Article Text

Abstract
Objectives To investigate whether dying patients receiving parenteral fluids (PF) suffer from more or less symptoms than patients who do not receive PF. Today's evidence on how PF affects palliative patients’ symptoms is very scarce. Nevertheless, 40% of the patients who die expectedly in Swedish hospitals receive PF during their last 24 h of life.
Methods A historical cohort study of medical records was performed. Of the 530 patients who were reported to have died expectedly at hospital in Västerbotten county (Sweden) between 1 January 2011 and 30 June 2012, 140 cases who had received PF and 140 controls who had not received PF were identified by stratified randomisation and matched by age, sex and main disease. The groups were compared regarding documented presence of dyspnoea, respiratory secretions, anxiety, nausea and confusion during the last 24 h and the last week of life.
Results The prevalence of documented dyspnoea in the PF groups was higher than in the non-PF groups (51% vs 22% last 24 h, p<0.0001; 70% vs 45% last 7 days, p<0.001). The proportions of patients suffering from dyspnoea increased with larger administered volume. Although our main hypothesis—that the prevalence of respiratory secretions would be higher in the PF group—was not confirmed, we found a tendency in that direction (63% vs 50% last week, p=0.072). No clinically significant differences in anxiety, nausea or confusion were found.
Conclusions There is an association between PF administration and increased frequency of documented dyspnoea for terminally ill patients in their last week of life.
- Palliative Care
- Fluid Therapy
- Nutrition Therapy
- Symptom
Statistics from Altmetric.com
Introduction
When a patient's life is approaching its end due to incurable progressive disease, the oral intake of fluids and food is normally reduced. Whether these patients should receive artificial nutrition and/or hydration (ANH) has been debated for many years. The intention of palliative care is to maintain quality of life and reduce distressing symptoms. Today's evidence on how ANH affects terminally ill patients’ symptoms and their well-being is scarce,1 and it has not been possible to make general recommendations on when to give ANH to these patients.2 ,3 The limited evidence is reflected by the diverging attitudes among physicians on how ANH should be used at the end of life.4 ,5 Common arguments against ANH are increased respiratory secretions (death rattles) and prolonged dying, whereas one of the most commonly mentioned benefits of hydration is less confusion.6 As ANH support is medical therapy, its use should be as well considered as the use of other therapies. Even so, due to the lack of scientific consensus, the physicians’ decisions about ANH administration tend to depend on personal opinion and experience rather than on facts.4 ,6
The Swedish Register of Palliative Care (SRPC) is a national quality register that focuses on the care of patients during their last week of life regardless of diagnosis or place of care.7 ,8 It covered 57 000 (62% of all) deaths in Sweden 2012.7 The SRPC collects data with an end-of-life questionnaire (ELQ) completed by a physician or a nurse as soon as possible (within a week) after a patient's death.7 ,8 These data include whether the patient in the last 24 h of life received ANH, as well as data about the patient's age, sex, main disease(s), date and place of death, and whether death was expected.7 ,8 The ELQ also asks about the presence of pain, nausea, anxiety, dyspnoea, confusion and respiratory secretions during the last week.7 ,8 From 1 January 2011 until 30 June 2012, data were registered with the SRPC for 17 048 patients who had died expectedly in a Swedish hospital.7 Among these patients, 40% had received ANH during their last 24 h.7 The ANH administration frequency in Sweden during the same time irrespective of death place (n=63 313) was 14%, and among patients who died in hospice (n=7253) 10%.7 Thus, the SRPC reveals large differences in ANH administration depending on where and probably by whom the patient was treated, a difference possibly due to a lack of consultative palliative teams in hospital care. These data indicate there is a definite need for guidelines on when ANH should and should not be provided.2 ,3 ,5 To accomplish an evidence base for such guidelines, more research is needed to examine what impact ANH has on these patients’ symptoms.1–4 ,6
The purpose of this study was to study the association between the provided parenteral volume and documented symptoms. To be strict, we included all parenteral fluids (PF), including drug infusions and blood products. The symptoms chosen were those reported to the SRPC except from pain, that is, dyspnoea, respiratory secretions, nausea, confusion and anxiety. Our main hypothesis was that the prevalence of respiratory secretions would be higher in the PF group than in the non-PF group and that increased volume would be associated with an increased prevalence of respiratory secretions. The study was a historical cohort study based on information from patients’ medical charts.
