Article Text

Abstract
Purpose Although surrogate decision-making (SDM) is prevalent in intensive care units (ICUs) and concerns with decision quality are well documented, little is known about how clinicians help family members understand the surrogate role. We investigated whether and how clinicians provide normative guidance to families regarding how to function as a surrogate.
Subjects and methods We audiorecorded and transcribed 73 ICU family conferences in which clinicians anticipated discussing goals of care for incapacitated patients at high risk of death. We developed and applied a coding framework to identify normative statements by clinicians regarding what considerations should guide surrogates’ decisions, including whether clinicians explained one or more of Buchanan and Brock’s three standard principles of SDM to family members.
Results Clinicians made at least one statement about how to perform the surrogate role in 24 (34%) conferences (mean of 0.83 statements per conference (1.77; range 0–9)). We observed three general types of normative guidance provided to surrogates, with some conferences containing more than one type of guidance: counselling about one or more standard principles of SDM (24% of conferences); counselling surrogates to make decisions centred on the patient as a person, without specifying how to accomplish that (14% of conferences); and counselling surrogates to make decisions based on the family’s values (8% of conferences).
Conclusions Clinicians did not provide normative guidance about the surrogate role in two-thirds of family conferences for incapacitated patients at high risk for death. When they did, clinicians’ guidance was often incomplete and sometimes conflicted with standard principles of SDM. Future work is needed to understand whether providing explicit guidance on how to perform the surrogate role improves decision-making or mitigates surrogates’ psychological distress.
- decision making
- end-of-life care
- clinical ethics
Statistics from Altmetric.com
Introduction
Roughly one in three elderly Americans will require a surrogate to make decisions for them at the end of life because they lack decision-making capacity.1 Over two decades ago, bioethicists provided a theoretical analysis of how to make such decisions ethically, which has become part of the medical ethics canon.2 According to this conventional paradigm, there are three standards or principles of surrogate decision-making. The first standard requires that ‘where a clear and bona fide (written or spoken) advance directive is available, it is to be followed’,3 which may be called the stated preferences standard. The second standard requires ‘a surrogate…choose as the patient would choose if the patient were competent and aware’.3 This is called the substituted judgement standard because it asks the surrogate to make a judgement about treatment options based on her knowledge of the patient. The third standard is called the best interest standard or principle, which ‘states that a surrogate is to choose what will best serve the patient’s interests’ or will most promote the patient’s good.3 This standard is intended to be applied in cases where little is known about the patient’s values or where the patient is deemed unable to have developed wishes because of age or intellectual disability.
Although these principles of surrogate decision-making have become orthodoxy in bioethics, empirical work indicates that surrogates often do not make decisions that are consistent with normative theory. For example, surrogates often make decisions that differ from what patients would choose for themselves,4 and surrogates’ decisions are sometimes more consistent with their own preferences than with patients’ preferences.5 6 However, little is known about why this occurs. One possibility is that there may be shortcomings in whether and how clinicians counsel surrogate decision-makers about how to make decisions. For example, perhaps clinicians do not counsel surrogates about their role responsibilities, which may leave surrogates more susceptible to well-documented projection biases,6 7 or perhaps they advise an approach to surrogate decision-making that is substantially different from the conventional approach described by Buchanan and Brock.
We therefore investigated whether and how clinicians communicate with surrogates about principles of surrogate decision-making during audiorecorded family conferences in intensive care units (ICUs).
Study methods
Data collection
The current study stems from a previously described dataset of audiorecorded ICU family conferences.8 9 No published studies have addressed the question of whether and how clinicians educate family members about the surrogate role in making decisions for incapacitated patients. Clinician–surrogate conferences were audiotaped at two California hospitals from January 2006 to August 2008. Eligible conferences were those in which the attending physician anticipated a discussion of withholding or withdrawing treatment or discussing bad news, occurred on weekdays, included family and clinicians, and took place in English. Conferences included physicians and allied health providers, such as social workers. As we use the term ‘clinician,’ such allied health providers are included. We excluded conferences if the patient was younger than 18 years old. Permission to approach each family was given by the attending physician and bedside nurse. Each conference was audiotaped after informed consent was obtained. Institutional review boards at each hospital approved all procedures. All conferences were transcribed verbatim.
Qualitative analysis
Our coding strategy used Crabtree and Miller’s methods for both template (deductive) and open (inductive) coding10 to analyse clinician communication with family members about values and preferences in surrogate decision-making.
