Article Text

Abstract
Timely access to medicines within the community is important for palliative patients where their preferred place of care is the home environment. The objective of this observational study is to establish baseline data to quantify the issue of poor access to medicines for symptom control in the last few days of life. The list of 13 medicines was generated from medicine use within a metropolitan palliative care unit. A survey was designed to determine which of these 13 medicines community pharmacies stock, the expiry date of this stock, awareness of palliative care patients by community pharmacists and basic demographic characteristics of the community pharmacies. Surveys were distributed, by post, to all community pharmacies in South Australia. The response rate was 23.7%, and was representative of all socioeconomic areas. Each pharmacy stocked a median of 3 medicines (range 0–12) with 1 in 8 pharmacies having none of the 13 medicines listed in the survey. When the data was combined to identify the range of medicines from all pharmacies within a geographical postcode region, the median number of medicines increased to 5 medicines per postcode. Just over 1 in 5 pharmacies reported learning about the palliative status of a patient through another health practitioner. Community pharmacies remain an underused resource to support timely access to medicines for community-based palliative patients. Palliative care services and government agencies can develop new strategies for better access to medicines that will benefit community patients and their carers.
- Home Care
- Quality Of Life
- Symptoms and Symptom Management
- Terminal Care
- Supportive Care
Statistics from Altmetric.com
Introduction
Good symptom control combined with advanced planning is crucial in achieving a greater likelihood of palliative care patients remaining in their preferred place of care for longer.1 Whether the setting of care is a residential aged care facility, an acute hospital ward, or at home, appropriate levels of support—including medicine availability—must be in place to provide a successful outcome.2 Models have been developed in palliative care, allowing prompt symptom control through physical and pharmacological interventions for patients.3 The literature describes the unique challenges of providing care in the home environment, including difficulty in timely accessing prescribed medicines.4 ,5 This is particularly relevant in the terminal phase of life where distressing symptoms can appear unexpectedly.
Symptoms experienced by patients in the terminal phase may include one or more of: fatigue, dyspnoea, pain, nausea, delirium, agitation and noisy secretions.6 These symptoms may begin suddenly or have gradual onset. The ability to manage these symptoms promptly is important in reducing patient and carer distress: quality of life remains the central goal in palliative care. The terminal phase can also be associated with decreased energy levels, reduced ability to swallow and impaired mental state, thus limiting the choice of routes for administering medicines.7
The Pharmaceutical Benefits Scheme (PBS) was introduced in Australia in 1948 to subsidise the cost of a range of medicines at the time of dispensing to patients. The patient pays a fixed contribution and the remainder is subsidised by the Federal Government. Some medicines’ costs are below the fixed contribution threshold. While the PBS is broad in scope, it is a finite list: some parenteral opioids used in palliative care, such as fentanyl and oxycodone, are unsubsidised. If these medicines are required for people at home and dispensed through their community pharmacy the patient pays the full cost of the medicine. Inpatients within public hospitals receive medicines during their admission without charge. Consequently, there may be a financial incentive for an inpatient admission over community-based care, if patients are unable to cover the costs of the relatively small group of medicines that remain unsubsidised.
In 2004, a specific palliative care section of the PBS was introduced as part of a range of initiatives aimed at improving access to quality palliative care within the community.8–10 This section allows larger quantities of medicines, such as opioids. The patient must be identified as palliative, in order to access this expanded list of subsidised medicines.
This study was designed to provide objective baseline data to identify gaps that may exist in the timely access to palliative medicines for patients being cared for within the community and consequently recommend strategies for improvement.
The primary outcome measured is the likelihood of prompt access to a range of medicines used to treat common terminal symptoms through community pharmacies.
Methods
The study cohort comprised all (455) registered community pharmacies in South Australia. The business names and addresses of the pharmacies were obtained from the Pharmacy Regulation Authority SA (PRASA).
