Article Text

Abstract
Introduction Of the 40 million people globally in need of palliative care (PC), just 14% receive it, predominantly in high-income countries. Within fragile health systems that lack PC, incurable illness is often marked by pain and suffering, as well as burdensome costs. In high-income settings, PC decreases healthcare utilisation, thus enhancing value. Similar cost-effectiveness models are lacking in low-income and middle-income countries and with them, the impetus and funding to expand PC delivery.
Methods We conducted a systematic search of seven databases to gather evidence of the cost-effectiveness of PC in low-income and middle-income countries. We extracted and synthesised palliative outcomes and economic data from original research studies occurring in low-income and middle-income countries. This review adheres to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and includes a quality appraisal.
Results Our search identified 10 eligible papers that included palliative and economic outcomes in low-income and middle-income countries. Four provided true cost-effectiveness analyses in comparing the costs of PC versus alternative care, with PC offering cost savings, favourable palliative outcomes and positive patient-reported and family-reported outcomes.
Conclusions Despite the small number of included studies, wide variety of study types and lack of high-quality studies, several patterns emerged: (1) low-cost PC delivery in low-income and middle-income countries is possible, (2) patient-reported outcomes are favourable and (3) PC is less costly than the alternative. This review highlights the extraordinary need for robust cost-effectiveness analysis of PC in low-income and middle-income countries in order to develop health economic models for the delivery of PC, direct resource allocation and guide healthcare policy for PC delivery in low-income and middle-income countries.
- palliative care
- low and middle-income countries
- costs
- cost-effectiveness
Statistics from Altmetric.com
Introduction
Globally, an epidemiological transition is underway. The combination of urbanisation, improved socioeconomics and access to medical care, longer life expectancies and the adoption of less healthy lifestyles has resulted in a dramatic increase in the prevalence of non-communicable diseases (NCDs).1 The combined burden of cardiovascular disease, cancer, diabetes and chronic lung disease is rising fast among low-income and middle-income countries, where up to 80% of deaths in 2014 were attributable to NCDs.2 3 At the same time, in many low-income and middle-income countries, there continues to be a high burden associated with communicable disease (eg, HIV, tuberculosis).4 In addition, complex humanitarian emergencies, including war and displaced populations, are occurring with increasing frequency and scale and present their own challenges for palliative care (PC) delivery.5 As a result, there is a great need to expand delivery of health services in these locations, in order to provide care for all stages of chronic and life-threatening disease.
PC has proven to be an effective approach to the care of patients with life-limiting illnesses.6 7 PC offers symptomatic relief to patients with life-limiting illness, as well as psychosocial support for patients and their families, which in turn has shown to reduce abnormal grief reactions and improve bereavement adjustment.8–10 Nevertheless, globally, there are large discrepancies in PC provision; a trend that mirrors the opioid access divide (figure 1).11

Availability of opioids for pain management (2010–2012 average). Reproduced with permission of the international narcotics control board.
In addition to lack of access to opioid analgesia, other barriers to PC implementation in low-income and middle-income countries include few healthcare policies that mandate access to PC, limited PC teaching in medical education and myths and misconceptions (eg, improving access to opioid analgesia will lead to increased substance abuse).12 13 Other misconceptions include that PC is only for patients with cancer or for the last weeks of life. The recognition that patients across the spectrum of chronic disease have pain, as well as other inadequately managed symptoms, has identified the importance of PC in both high-resource and low-resource settings.14–16
The cost-effectiveness of PC in high-income countries is well documented, and the emerging favourable cost profile has been a powerful motivator to increase PC services in high-income settings.17–23 Whereas, the lack of evidence supporting the cost-effectiveness of PC in low-income and middle-income countries is a potential political barrier to access.