Materials and methods
Patients
The 530 patients who were reported to SRPC to have died expectedly in a hospital in the Västerbotten county (Sweden) between 1 January 2011 and 30 June 2012 constituted the main population of this study. Using stratified random sampling we formed two groups: one with patients who were registered to have received ANH and one with patients registered to have not. The patients included in each group were matched by age, sex and disease (cancer, heart disease and lung disease) based on information gathered from the SRPC. The sample size needed to detect differences with an 80% power, with a significance level of 0.05 in two-sided tests, was calculated. According to the SRPC, the prevalence of respiratory secretions in this patient group (n=530) was 58%.7 If the clinically relevant difference between the cases and the controls were at least 18%, the required group size would be 120 patients. To cover up for any technical or sampling problem that would necessitate patient exclusion, the final number of patients was set to 140 per group (figure 1). Sampling and matching was performed by a professional statistician (BT).

Flow chart describing the exclusion of patients and formation of PF and non-PF groups. 1SRPC, Swedish Register of Palliative Care. 2PF, parenteral fluids (including clear liquids, nutrition solutions, drug infusions and blood product transfusions). 3Including the 120 patients who did receive PF during the last 24 h of life.
Methods
The patients’ (n=280) medical charts were analysed by the author for the following information to complement the limited data extractable from the SRPC.8
-
Received volume. It was registered whether the patient had received PF during the last 24 h and the last 7 days of life. Administered volumes of clear liquids (saline and glucose solutions), parenteral nutrition, blood products (erythrocytes/thrombocytes/plasma) and drug infusions were noted separately. Drug infusions containing ≥100 mL liquid per dose or ≥10 mL/h with a total volume of ≥100 mL were included. The total volume given the last 24 h of life was calculated. In addition, the administered total volume and the average daily (24 h) volume for the last week was calculated. For patients treated in hospital <7 days before death, the length of stay was registered in hours and the administered average 24 h volume during the stay was calculated.
-
Presence of symptoms. Medical and nursing records were searched for documentation of nausea, anxiety, dyspnoea, confusion and respiratory secretion. Different wordings were accepted for each symptom, and included and excluded terms were noted during the whole study. ‘Hard to breathe’, ‘feels like he doesn't get enough air’ and ‘air hunger’ were all counted as ‘dyspnoea’, whereas objective signs such as ‘sounds obstructive’, ‘tachypnoea’ and ‘low oxygen saturation’ were not included. The same principle was applied for all symptoms. For nausea, the only included term used was nausea, and expressions such as ‘sudden vomit’ were not counted. For respiratory secretions, the expressions ‘bubbly breathing’ and ‘mucous in airways’ were included, but ‘lots of mucous in mouth’ was not. ‘Hallucinations’ and ‘doesn't know were he/she is’ were counted as confusion, whereas ‘feels worried’ and ‘motor anxiety’ were counted as anxiety. Health personnel did not know which group the patients were in while registering symptoms.
-
The therapy interventions made to alleviate symptoms. These included the administration of drugs, including oxygen therapy, given with the intention to treat any of the five symptoms analysed. If the patient had received oxygen therapy, it was noted whether a low (<90%) saturation was measured and documented.
When reading medical charts it was also noted whether a treatment-limiting decision was documented by a physician, as well as if the patient died in an intensive care unit (ICU).
Patients who had a length of stay <24 h and/or had been deeply sedated during the last 24 h of life were excluded.
As the medical records were decided to give the most valid information, new PF and non-PF (have not received any clear liquids, parental nutrition, blood products or drug infusions) groups were formed according to the information gathered from the medical records of each patient: two groups representing the last 24 h, and two groups representing the last week of life (figure 1). The patients were also divided into five groups depending on their received volume during the last 24 h and five groups depending on their received average daily volume during the last week. The volumes defining these groups were (in millilitres): 0; 1–500; 501–1500; 1501–2500 and >2500.