To assess the level of relevant medicines currently stocked for end-of-life symptom management within South Australian community pharmacies, a Terminal Phase Medicines (TPM) list was constructed (see box 1). The lead author, a palliative care pharmacist, developed this in consultation with a multidisciplinary group of colleagues. The TPM list was simply intended to provide for a range of medicines and formulations that are prescribed for this patient group.
Terminal Phase Medicines list
Clonazepam 1 mg injection*
Clonazepam 2.5 mg/mL oral drops*
Dexamethasone 4 mg/mL injection*
Fentanyl 100µg/2 mL injection
Haloperidol 5 mg/mL injection*
Hydromorphone 10 mg/mL injection*
Hyoscine Butylbromide 20 mg/mL injection*
Hyoscine Hydrobromide 400 µg/mL injection
Metoclopramide 10 mg/2 mL injection*
Midazolam 5 mg/mL injection
Morphine 10 mg/mL injection*
Morphine 10 mg/mL oral mixture*
Oxycodone 10 mg/mL injection
*Subsidised by the Australian Pharmaceutical Benefits Scheme
The list of medicines was selected through a review of discharge prescription data within a local inpatient palliative care unit. A systematic approach was used to develop a short list that illustrated the range of medicines that could be used for symptom control in the last few days of life and may need to be accessed through a community pharmacy. The process of reviewing the list of discharge prescription data took into account the medicines:
-
Where evidence existed for pharmacological management of symptoms commonly observed in the terminal phase of a palliative illness;
-
Which were registered in Australia;
-
That could be administered as either an oral liquid or subcutaneous injection, to account for the dysphagia expected in this patient population.
Where several concentrations existed for the same formulation, the most commonly prescribed item was selected.
A survey (see box 2) was compiled (full survey is available from the primary author) with the purpose of:
-
Establishing the likelihood of community pharmacies having medicines from the TPM list in their pharmacy;
-
Establish the range of the shelf life of the stock held;
-
Identifying level of awareness of palliative care patients or their carers using their service; and
-
Identifying demographic characteristics of the pharmacy.
Suggested responses with check boxes were used to prompt for most of the information. These suggested responses were gathered from informal conversations with community pharmacy colleagues. Some open questions were used where necessary. Open questions were evaluated for common themes.
Summary of Community Pharmacy Survey
Demographics of the pharmacy
-
Role of the person completing the survey;
-
Postcode of where pharmacy is located;
-
Number of pharmacists (full time equivalents) working at the pharmacy;
-
Pharmacy usual opening hours; and
-
Clinical and supply services offered by the pharmacy.
Awareness of palliative patients
-
Knowledge of how many palliative patients had used the pharmacy over the previous 12 months;
-
How they became aware of palliative status; and
-
The range of issues affecting timely access to these medicines.
Access to stock
-
Date of completing the survey;
-
Existence of medicines from the Terminal Phase Medicines list in their dispensary; and
-
Shortest expiry date of each item held within the pharmacy.
Willingness to be part of an email distribution list
All questions were reviewed by peers to provide objectivity.
All 455 community pharmacies in South Australia were mailed a personally signed covering letter, the survey, and a return addressed envelope, as suggested by the Dillman Total Design Survey Method.11 Responders were also offered a facsimile number to which to return the completed survey.
To ensure anonymity of the pharmacies involved, each community pharmacy was allocated an individual code. Once the survey was returned, the data were entered into a secure results database.
All responding pharmacies were allocated to a decile (constructed by dividing the postcodes in South Australia into state-based deciles of Seifa score) of the Socio-Economic Index for Areas (Seifa), Index of Relative Socio-Economic Disadvantage 2006 based on the postcode identified.12
No reminders were sent out.
All data were statistically analysed through Stata V.12 software (StataCorp 2011. Stata Statistical Software: Release V.12. College Station, Texas, USA: StataCorp LP). Continuous data was compared using a two-sample Wilcoxon rank-sum (Mann-Whitney) test. Categorical data was compared with a χ2 test.
Results
Participating pharmacies
A total of 455 surveys were mailed and 12 were returned without opening. Of the remaining 443 pharmacies, 105 (23.7%) completed surveys were returned using the reply address envelope supplied to them. No surveys were returned by fax.