At present, the financial cost of incurable diseases in low-income and middle-income countries settings and within fragile health systems is poorly understood.24 However, this information is crucial for demonstrating the economic value of PC in low-income and middle-income countries which, in turn, will guide healthcare policy and support sustainability.25
Cost-effectiveness analysis (CEAs) and cost-benefit analysis (CBAs) are strategies used to compare the costs and consequences of different interventions in order to guide healthcare policy decisions on a population level. While CBAs translate consequences into a monetary value (eg, the cost of disability days avoided), CEAs use health surrogate units, for example, quality-adjusted life years (QALYs), as measures of outcome.26 Cost-effectiveness evaluations are used globally in health policy research to find ways to decrease the price of medical care without compromising quality. The results guide international and national health policy and funding and are especially useful where resources are scarce.27 With the HIV epidemic and rise in NCDs and cancer in low-income and middle-income countries, cost-effectiveness evaluations have been used to create models for healthcare delivery that inform best practices. Examples include community-based screening for HIV and tuberculosis with linkage to care, Mycobacterium tuberculosis culture for HIV-infected persons, cancer prevention and treatment and treating paediatric cancers.28–31
In high-income countries, there has been an increase in the monetary burden of illness both for individuals and society. Empirical evidence and a cost-avoidance economic model have helped to establish the cost-effectiveness of PC.18 19 Hence, the provision of PC in high-income countries has continued to grow over the last few decades for financial reasons while simultaneously improving quality of life.20–23
In the absence of PC for chronic and incurable disease in low-income and middle-income countries, uncontrolled pain and psychosocial sequelae for patient and family are common (eg, anxiety and depression). In addition, personal and societal costs accrue, sometimes insurmountably. These costs include not only direct expenses of illness such as the cost of treatments and medication but also, perhaps more importantly, indirect and often hidden costs of illness. For example, expensive travel to receive medical care, lost wages of the patient and a second lost wage of the caregiver, the sale of personal assets such as wedding gold or a family home. Furthermore, the sale of livestock and farmland, as well as pulling children from school when school fees become unmanageable, serve to decrease the future earning potential of a family coping with illness.32 33 Inherent to the design of effective, sustainable PC interventions is an enhanced understanding of the underlying health economics involved, including both direct and indirect costs of illness within fragile health systems.34
A prior systematic review by Gomes et al evaluated the effectiveness and cost-effectiveness of home-based PC largely in high-income countries and found that it reduces symptom burden for patients with cancer and also increases the chance of dying at home as opposed to hospital.35 While acknowledging that more work is needed to study cost-effectiveness, these authors concluded that their findings justify providing home-based PC for those who wish to die at home. Smith et al conducted a review of the costs and cost-effectiveness of PC and found that PC was consistently less expensive than the alternative.36 However, all of the 46 studies included in the review took place in high-income countries. To our knowledge, there have been no systematic reviews of the cost-effectiveness of PC in low-income and middle-income countries.
In this mixed-methods systematic review, we sought to synthesise the existing data on the cost-effectiveness of PC in low-income and middle-income countries so as to identify gaps in current knowledge and inform policymakers, healthcare providers and public health researchers.
Methods
This systematic review was registered with the PROSPERO International prospective register of systematic reviews. The registration number is CRD42016053665. A senior medical librarian (DH) originally searched for relevant studies in PubMed (NLM/NIH) and Scopus (Elsevier) to help determine the appropriate controlled vocabulary terms and synonymous free text words necessary to capture the concepts of PC, low-income and middle-income countries and costs. Afterwards, we used an iterative process to translate and refine the searches to create more comprehensive searches performed on multiple databases: PubMed (NLM/NIH), Ovid Global Health, Scopus (Elsevier), The Economic Evaluation Database (Cochrane Library/Wiley) and CINAHL (EBSCOHost). Original searches were conducted in Ovid Global Health and PubMed on 17 January 2017, in CINAHL and Scopus on 18 January 2017 and the Economic Evaluation Database on 24 January 2017. Databases were searched from inception to the date of search. All searches were updated on 6 July 2018. The search strategies were filtered to include only articles written in English and French, but results were not limited by study design or year of publication. Non-original research was excluded. All search strategies are available in the online supplementary appendix 1.
Supplemental material
The results of the final search were pooled in EndNote and de-duplicated. This set was uploaded to Covidence, an online software screening and data extraction tool.37 Two reviewers independently evaluated the titles (ER and OK), abstracts and full text of the eligible articles. The World Bank classification system was used to define low-income and middle-income countries.38 Monetary results are reported in US dollars. A third reviewer (KJ) resolved any discrepancies if there was disagreement between the two primary reviewers. References of the articles meeting the inclusion criteria were reviewed to ensure comprehensiveness.
