janssen and Novartis and travel grants from Jazz Pharmaceuticals, outside the submitted work. RM: honoraria from AbbVie, Roche, Janssen and Shire, outside the submitted work. FE: consultancy for AbbVie, Amgen, Janssen, Orsenix and Takeda and grants from Amgen (to his institution), outside the submitted work. EB: grants from Helsinn Healthcare, outside the submitted work. ML: advisory board for AbbVie, Novartis, Gilead Sciences, Jazz Pharmaceuticals, Sanofi, MSD and Daiichi Sankyo and travel grant from Gilead Sciences.
Provenance and peer review Not commissioned; externally peer reviewed.