All respondents identified themselves as registered pharmacists (see table 1).
Identified role of person completing the survey
Responding pharmacies had a median of two pharmacists on staff (range 1–10) and participated in a range of services, including preparing dose administration aids (92.4%), Home Medicines Reviews (91.4%) and home delivery service (76.2%). Selected pharmacies offered an after-hours or on-call service (17.1%), provided medicines for a local hospital (15.2%) or provided a clinical service for a local hospital (12.4%).
Forty-two (40.0%) responses came from pharmacies with a rural postcode and 63 (60.0%) from metropolitan Adelaide.
Because surveys were received from a broad range of socioeconomic areas, the data were considered to be sufficiently geographically representative of all pharmacies in South Australia and no follow-up letters were sent out.
Current stock holdings from the TPM list
Each pharmacy stocked a median of three medicines (range 0–12) from the TPM list (see figure 1). Thirteen (12.3%) pharmacies had none of the medicines on the list.

Number of community pharmacies with stock from the Terminal Phase Medicines list.
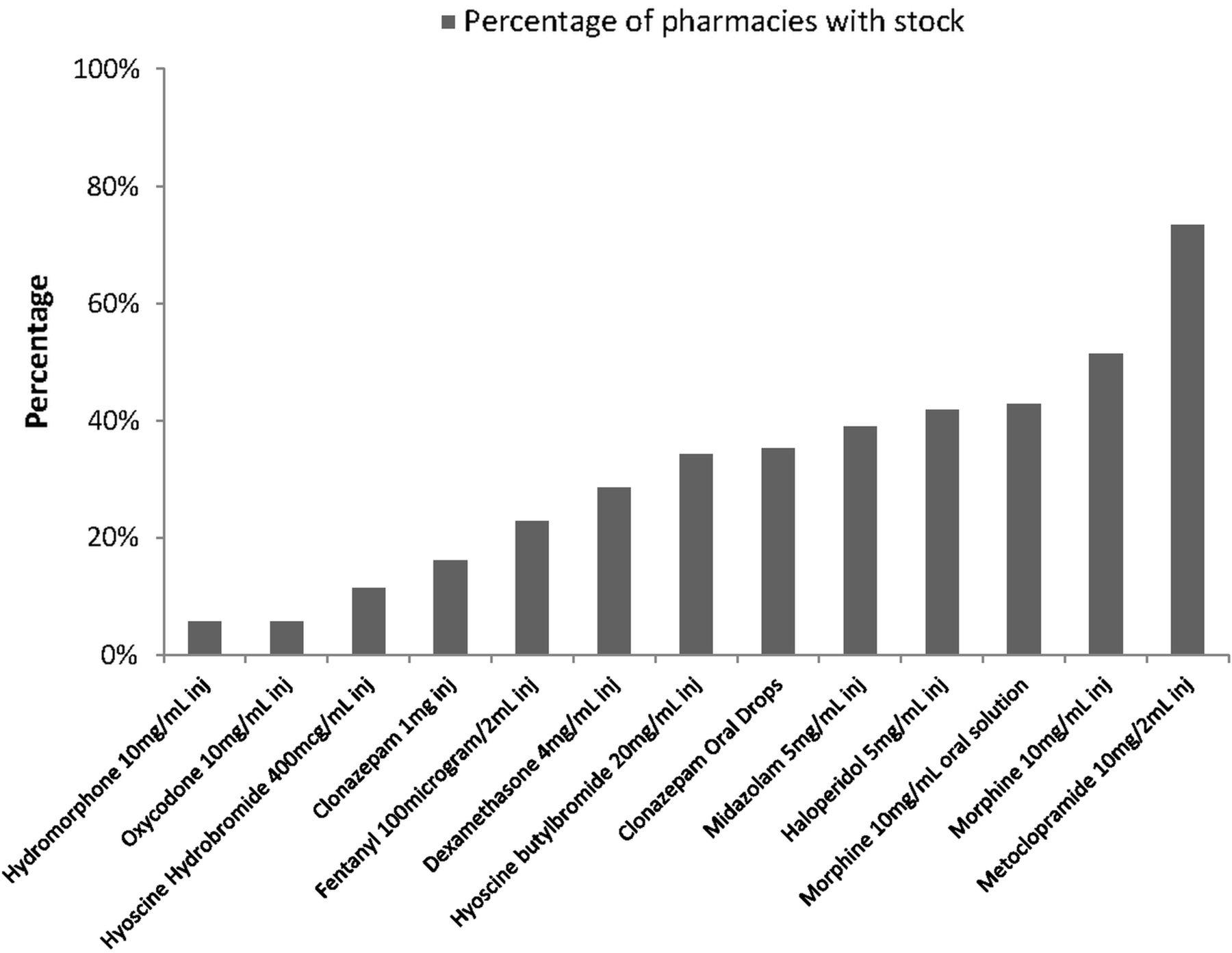
The percentage of responding pharmacies stocking each medicine is shown in figure 2. The four most commonly held medicines, metoclopramide 10 mg/2 mL injection (73%), morphine 10 mg/mL injection (51%), morphine 10 mg/mL oral solution (43%) and haloperidol 5 mg/mL injection (41%), are all listed on the PBS.
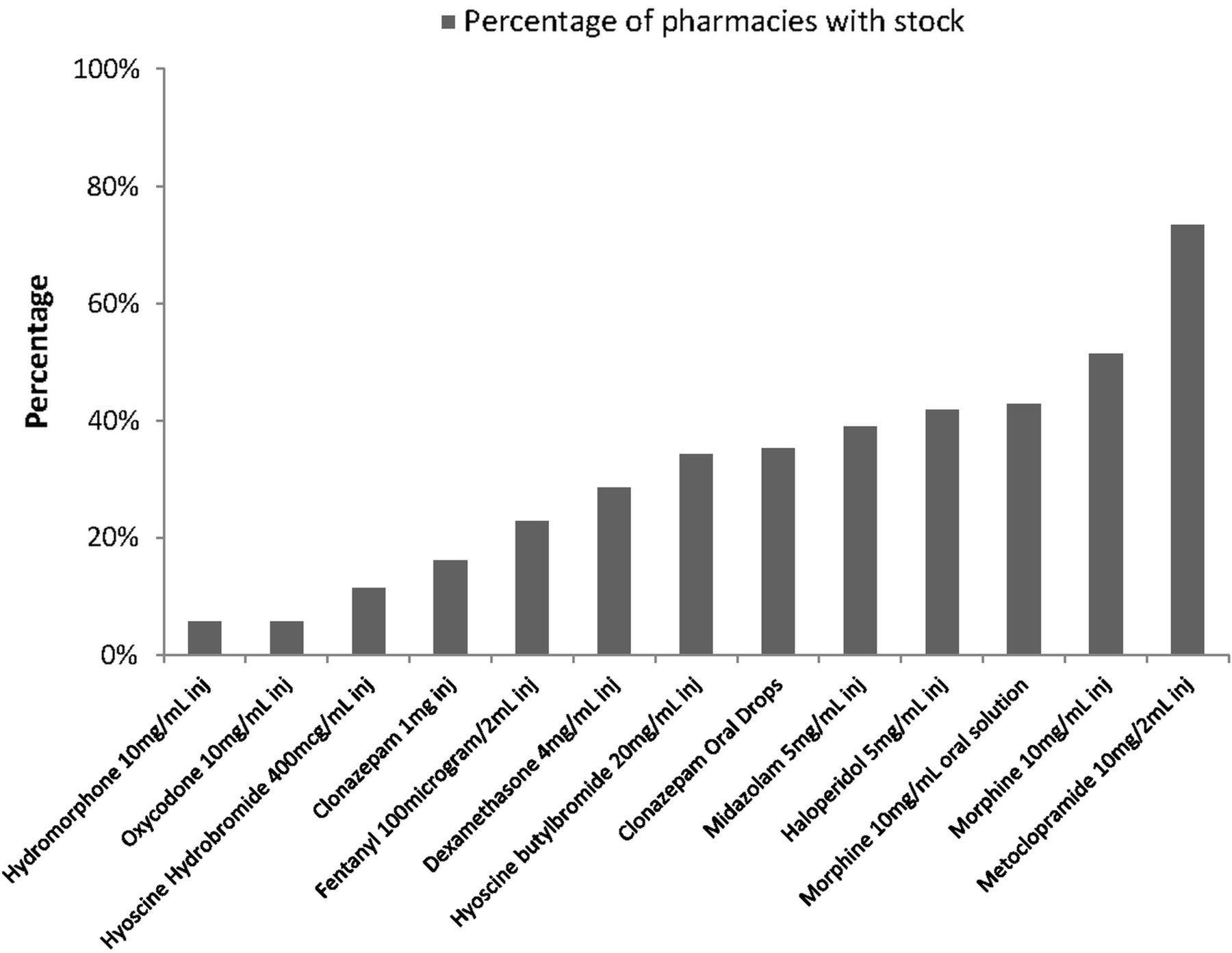
Proportion of pharmacies with medicines from the Terminal Phase Medicines list.