We chose a deductive coding strategy to describe whether and how often clinicians counselled patients about standard principles of surrogate decision-making. Using Buchanan and Brock’s theoretical framework described in the introduction,3 we defined three standard principles of surrogate decision-making. Then we coded conversations, looking for statements where clinicians explained one or more principle of surrogate decision-making. When coding, we were inclusive and charitable in our identification of clinician statements. For example, when coding for statements of the substituted judgement standard, we included any statement in which clinicians counselled family to be guided by what they know about the patient’s values or what they think the patient might choose for herself.
For our inductive coding strategy, we used the method of qualitative description to code conversations a second time, looking for statements where clinicians stated any norms for making decisions for an incapacitated loved one. Qualitative description is a method of qualitative data analysis that provides a data-derived approach for describing behaviours that are not specified a priori for inclusion in an initial coding framework.11 We iteratively and recursively developed codes for these behaviours by mutual agreement and then applied them to the entire set of conversations.
Two coders (TC and LS) independently applied the coding schema to the 73 audiotaped transcripts. Coding was comparative and recursive. A subset of 12 transcripts was double coded. Inter-rater reliability was good (κ >0.7). We used ATLAS.ti 6.2 (Berlin, Germany) for qualitative data management and preliminary analysis.
Quantitative analysis
Using ATLAS.ti 6.2 for data management, we generated a table of frequency counts of coded behaviours by conference, which we then analysed quantitatively using STATA V.11.0. To capture how often a decision-making norm was discussed as a proportion of all conversations, we calculated the percentages of conferences where behaviours occurred. To measure the amount of clinician communication about norms in family conferences, we added up the total number of clinician statements expressing norms in each conference and calculated the mean, SD and range across conferences.
Results
Characteristics of family conferences and participants
We audiotaped 73 out of 104 eligible family conferences (70% participation rate); five clinicians and 23 family members declined participation. Out of the 73 conferences, 71 contained discussion of treatment options. We excluded the two that did not from subsequent analysis. Family conferences averaged 35 min in length (range 10–105 min) and occurred on average 10 days (range 0–56 days) into the ICU admission, and 25% occurred within the first 48 hours of ICU admission.
The study included 71 patients, 159 surrogates and 54 clinicians (see table 1). Most participating clinicians were attending physicians, while one-third were residents or fellows. Roughly 60% of surrogates were female. Nearly 80% were patients’ family members, most commonly their children. They were racially and ethnically diverse. Seventy-three percent of patients died during the hospitalisation.