ER and OK extracted and recorded study information and additional data together to summarise findings and create tables and figures. The following information was extracted and recorded in for each study: author name, journal, year of publication, location of research, number of study subjects, type of study (qualitative, quantitative, mixed methods), type of economic analysis (eg, CBA, CEA), main study outcomes and limitations. A Microsoft Excel spreadsheet was populated with this extracted information. Qualitative data was analysed by theme: the most common themes were counted and are reported in this review.
The Mixed Methods Appraisal Tool (MMAT) was used to assess the quality of included studies.39 The MMAT is a previously validated tool, designed to appraise the methodological quality of qualitative, quantitative and mixed methods studies.
Results
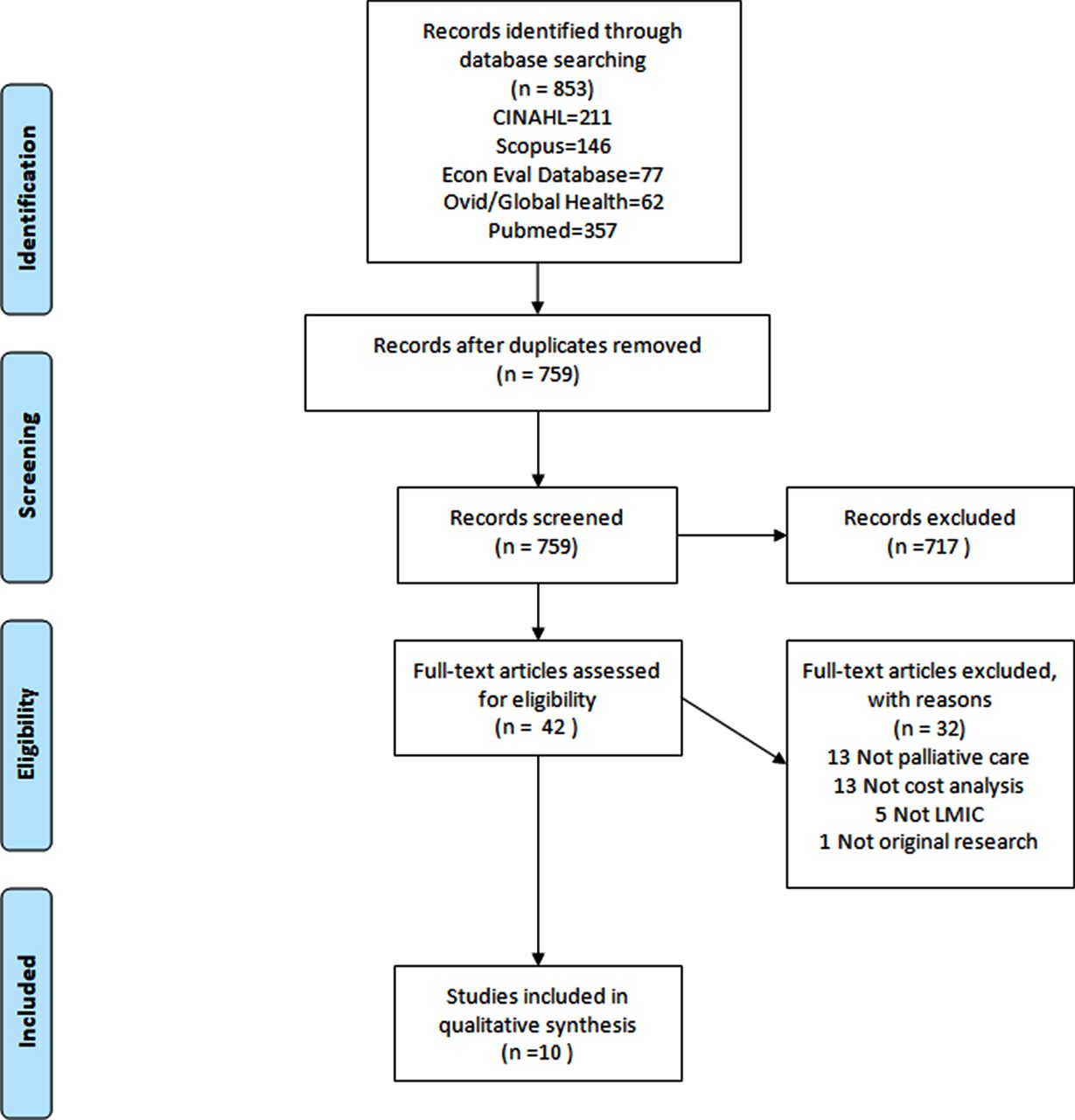
The final search retrieved a total of 853 references, which were de-duplicated to 759.