Medicines least likely to be found in a community pharmacy were: oxycodone 10 mg/mL injection (6%) and hydromorphone 10 mg/mL injection (4%).
Data was collected from 73 (22.9%) separate postcodes across South Australia. When the availability of medicines from the TPM list was measured from all pharmacies within a specific postcode, the median number increased from three medicines per pharmacy to five medicines per postcode region.
Metropolitan community pharmacies held a median of 2.5 medicines (range 0–12) from the TPM list. This was significantly lower (p=0.0063) than the median of five medicines (range 0–11) held in rural pharmacies.
While none of the pharmacies surveyed held every medicine from the list, 102 (97.1%) pharmacists acknowledged they would employ multiple strategies to source the item, if they did not stock it. The most common strategy (77.2%) to source the item immediately was to contact another pharmacy, on the patient's behalf. A smaller proportion of pharmacists indicated they would contact the doctor on the patient's behalf, to recommend a change in medicine (20.0%), or to recommend a change in strength of the medicine (25.7%). Only two pharmacists indicated they would tell the customer that the medicine was unavailable and then purchase the item through their regular ordering arrangements (which may take a day or so to arrive).
Awareness of palliative patients using the pharmacy
Ninety-one (86.7%) pharmacists surveyed were aware of at least one palliative patient or carer using their business over the previous 12 months. However, only 22 (21.0%) reported learning about the palliative status of a patient through another health practitioner. This latter group held a median of 5.5 medicines from the TPM list (range 0–11). This was statistically higher (p=0.0057) than the median of three medicines (range 0–12) held in those pharmacies that did not report learning about the palliative status of a patient through another health practitioner.
Compared with metropolitan pharmacists, a statistically greater number of rural pharmacists (34.2% vs 12.5%) learnt about the palliative status of a patient through another health practitioner (p=0.008).
Expiry dates
Figure 3 shows the median expiry (in months) of each medicine along with the minimum and maximum recorded months unexpired. Most items had a median expiry of greater than 12 months, with the exception of dexamethasone 4 mg/mL injection (10 months).

Median, minimum and maximum time to expiry.
Discussion
These findings provide an objective baseline measurement of the availability of medicines used to treat a number of common symptoms in the terminal phase through community pharmacies, and thus, the likelihood of patients being able to promptly access these medicines. Timely access to metoclopramide 10 mg/2 mL injection is possible from the majority of community pharmacies. The availability of the remaining medicines on the TPM list was limited, across the cohort of pharmacies surveyed. However, pharmacists consistently indicated that in the event they were unable to supply a medicine, they would contact other pharmacies within the vicinity. This finding combined with the evidence that a larger range of medicines was available across a given postcode provides support for a community pharmacy hub and spoke model. This is where a selected pharmacy within a geographical location undertakes to stock a small range of medicines under an agreement and to support other pharmacies in the geographical region to quickly access the required medicine. The focus for palliative care organisations is to work with community pharmacies and general practitioners to build geographical networks to ensure that a range of medicines are available in a timely manner. Abel et al13 describe this model as circles of care.