Patient, surrogate, clinician and family meeting characteristics
Communication about the surrogate role
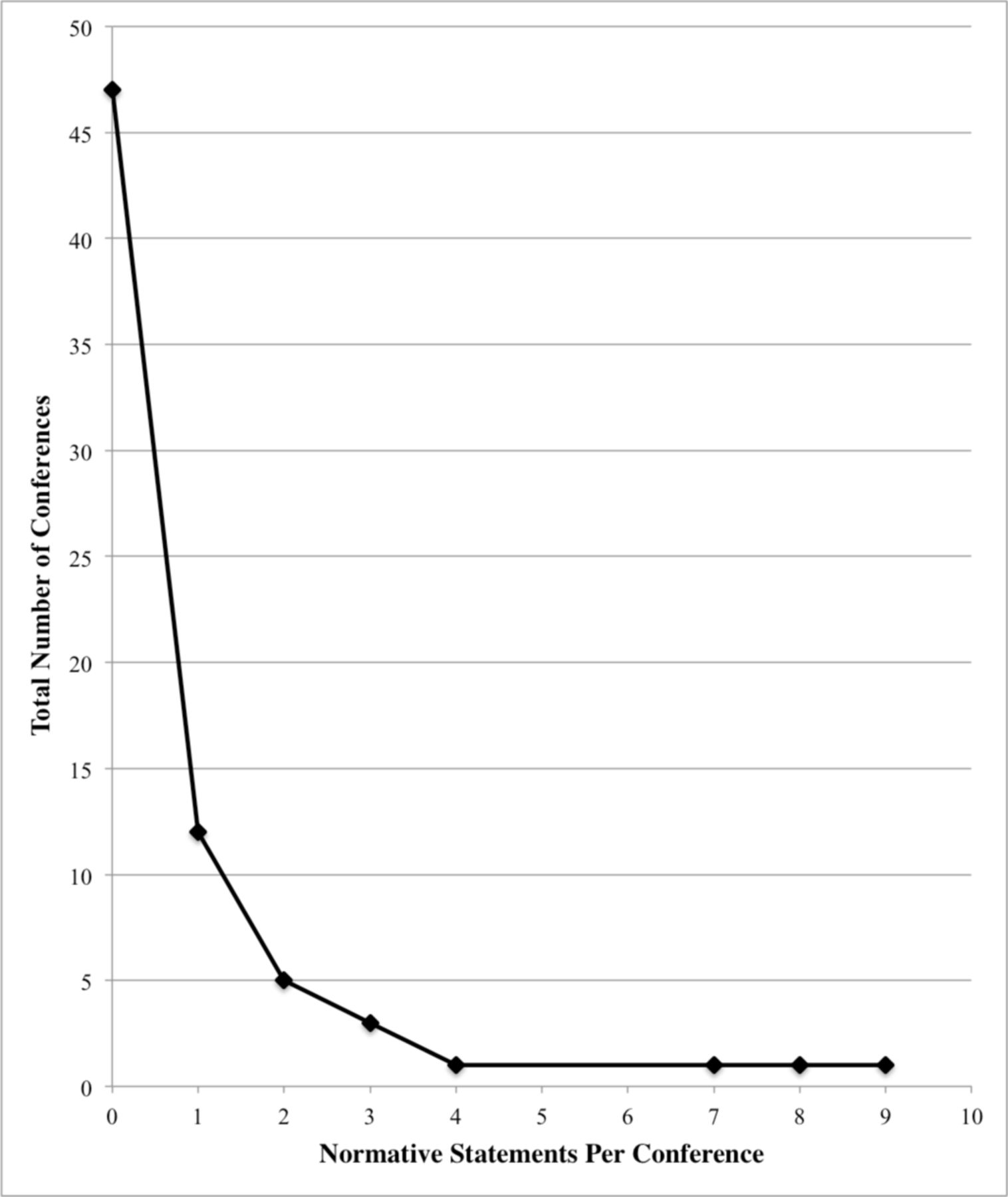
In 47 (66%) conferences, clinicians did not make any statements to family members about how to function in the surrogate role (table 2). Clinicians made at least one statement to family members about how to make decisions for an incapacitated loved one in 24 (34%) conferences. Clinicians averaged 0.83 statements (SD 1.77, range 0–9) to family members about the surrogate role per conference (figure 1). When clinicians discussed the surrogate role with family members, we observed three different types of normative statements about surrogate decision-making: clinicians counselling about one or more of Buchanan and Brock’s principles of surrogate decision-making; clinicians providing general advice to focus on the patient as a person without specifying how to operationalise this; and clinicians counselling to focus on family member interests when making decisions (table 3).

{kind=link}
Clinician statements about the surrogate role per conference.
Clinician communication about the surrogate decision-making role
Frequency of clinician education and guidance about decision-making norms
Standard principles of surrogate decision-making
In 16 (23%) conferences, clinicians explained one or more of Buchanan and Brock’s standard principles of surrogate decision-making to family members. In 15 (21%) conferences, clinicians discussed only one of the standard principles of surrogate decision-making; in one (1%) conference, they discussed two of the three standard principles, and they discussed all three principles in none of the conferences. Clinicians discussed the stated preferences standard in four (6%) conferences. For example, a clinician said to the family,
“Some people, you know, state to their families, before something like this happens, you know, what they would want, in a situation like this. So, we want to get a sense of what she would want because you are the ones who could tell us that. Ok? You know, we’re always happy to proceed in a very aggressive manner, if that’s what the patient wants.”
In 13 (18%) conferences, clinicians explained Buchanan and Brock’s substituted judgement standard. In one example, the clinician said,
“But again, today, I guess our goal is to find a common ground to see where we should be and to get your input, concerning what—our goal is to see, if she could sit here right now and could speak on her behalf, you know, how would she, what would she desire for her medical care? And the people that would know her best would be you all, who are the loved ones and family members. And that’s why you guys are so crucial and so important in this process. Because we want to respect her and respect the decision that she would’ve wished and to have that kinda guidance, you know, we draw from you all. So that’s why this meeting’s very important.”
Although the best interest standard is a standard principle of surrogate decision-making defined by Buchanan and Brock, we did not observe any clinician discuss the best interest standard.