Statistics
Statistical comparisons between groups were made with the Pearson χ2 test, univariate logistic regression and the non-parametric Mann–Whitney U test, in Statview V.5.0. ORs are presented with 95% CI. Statistical trends were tested with linear-by-linear association tests in the Statistical Packages for the Social Sciences (SPSS), V.19.
Results
Description of population
Of the 280 included patients, 29 patients were excluded due to non-existing data, length of stay <24 h and/or continuous deep sedation (figure 1). The excluded patients differed significantly from the included with respect to sex (men: n=21, 72%; women: n=8, 28%) and length of stay (median 1 day), but not with respect to age or main diagnoses.
The PF and non-PF groups formed according to data from medical records exhibited no statistically significant differences in age, sex or diagnoses, although the PF groups had a significantly shorter median length of stay as well as a significantly higher proportion of patients who died in an ICU (table 1).
Patient characteristics in the PF* and non-PF* groups formed according to information from the medical charts
Among the patients who did not receive PF during the last 24 h (n=131), 58 (44%) did not receive PF during the last week.
For 233 (93%) patients, a physician had documented a treatment-limiting decision saying ‘no cardiopulmonary resuscitation’, ‘no invasive respiration therapy’ and/or ‘strict palliative care’. The proportion of patients with a treatment-limiting decision did not differ significantly between the PF and non-PF groups (table 1).
Volumes and kinds of fluids
Clear liquids were the commonest fluids administered during the last 24 h (median 1.0 L, IQR 1.0) as well as during the last week of life (median 5.0 L, IQR 7.6; table 2).
Declaration of administered volumes, kinds of fluids and volume groups in the PF* groups representing the last 24 h and the last 7 days
Parenteral nutrition was provided to 24 patients (20%) in the PF group representing the last 24 h, and to 46 (24%) in the PF group representing the last week (table 2). Among all 251 patients, 49 (20%) received blood products during the last week and 17 (7%) during the last 24 h. Two of the 49 patients who received blood products during the last week received only thrombocytes, whereas 43 (17% of our 251 patients) received erythrocytes. The drug infusions provided to the patients were antibiotics, albumin, paracetamol, etc. None of the maximum total volumes were provided to a patient who died in an ICU.
Symptoms of interest
Comparisons between the PF and non-PF groups showed statistically significant higher prevalence of documented dyspnoea in the PF groups in all comparisons (51% vs 22% last 24 h, p<0.0001; 70% vs 45% last week, p=0.0005; table 3).
Absolute and relative frequencies of symptoms in the case and control groups
The ORs calculated regarding dyspnoea in the same groups were 3.6 (95% CI 2.1 to 6.3) last 24 h and 2.9 (1.6 to 5.2) last week.
In some comparisons, the PF groups presented a statistically significant higher prevalence of confusion and respiratory secretions, but no differences regarding anxiety or nausea were found (table 3).
The proportion of patients suffering from dyspnoea was larger with increasing received volume (p<0.001, figure 2). Analogous trends were seen neither in respiratory secretions nor in confusion.

Proportion of patients suffering from dyspnoea in relation to received volume. *Number of patients in volume groups representing last 24 h of life. **Number of patients in volume groups representing daily volume last 7 days of life.
Oxygen therapy was provided to 152 (79%) of the cases and to 27 (47%) of the controls during the last week (p<0.0001). Comparisons between volume groups showed an increasing prevalence of both oxygen use and documented low (<90%) saturation with increasing received volume (p<0.001; figure 3). The usage of opioids and diuretics against dyspnoea during the last week did not differ significantly between the PF and non-PF groups or between volume groups.

Oxygen therapy and low oxygen saturation (<90%) in relation to received mean volume last 7 days.