The expiry data illustrates this group of medicines can remain in community pharmacy dispensaries for some months without going out of date and affecting stock management. There is opportunity to further improve stock turnover, and thus, the shelf life through developing strategies. This may involve the nomination of a (hub) pharmacy to carry a range of agreed medicines for a geographical area while encouraging consistent prescribing patterns through education programmes for local prescribers. In turn, this could improve the appeal for pharmacy managers to keep this small range of medicines as they are avoiding the cost and inconvenience associated with expired stock.
One in five community pharmacies acknowledged they had learnt about a palliative patient from another health practitioner. This group of pharmacies were statistically also more likely to stock medicines from the TPM list indicating that pharmacies receiving greater communication from other health practitioners are more likely to hold a greater number of medicines for palliative symptoms. Further research is warranted to investigate this association. Anticipatory discussions with the palliative patient's regular community pharmacy at an earlier point of the care journey make practical sense given the speed and unpredictability of deterioration. Community pharmacies are often geographically isolated from the healthcare team, yet are an integral stakeholder with regards to access to medicines.
Community pharmacies provide an important range of healthcare services in the community beyond their traditional supply role.14 While the focus of this survey was to establish the capacity of community pharmacies to supply core palliative medicines in a timely fashion, other services provided by some pharmacies—including the preparing of dose administration aids and the conducting of Home Medicines Reviews—are valuable interventions for this patient group and their carers.
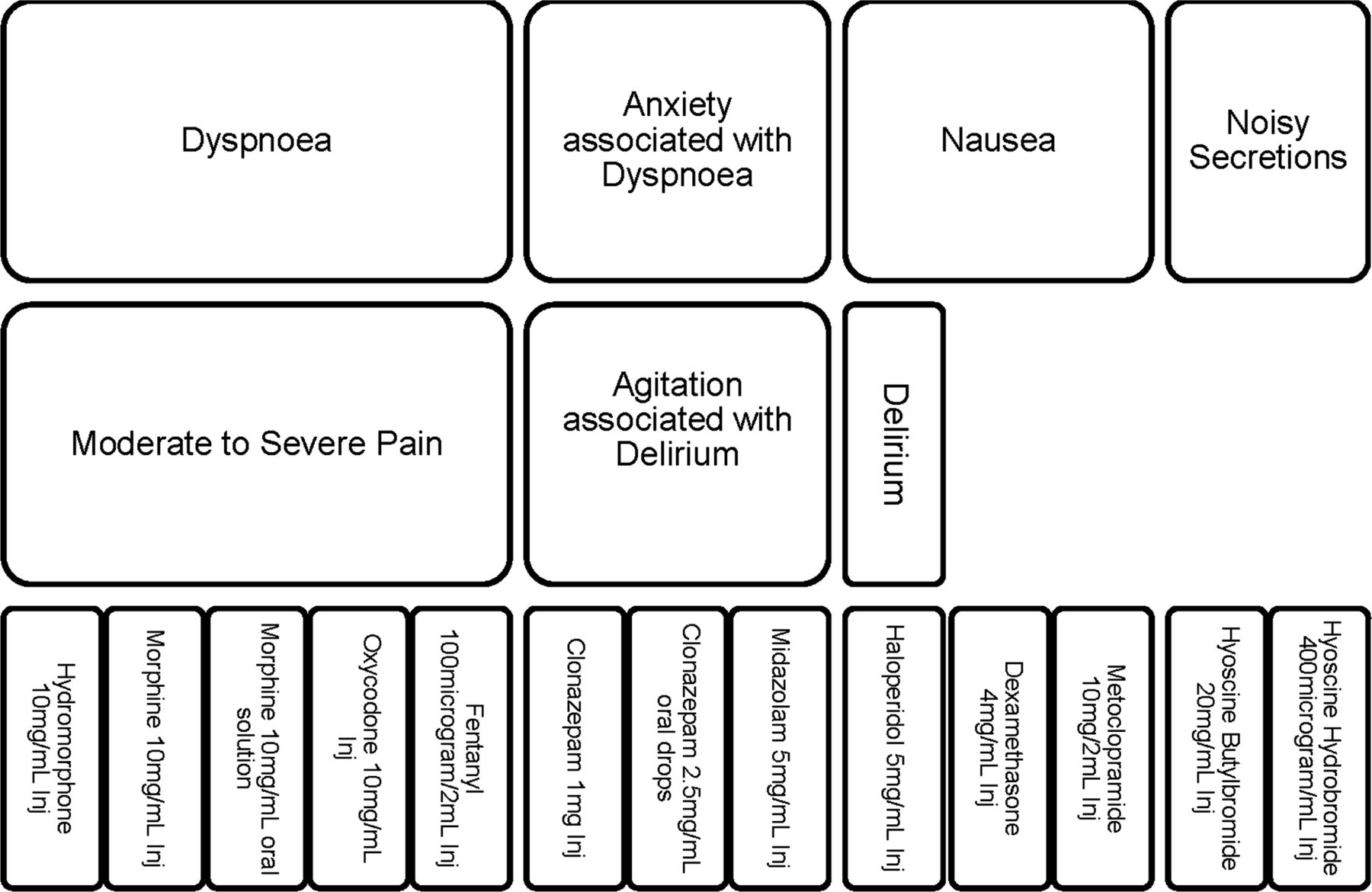
The TPM list developed for this survey contained 13 distinct items. It is an overview of the range of medicines that are likely to be prescribed, and was based on prescribing patterns from a metropolitan inpatient palliative care unit. It was never intended to be a complete list of medicines that could be used to treat palliative symptoms. Many of these medicines overlap in the symptoms they are designed to manage (see figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overlap of symptoms managed by Terminal Phase Medicines list.