The patient as a person
In 10 (14%) conferences, clinicians made normative statements to family members that drew attention to the importance of understanding the patient as a person when thinking about medical decisions for that patient but did not directly address any of the three standard principles of surrogate decision-making. Statements of this form differ from statements explaining a standard principle of surrogate decision-making in that they lack specificity for how to make surrogate decisions. Yet, they do emphasise the importance of thinking about the patient when making decisions as a surrogate. For example, one clinician said, “And, as hard as this is, I think that we have an opportunity right now to come together and think about what she wants and to really try to make the best choices, preserving, you know, the respect for her as an individual and her desire for independence, above all.”
Family-oriented decision-making
In six (8%) conferences, clinicians made normative statements to family members that emphasised focusing on family interests when making decisions for an incapacitated patient. In these statements, clinicians also implied a norm for acting as a surrogate decision-maker, without expressly stating the norm. In such statements, clinicians vaguely referred to the importance of the family’s sentiments or thoughts about surrogate decision-making. One clinician, for example, stated, “And so the recommendation that—from our attending, and I think this is really the question. If we want to take—if it’s felt by the group, the family, that we want to sort of search for this aetiology and see if we can continue to push forward, we have to broach these issues with the tracheostomy…”
Discussion
We found that clinicians often did not provide explicit normative guidance to individuals regarding how to function in the role of surrogate decision-maker. In nearly two-thirds of the conversations, clinicians made no statements describing surrogates’ roles in decision-making. When they did discuss a surrogate’s role, we identified three different types of normative guidance provided to surrogates: educating about one or more standard principles of surrogate decision-making, providing non-specific guidance to focus on the patient as a person and guidance to consider family interests.
There are at least three potential explanations for our finding that clinicians often do not provide normative guidance about the surrogate role. One possibility is that clinicians have not received adequate training about the ethics of surrogate decision-making or how to convey this information to surrogate decision-makers. This explanation is partially supported by research on ethics education in medical school, which indicates wide variation in curriculum and disagreement over the basic aims of teaching ethics to medical students.12 A second possible explanation is that clinicians perceive talking about how surrogates make decisions to be a topic of discussion that is more likely to increase conflict, as a ‘touchy subject’, than to reduce conflict, and thus, that clinicians avoid talking about it for this reason.13 Research suggests that at least one provider on the healthcare team commonly perceives conflict during end-of-life decision-making,14 which provides support for this view. Another possibility is that clinicians may not be attuned to the complexity of the cognitive task that surrogates face when making decisions for another, particularly high-stake decisions about goals of care in advanced illness, and therefore underestimate the need for guidance on this emotionally and cognitively complex topic.
Our finding that clinicians rarely provide normative guidance to families about the surrogate role points to a potential cause of poor-quality surrogate decision-making. Explicit education about how to perform the role may benefit surrogates by providing them with a conceptual framework for organising their judgements. This ‘sense-making’ function of ethical guidance may help alleviate the well-documented stress of surrogate decision-making.15 Explaining the process of being a surrogate as one focused on the patient’s values and preferences (rather than the surrogate’s) may help create cognitive and emotional distance from the decisions and lessen the personal responsibility that often troubles surrogates around end of life decisions. Educating surrogates about the role could also have the effect of reducing how frequently surrogates exhibit biases in decision-making, such as projection biases.6 7 It is also possible that explicitly educating surrogates about the surrogate role may have negative effects, such as increasing surrogates’ distress in situations where they are asked to make a substitute judgement but perceive that they lack sufficient information about the patient to do so. Future research is needed to understand whether explicitly educating surrogates about the surrogate role impacts the psychological difficulty of deciding for others.