Of the 759 abstracts screened, 32 full-text articles were excluded (see figure 2 for exclusion reasons). Ten references were included in the primary analysis, of which one was a non-randomised controlled trial and nine were observational. Of the observational studies, four were purely quantitative and five contained both qualitative and quantitative methods (mixed methods).

PRISMA flow diagram.
Among the five studies in low-income countries, one was conducted in Malaysia, one in Nigeria and three in India. The five studies from middle-income countries took place in Romania and South Africa. The geographical locations of the studies included are shown in figure 3.
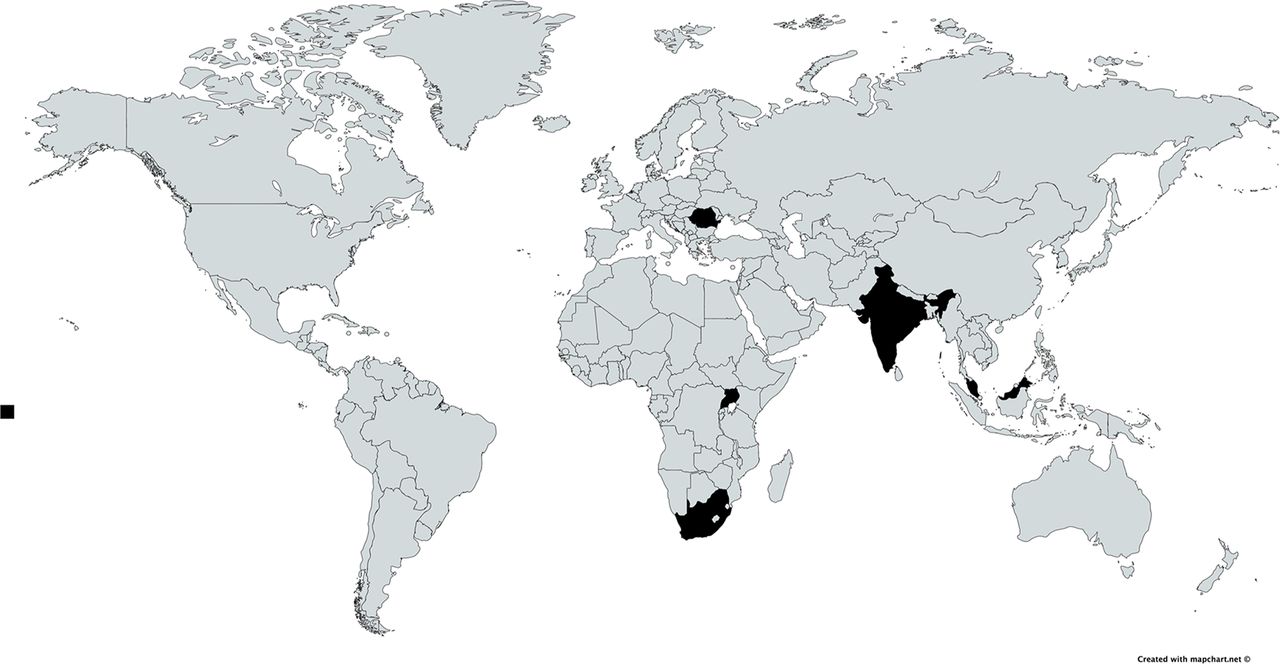
Countries included in systematic review.