Palliative patients being managed in the community often have less complex needs than those cared for in hospices and inpatient facilities. Therefore, it is likely that the range of medicines needed within the community setting to treat terminal-phase symptoms, may be less than required in a tertiary inpatient palliative care unit. Potentially, better engagement between community-prescribing practices and pharmacy stock holdings could be directed at a narrower range of medicines that address more than one symptom.
In Australia, consensus guidelines exist to support prescribers and pharmacists alike with regards to the appropriate medicines to prescribe and to stock for palliative symptoms.15 These results show there is a poor fit between these guidelines and the medicines community pharmacies stock. This probably reflects diversity in prescribing practices, and the relatively small number of palliative care patients that access medicines through an individual pharmacy each year. Therefore, pharmacy managers are currently unable to reliably anticipate which medicines to make available. In practical terms, this may well lead to delays in access to medicines for the management of terminal symptoms. This observed poor fit between stock levels and prescribing practices paves the way for more structured education of community prescribers and pharmacy managers to encourage use of a narrower list of medicines for the range of terminal symptoms in non-complex community patients.
Organisations across the globe have studied the problem of timely access to palliative medicines through different lenses. Palliative medicine kits containing a small number of medicines have been used in the home as a means to anticipate symptoms and address comfort for dying patients being cared for in the community.1 ,16–18
In Australia, a range of injectable emergency drugs are provided to prescribers for use in situations where urgent access to medicines is required. This includes medicines that are useful in treating symptoms common in the terminal phase.19 This list of medicines is available free of charge to prescribers who may order up to a specified maximum quantity of each medicine via the PBS, on a monthly basis. The prescriber can then issue this restricted range of medicines free to patients, in an emergency. This is known as the Prescriber Bag (Emergency Drug) Supply.
A succinct TPM list would be the foundation for a broad range of applications, including supporting community pharmacy hubs where pharmacies within a local geographical network can communicate between each other to coordinate timely medicine supplies. This model is likely to succeed within a metropolitan area where there is a median of 2 (range 1–17) pharmacies per postcode region. This model could also work in selected rural centres.