Our qualitative analysis indicates that there is substantial variability in whether and how clinicians provide normative guidance to families about surrogate decision-making. Across the conversations we analysed, we identified three ways that clinicians discuss the role of surrogate decision-maker. We also found that clinicians who explicitly discuss surrogate decision-making with surrogates sometimes discuss the surrogate role in two or three ways within a single conversation. This variance in language and content suggests that there may be opportunities for allied health providers to improve how they are counselling families about being a surrogate decision-maker. Little research has been performed on involving other clinicians in the surrogate decision-making process, but what has is promising. An exploratory study with 35 surrogates and 15 physicians suggested that involving a family support specialist who, among other things, educated the family about the role of the surrogate decision-maker in the ICU was perceived by clinicians and surrogates as improving communication, decision-making quality and the patient centredness of care.16
It is important to acknowledge that there have been recent calls to improve on the normative framework for surrogate decision-making developed by Buchanan and Brock. For example, one analysis proposes integrating the best interest and substituted judgement standards to create a ‘substituted interests’ model of surrogate decision-making.17 Another advocates for an ‘endorsed life’ interpretation of the orthodox view, which directs decision-makers to focus on a patient’s prior values rather than the values and preferences that patient would have articulated if they had decisional capacity.18 Others also argue for incorporating a ‘patient preference predictor’ into shared decision-making between clinicians and surrogate decision-makers to improve the fit between patient’s actual preferences and surrogate decisions.19 Our findings suggest that, regardless of the normative framework that ultimately prevails, there may be important work to be done to help clinicians develop the communication skills needed to help surrogates understand their role obligations. To put it another way, irrespective of how our best normative accounts characterise surrogate decision-making, if clinicians do not adequately explicate this guidance for surrogates, then it is not clear how normative accounts will impact actual clinical practice and improve actual patient and surrogate experiences.
This study has a number of strengths. Most importantly, we studied actual encounters in ICUs rather than hypothetical, which establishes the clinical validity of our findings. Second, audiorecording conversations allowed us to describe in detail how clinicians and family members discuss making actual decisions for incapacitated patients, as opposed to asking them to recall such conversations.
This study also has limitations. Our study design entailed that we captured only one conversation during a patient’s hospital course. Thus, we cannot exclude that communication between clinicians and surrogates about how to play the surrogate role happened during other conversations. Although this is possible, we did not find any references to prior conversations in our audiotapes. Another potential limitation involves the possibility that the family members involved in the analysed conversations differed from the person(s) who had been previously selected by the patient, which may have skewed clinicians’ communications during these important conversations. We did not assess whether the surrogates involved in these discussions were appointed by patients versus by attending physicians and so cannot assess this possibility. Additionally, while our methods permit description of clinician–surrogate communication patterns, we have no method for estimating how much conversation about the surrogate role among clinicians and surrogates should occur. We also did not measure surrogate health literacy or information comprehension. Finally, our sample was limited a single geographical area and therefore may not be generalisable to other areas with different demographic or cultural factors.
Conclusions
In conversations where clinicians anticipated discussing goals of care and treatment options with family members of incapacitated ICU patients, most clinicians did not provide normative guidance regarding how to function in the role of surrogate. When they did provide such guidance, clinicians’ statements were often incomplete and sometimes conflicted with standard principles of surrogate decision-making. Future research is needed to investigate whether explicitly educating surrogates about ethical norms for decision-making improves decision-making in practice and benefits surrogates.
References
Footnotes
Contributors Data were collected at the University of California at San Francisco (DW). Development of the framework occurred at the University of North Carolina at Chapel (LS), the University of Pittsburgh (DW and RA) and the University of Arkansas for Medical Sciences (TC). Transcript analysis and statistical analysis were performed at the University of Pittsburgh (LS and TC) and the University of Arkansas for Medical Sciences (TC). Drafting of the manuscript was performed at the University of Pittsburgh (DW, RA and LS) and the University of Arkansas for Medical Sciences (TC).
Competing interests None declared.
Patient consent Obtained.
Ethics approval IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Other content recommended for you
- Palliative care integration in the intensive care unit: healthcare professionals’ perspectives – a qualitative study
- Persistence of patient and family experiences of critical illness
- In the patient’s best interest: appraising social network site information for surrogate decision making
- Development and evaluation of a decision aid for family surrogate decision-makers for patients with acute kidney injury requiring renal replacement therapy (RRT) in ICUs: a study protocol
- Exploring the experiences and perspectives of substitute decision-makers involved in decisions about deceased organ donation: a qualitative study protocol
- Palliative care phenotypes among critically ill patients and family members: intensive care unit prospective cohort study
- Sacrifice and solidarity: a qualitative study of family experiences of death and bereavement in critical care settings during the pandemic
- Learning from stakeholders to inform good practice guidance on consent to research in intensive care units: a mixed-methods study
- Feasibility of conducting prospective observational research on critically ill, dying patients in the intensive care unit
- Palliative medicine family conferences and caregiver psychological distress during prolonged mechanical ventilation