The sample sizes could not always be identified. In one study, there was no data on the patient population but only information on economic outcomes (Rajagopal and Kumar40). A total of 6291 patients were included in the remaining nine studies.
Findings
A summary of the data extracted from the 10 included studies is shown in the online supplementary appendix 2.40–49 The most commonly reported economic findings were the total costs of the respective PC programmes, start-up costs and costs per patient. Hongoro et al reported the difference between hospital outreach and in-hospital PC costs per day (US$71 vs US$80) and compared this to the cost of a hospital admission (US$142 per day).44 Similarly, Mosoiu et al found that the cost of inpatient PC was US$96.58 per day versus US$30.37 for home-based care.45 DesRosiers et al compared the costs and home death rates of patients enrolled in hospital-based PC versus traditional therapy and reported decreased costs (US$587 vs US$1209) and increased home death rates in the PC group (59% vs 19%).46 Finally, Ratcliff et al demonstrated a reduction in household poverty once patients enrolled in PC and a decrease in healthcare utilisation; both of these savings increased with the length of time the patient spent enrolled in PC leading researchers to conclude that early PC further enhances poverty reduction.49 Unanimously, PC or home-based PC was less expensive than the alternative.
Supplemental material
The most commonly reported palliative outcomes included quantitative palliative outcome score or pain score (Hongoro et al 44 and Yaeger et al 47), morphine consumption indices (Devi et al 48 and Rajagopal and Kumar40) and percentage of deaths at home versus in hospital (DesRosiers et al 46 and Yaeger et al 47); in all of these studies, reported palliative outcomes were favourable when compared with the alternative.
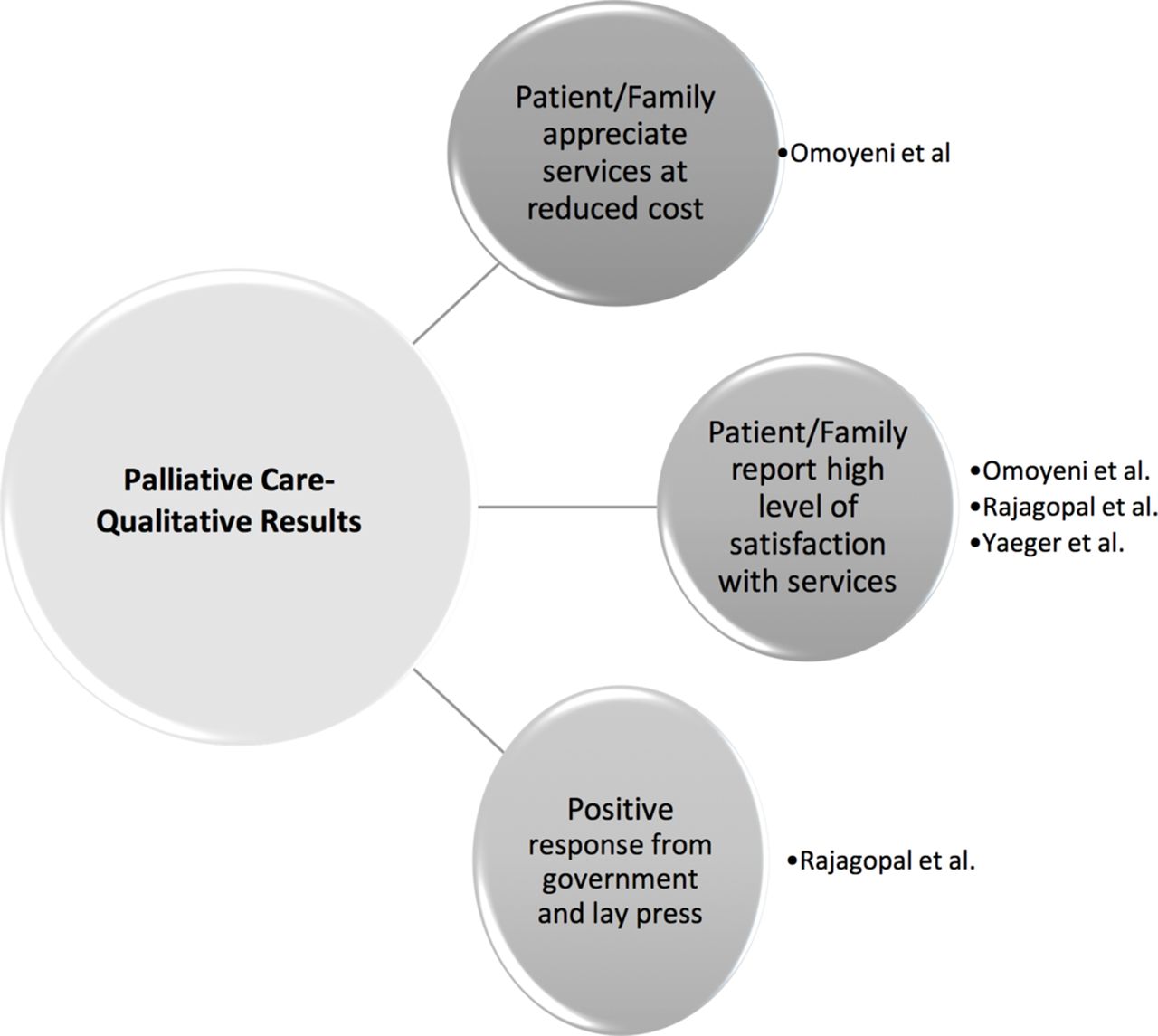
Three studies included qualitative results, which are summarised in figure 4. The most common qualitative parameters reported were patient and family satisfaction with care, appreciation of services at reduced costs and positive feedback from the local government and lay press. There were no negative qualitative results reported.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of qualitative results.
Quality