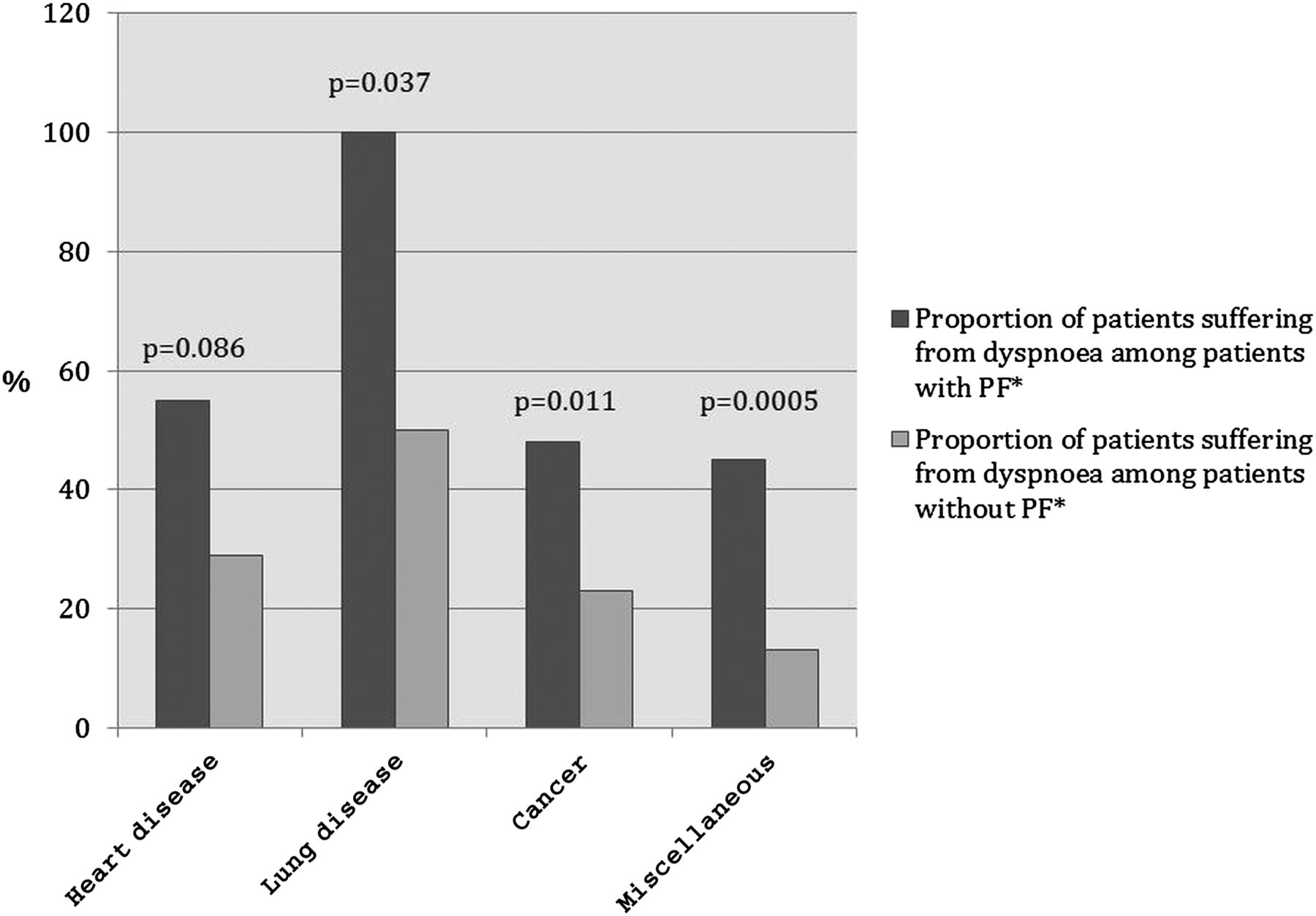
When the patients were subdivided by main diagnosis and comparisons were made between the PF and non-PF groups in each subgroup, there was a higher prevalence of dyspnoea in the PF groups in all diagnosis groups with statistical significance in all groups except in heart disease (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Subgroup analysis based on diagnosis group. Comparisons were made between each PF* and non-PF* group representing the last 24 h regarding the presence of dyspnoea during the last 24 h. *PF, parenteral fluids, which include clear liquids, nutrition solutions, drug infusions and blood products.