The Australian Government has recently invested in an electronic health (eHealth) record system that places the patient at the centre of their own healthcare. This offers the capacity for patients and their healthcare providers to securely access health information, thus improving communication between healthcare providers, with the potential for better advanced care planning and improved medicines management for community patients.
Lucey et al5 performed a qualitative systems analysis of the process by which palliative patients obtain medicines. They identified a number of factors that have caused delays in accessing medicines. These include medicines not being stocked in community pharmacies, specific formulations being unavailable and medicines being unsubsidised through federally funded schemes. Our data supports their findings and quantitatively demonstrates the likelihood of accessing a range of medicines in the last few days of life.
Limitations
Medicines were selected for the TPM list based on usage within one metropolitan inpatient palliative care unit. Whether the concentrations selected for each medicine reflect community prescribing for palliative symptoms is unknown. For example, the availability of the 10 mg/mL hydromorphone injection was the lowest of all the medicines. The authors note the 10 mg/mL hydromorphone is about five times the potency of the other parenteral opioids included within the list. The results for stock levels of this medicine may have been different if the equivalent potency strength (2 mg/mL) of hydromorphone was included within the TPM list.
The study was conducted using a postal survey. As the responders were asked to use information from the pharmacy shelves—including stock availability and expiry dates—the postal survey was considered more practical to use in this instance. Irrespective of the practical intentions, postal surveys have a larger response rate to online surveys.20
The response rate of 23.7% achieved with one mailing of the survey is low. However, since the responses came from a wide distribution of socioeconomic areas and the proportion of rural postcodes expected, this was considered an acceptable representative sample of the overall pharmacy population.
The use of a survey relies on recall which can be biased. The use of suggested responses and checked boxes within the survey to encourage information may have shifted the thinking of some respondents from actual to best practice. However, given the range of responses, it appears likely the strongest viewpoints have been reported.
While postcodes are a valuable system in arranging data and models of service delivery across a geographical region, it is important to consider that postcodes across Australia vary significantly by population and area. The largest South Australian postcode region measures 258 139 km2 making it larger than the land area of the UK. It is unfeasible to consider a hub and spoke model in such a remote part of the country.
Recommendations
Health practitioners should identify the patient's usual community pharmacy and involve the pharmacist in discussions about care planning related to medicines for community-based palliative patients in advance.
Palliative care organisations should collaborate with medical, nursing and pharmacy organisations to develop an agreed core medicines list that would support symptom management in non-complex community palliative patients. It should take into consideration cost, access to government subsidies (eg, PBS), pharmacokinetics and shelf life.
Policy makers need to put in place incentives for community pharmacies to hold a small range of medicines that may be required urgently, but so infrequently, that loss of stock due to expiry is otherwise a financial burden.
Conclusion
Enabling palliative patients to receive care in their home environment is good public health practice. This study provides valuable evidence to enable palliative care services and government agencies to develop new strategies for better access to medicines for community patients. While there are many challenges that affect symptom control for palliative patients in their home environment, access to medicines for the relief of frequently encountered symptoms should not be one of them.
Acknowledgments
We would like to thank Mrs Anne Friedman for her valuable assistance in distributing the survey, and the staff of the responding community pharmacies for their cooperation.
References
Footnotes
-
Contributors PAT initiated the collaborative project, designed the Terminal Phase Medicines (TPM) list and the community pharmacy survey, monitored data collection for the whole trial, cleaned and analysed the data, and drafted and revised the paper. He is guarantor. JG and PH supported the design of the community pharmacy survey, analysed the data, and revised the draft paper. BM supported the design of the community pharmacy survey, and revised the draft paper. DCC supported the design of the TPM list, and revised the draft paper. DSR designed the TPM list and the community pharmacy survey, and revised the paper.
-
Competing interests None.
-
Ethics approval Ethics approval for the study was obtained from the Southern Adelaide Clinical Human Research Ethics Committee (SAC HREC).
-
Provenance and peer review Not commissioned; externally peer reviewed.