The MMAT quality assessment for included articles is shown below in table 1. In summary, of the 10 included studies, six were of high methodological quality. Overall, quality was frequently impaired by poorly defined research questions, unclear exposures and outcomes, lack of robust health economic data and lack of generalisability due to selection bias, unrepresentative samples and small sample size. For quantitative studies, lack of statistical precision and heterogeneity in comparators frequently detracted from quality. For qualitative studies, unclear sampling design and vague reporting of results most commonly marred quality.
Mixed methods appraisal tool—quality assessment
Discussion
Our extensive review of the literature found five studies assessing cost or cost-effectiveness of PC in low-income countries and five in middle-income countries. Though patient and cost-related outcome measures differed by study, all 10 of these studies reported some version of a low cost or cost-effective PC delivery. Unfortunately, the overall evidence is inadequate, due to both the paucity of studies from a small number of countries (with the exception of South Africa and Romania) and the overall low quality of the published literature on this topic.
The quality of the studies assessed by the MMAT varied: six out of the 10 studies met all criteria. However, this tool provides an overall estimate of the study of methodological quality rather than a critical appraisal of economic analysis. Four of the included studies (Mosoui et al, Hongoro et al, DesRosiers et al and Ratcliff et al) met criteria for true economic analyses in comparing two or more courses of action and considering the costs and consequences of each.26 However, cost-analysis terms were used loosely, without definition of terms and often inappropriately (eg, cost-benefit, cost-effective, cost-efficient), further adding to the confusion surrounding exactly what type of economic analysis, if any, the authors were reporting.
One explanation for the lack of true cost-effectiveness analyses in PC interventions may be the complexity of outcome measures in PC and what has been referred to as ‘the QALY problem’.50 Namely, the limitations of the more common outcome measure, QALYs, do not capture palliative outcomes or the short-term benefits of end of life care and make comparisons between PC and alternative treatments inappropriate. It has been argued that as a result of a lack of appropriate measurement tool, resources have been shunted away from PC; an alternative and supplemental measure, the Palliative Care Yardstick, has been proposed to better account for the effects of PC including the components of a good death.51 Use of better measurement tools may facilitate improved cost-effectiveness analyses in future studies and lead to improved resource allocation.