Discussion
This study has shown an association between provided PF and documented dyspnoea for patients treated in hospital during their last days or week of life. Although our main hypothesis—that the respiratory secretion prevalence would be significantly higher in the PF group—was not confirmed, the results indicate a tendency in that direction. We found no differences regarding anxiety and nausea, and the confusion prevalence was too low to make our results conclusive. The very few previously performed original studies on this subject have often focused on clinical signs of dehydration or overhydration, such as sunken eyes or peripheral oedemas, rather than on the patients’ symptoms.1 In addition, these studies were often conducted on a selected patient population, most commonly in patients with advanced cancer.1 ,9 In our study, we tried to focus on the subjective symptoms reported, and our patient population was not limited to any specific disease. Therefore, our results could be of interest to a broad group of clinicians.
Studies have previously shown artificial hydration providing frequencies varying from 10% to 88% in hospital settings in the last week of life.1 Before beginning this study, we knew that 40% of the patients who die expectedly at hospital in Sweden receive ANH during their last 24 h.7 To our knowledge, no previous study has thoroughly examined the total volumes provided to these patients or identified the kinds of fluids administered. Our patients’ volume ranges are to us surprisingly wide (table 2). That clear liquids would be the dominant contributor to the volumes was expected, but we did not expect that some patients would receive many litres of fluids from drug infusions and/or blood products. At the same time, many patients received no PF at all during the last week. Certainly, these variations could be due to the patients being in different stages of their illness, and some of the drug infusions may have been necessary for the patient. However, all the included patients’ deaths were reported to be expected and 93% of these had a documented decision on treatment limitations. These data provide credence to the assumption that the patients were in a stage of disease where end-of-life care was appropriate. In an earlier phase of disease, the median administered volume of 1 L/day (and no oral intake) will not be volume loading; it will rather cause dehydration. Whether this is applicable in end-of-life care is to our knowledge not sufficiently studied, and our study can also not be used to answer that question as it was not set up to study the response to adequately titrated volume replacement.
When forming our case and control groups, we had to decide what volume limits to use. Some patients in the PF groups had received only 0.1 L, which has been used as placebo in other studies. Although we have decided to put all patients who have received at least 100 mL/dose fluid intravenously in the intervention group, and, for example, in figures 2 and 3, we can see that with respect to dyspnoea the results differ between patients with no PF and those with 0.01–0.5 L.
Authors have previously suggested that terminally ill patients do not benefit from receiving artificial nutrition.10 In our PF group, 24 (20%) patients received parenteral nutrition during their last 24 h (table 2). This could be interpreted as a sign of ambivalence on the behalf of the physician in charge or that the medical assessment that death is imminent and unavoidable was made rather late. A previous study has examined the effects of blood transfusion in terminally ill patients.11 According to their results, blood transfusions for anaemic patients <4 weeks before death do not improve subjective well-being.11 That 43 (17%) of our patients received erythrocytes during their last week is possibly explained by the ambivalence mentioned above, but this finding is worthy of further reflection.
A previously made randomised controlled trial that studied all five symptoms included in our study did not find any significant differences between hydration (1 L/day) and placebo (0.1 L/day) groups when studying each symptom individually.12 That our results are inconsistent with theirs is possibly explained by our larger study groups, different patient population and that many of our patients received larger volumes.12
We have found one more previous study that used dyspnoea (respiratory distress) as an outcome when studying hydration therapy in palliative patients.13 In that study, no statistically significant difference in respiratory distress was found between patients receiving small (<1 L) and large (>1 L) daily volumes of fluid in the last weeks of life.13 Our results are not consistent with theirs, but the differences are also probably due to different research methods (eg, their study group did not have a matched control group).13 We found a strong association between PF administration and documented dyspnoea (table 3). This association is strengthened by the increasing relative frequency of dyspnoea, documented low (<90%) oxygen saturation and patients needing oxygen therapy in relation to a larger received volume (figures 2 and 3). The association is also supported by the fact that the subgroup analysis showed the differences being in the same direction and almost of same size in each diagnosis group (figure 4).