In honourable mention, two reports from Uganda were excluded due to lack of hard cost data. However, these reports provide much needed examples of a sustainable model of home-based PC delivery. In Uganda, community-based hospice care has been available since 1993, as the result of a public health approach to PC that embeds this type of PC within local health policy and delivery.52 53
In addition, several high-quality studies were excluded because they were conducted in rural or underprivileged settings within high-income countries. Namely, a study in Extremadura, Spain, provided a report of 20 years of a WHO PC demonstration project in which PC services have been integrated within the public health system, with an overall savings of €69 300 000 (€2275 per patient, representing a net savings of €16 732 000).54
In the absence of robust cost-effective models for PC delivery in low-income and middle-income countries, it may be possible to extrapolate some of the lessons learnt from existent disease models: for example, similarities exist between the chronic disease economic model and that for incurable disease. Chronic disease simultaneously destroys the internal family resources and stunts local economic growth.55 The WHO has conceded that ‘existing knowledge underestimates the implications of chronic diseases for poverty and the potential that chronic disease prevention and health promotion have for alleviating poverty in low-income and middle-income countries’. They conclude that investment in chronic disease prevention programmes is essential to reduce poverty.24 It has previously been argued that investment in PC programmes is just as essential to reduce poverty; however, as determined in this systematic review, the robust health economic data needed to translate this argument into policy is not yet available.56
Strengths and limitations
Publication bias was minimised by searching databases that included grey literature. Duplicate reports from the same PC service were excluded. Another source of potential selection bias was introduced by excluding studies in languages other than English and French. In addition to the small number of included studies and even smaller number of low-income and middle-income countries represented in this systematic review, as well as the lack of quality economic analyses, we recognise that successful and meaningful PC initiatives may be ongoing in low-income and middle-income countries, but that this work may not have been presented or accepted for publication. The results of PC efforts may be reported only to internal agencies in any individual country, which would not have been included in our analysis. Finally, the term ‘supportive care’ was not included as a search term. While distinct from PC, this inadvertent omission may have excluded studies that use the term ‘supportive care’ in lieu of PC.
Interestingly, few studies describe how selection bias was minimised in their studies. It would be important to understand how each study attempted to randomise the composition of patients who underwent PC therapy. If sicker patients with advanced terminal disease were chosen in one study and compared with a population with newly diagnosed cancer in another, there might be obvious and large differences in costs of PC, especially in studies with small sample sizes.
Given the rising burden of cancer and other NCDs in low-income and middle-income countries and the resultant increasing need for incorporation of sustainable PC services into the public health system in these settings, it is remarkable that this review revealed an evidence base of only 10 studies, with notable methodological weaknesses including a lack of comparator and a range of incompatible cost definitions. The time is right to focus on sustainable health policy to care for adult and paediatric patients at all stages of chronic and incurable disease, including PC. There is a tremendous need for robust cost-effectiveness analysis of PC delivery in low-income and middle-income countries, especially given the success and known cost savings of PC implementation in high-income countries and more importantly perhaps, in rural, limited-resource settings within high-income countries (eg, Extremadura, Spain). Future studies must assess the microeconomic effects of PC implementation in low-income and middle-income countries by examining the scope and impact of cost savings at the individual, family and local community levels. This can be achieved by assessing both direct and indirect informal costs of illness (eg, sale of major assets, lost wages, costs of transportation to receive medical care), the latter of which are especially important sources of poverty in low-resource settings and are not captured in traditional cost-effectiveness analysis.
Conclusion
Despite gaps in hard health economic data on PC delivery in low-income and middle-income countries, the included studies report a variety of methods for low-cost delivery of PC in challenging settings. Although it is difficult to put an actual economic value on the relief of human suffering, this financial estimate is necessary to promote the expansion and sustainablity of PC services in low-income and middle-income countries. Demonstrating the economic value of PC in low-income and middle-income countries, through the development of a health economic model for delivery, is key. This, in turn, is crucial to guide healthcare policy and gain momentum for increasing government sponsored, locally run PC services.
Acknowledgments
The authors are indebted to Alison Brown for her excellent technical editing, language editing and proofreading.
References
Footnotes
Contributors ER conceptualised the review. DH performed the searches and wrote the methods section. ER and OK screened manuscripts and extracted data. KJ arbitrated in case of discrepancies between the two reviewers. ER and OK generated the manuscript, which was reviewed by LG, SB and KJ. ER is the guarantor of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data from this study.