Because increased respiratory secretions have been one of the main arguments against providing PF to dying patients,5 ,9 ,14 we based our power calculations on the reported prevalence of respiratory secretions. Previous studies have found a tendency of higher prevalence with more hydration.13 ,15 Our results are in accordance with those; the prevalence was higher in the PF groups for all time frames, although significant only when comparing PF administration the last week with symptom for the last 24 h (table 3).
One of the commonest arguments favouring hydration therapy in end-of-life care is reduced confusion/delirium,9 ,14 ,16 an argument supported by the results of two studies.13 ,17 One of these studies used an intervention including both hydration and opioid rotation,17 and the other compared a small volume with a large volume group.13 Another study found that delirium could be reversed with hydration when using univariate analysis but not when using multivariate analysis.18 Three other studies did not find any difference in delirium or hallucinations outcome.19–21 In conclusion, previous studies have shown diverse results. Our results show a statistically significant lower prevalence of confusion in the non-PF group during the last 24 h, thus opposing the common argument described above. However, when studying the last week, we did not find any statistically significant differences between groups with respect to confusion prevalence. The prevalence during the last 24 h was so low (n=15 in the PF group vs n=3 in the non-PF group) that the clinical significance of the found statistical difference must be questioned. In addition, our prevalence of confusion for the last week of life was 29%–30%, a rather low proportion compared with other studies.22 Therefore, our study does not provide any definite conclusions regarding the effects of hydration on confusion prevalence.
A previous study found that terminally ill patients with advanced cancer receiving artificial hydration during a 48 h period had decreased nausea.19 At the same time, an often-mentioned burden of artificial nutrition is increased nausea/vomiting.23 Our results suggest that there are no significant differences in nausea between the PF and non-PF groups, although the prevalence was too low to make any conclusions.
A disadvantage of this study is that it is not blinded. As a retrospective study, the results also depend on the correctness of the documentation, which includes a substantial share of subjectivity as it is up to the staff when to document a symptom or not. However, no one involved in documentation was aware of the purpose of this study, and potentially biased, at the time of documentation. Furthermore, a prospective study would probably not have revealed these wide range of administered volumes. Our impression is that the correctness of the administered volumes is high as it is signed by both the prescribing physician and the nurse responsible for the administration of each unit.
Our PF and non-PF groups showed no statistically significant differences in sex, age or main diagnoses, which potentially would have been strong confounders. The shorter median lengths of stay in the PF groups are to us understandable since making the decision not to provide PF probably requires knowledge about the patient's prognosis and personal preferences. Until that information was obtained, some intravenous fluids were probably already administered. However, the shorter median length of stay could also be a result of selection bias as patients in the PF groups may have been admitted at an earlier disease stage although progressing faster to death.
More research is needed on this subject, and randomised controlled trials (RCTs) are preferred. RCTs, however, can be difficult to perform with this patient group, and observational studies are therefore also of importance.
To conclude, we have found an association between PF administration and higher prevalence of documented dyspnoea during the last week of life. There were also tendencies of more respiratory secretions in the PF groups. None of the analysed symptoms appear significantly more in the non-PF groups. These findings indicate that providing PF the last days of life may not be beneficial and it may even cause iatrogenic harm. Whether a dying patient should receive PF therapy or not therefore needs a carefully made decision, which also should be actively and regularly re-evaluated in each case. If the patient is assessed to be in an earlier stage of disease after a thorough medical examination, PF and other ‘active’ treatments are self-evident components of optimal care. Palliative care is all about optimising patients’ well-being and making the symptom burden as light as possible. We hope that this study encourages continued trials that further analyse the impact of PF on terminally ill patients’ symptoms and subjective well-being.
References
Footnotes
-
Contributors AF performed data collection, analyses of the data and drafted and revised the paper. BT was responsible for making the stratified random sampling of cases and matched controls and also assisted in statistical analysis and planning of the study. BA was responsible for planning the study and choosing study design and also made data analyses and revised the paper.
-
Competing interests None.
-
Ethics approval The study was approved by the Regional Ethical Review Board in Umeå, Sweden, 27/7/2012. Dnr:2012-217-31M.
-
Provenance and peer review Not commissioned; externally peer reviewed.