Article Text

Abstract
Palliative care (PC) has focused on patients with cancer within specialist services. However, around 75% of the population in middle-income and high-income countries die of one or more chronic advanced diseases. Early identification of such patients in need of PC becomes crucial. In this feature article we describe the initial steps of the NECPAL (Necesidades Paliativas [Palliative Needs]) Programme. The focus is on development of the NECPAL tool to identify patients in need of PC; preliminary results of the NECPAL prevalence study, which assessed prevalence of advanced chronically ill patients within the population and all socio-health settings of Osona; and initial implementation of the NECPAL Programme in the region. As first measures of the Programme, we present the NECPAL tool. The main differences from the British reference tools on which NECPAL is based are highlighted. The preliminary results of the prevalence study show that 1.45% of the total population and 7.71% of the population aged over 65 are ‘surprise question’ positive, while 1.33% and 7.00%, respectively, are NECPAL positive, and surprise question positive with at least one additional positive parameter. More than 50% suffer from geriatric pluri-pathology conditions or dementia. The pilot phase of the Programme consists of developing sectorised policies to improve PC in three districts of Catalonia. The first steps to design and implement a Programme to improve PC for patients with chronic conditions with a public health and population-based approach are to identify these patients and to assess their prevalence in the healthcare system.
- Chronic conditions
- Clinical assessment
Statistics from Altmetric.com
Introduction and background
Conceptual transitions in palliative care
Palliative care (PC) was initially developed in the British hospice movement in the 1960s, and spread into all services and countries, during which time different types of services and models of organisation were developed. PC services have incorporated conceptual transitions and identified challenges, the most relevant being to extend PC beyond cancer (table 1). In the process, there have been conceptual changes: from a disease-based approach towards the introduction of geriatric conditions and syndromes; promotion of early palliative interventions in the clinical evolution of the disease; identifying complexity versus prognosis as criteria for specialist interventions. Palliative and disease-specific treatments can be used concurrently, and are not incompatible or antagonistic. Other care innovations include the use of the comprehensive model of care and intervention, together with advance care planning and case management as core methodologies. From the epidemiological perspective, orientation has shifted from cancer mortality to all chronic conditions, and from the concept of terminal disease to ‘advanced chronic conditions with a limited life prognosis’,1 with several patterns or trajectories of progression.2 This approach supports the concept that PC measures need to be applied in all settings of healthcare systems (HCS). The population-based approach to mortality and prevalence should preferably be applied in districts or sectors3 from the public health (PH) and political perspective.4 Transitions outline needs, demands and policies for improving PC in all settings. Together with instruments to identify chronically ill patients in need of PC, the policies decided upon are key in implementing actions.5
Conceptual transitions in palliative care in the twenty-first century
Evolution of concepts of frailty, severity, progression and prognostic tools in patients with advanced chronic conditions
The criteria identifying a patient with an advanced disease combine levels of severity, progression and advanced frailty. The concept of severity depends on the criteria for every specific disease, more than on the number of comorbidities.6 Also contributing to severity are general parameters, such as functional7 or nutritional status,8 inter-current infections, and the use of emergency healthcare resources.9 Some of the geriatric syndromes such as delirium,10 dysphagia,11 sores/ulcers12 and falls13 have shown significant correlations with mortality. The criteria of progression are those aspects necessary to assess the evolution of disease, the degree of reversibility and the response to previous therapeutic measures. Frailty syndrome has been defined as a state of vulnerability and risk of health deterioration. It has been associated with mortality, especially if advanced and progressive. Frailty is frequently associated with chronic conditions and consists of deficit accumulation, with the probability of death exponentially related to the number of deficits and their progression over time. Clinically, frailty can be identified using the Multidimensional Geriatric Assessment, a specific tool with a strong relationship with survival time.14
Identifying PC needs in populations: mortality and prevalence
The assessment of PC needs in a population can be determined using a combination of methods.15 Mortality from chronic conditions can be estimated listing the related causes of mortality. The results of this methodology show that, in high-income countries, around 75% of the population will die due to chronic conditions, with a cancer-to-non-cancer ratio of 1 : 2. Our initial estimate of prevalence was based on the assumption of life expectancy of the advanced-terminal condition of 3–6 months for cancer, and 9–12 for non-cancer; the ratio of cancer-to-non-cancer being around 1 : 6–8.
Methods and tools to identify individual patients in need of PC
There are different experiences and associated prognostic tools to identify patients needing PC measures.16 The Prognostic Indicator Guidance at the Gold Standards Framework (PIG/GSF)17 and the Scottish Prognostic Indicator Tool (SPICT)18 were designed and developed in the UK and have inspired similar tools elsewhere.
The PIG/GSF and SPICT general tools combine the perception of the different healthcare professionals (‘the surprise question’) with the wishes and preferences of patients with respect to limitations of curative therapies and insertion of palliative measures (‘the choice question’). Clinical parameters (progressive, established and persistent functional and nutritional decline), the presence of comorbidities, and the use of resources (especially emergencies) can be included as tools to identify advanced status of specific conditions (cardiac, respiratory or other). GSF implementation includes identifying patients and instigating new processes of care, education and training in the different settings, together with actions to improve quality, including setting up indicators to measure progress. Experiences of implementation of GSF, SPICT or similar tools in settings such as primary care, hospitals and nursing homes have demonstrated effectiveness in identifying patients in need, and improvements in care quality in these settings.19 The PIG/GSF and SPICT are especially useful because of their simplicity, feasibility and availability in all settings, and their usefulness in identifying patients in need of PC, especially for non-cancer conditions.
The Catalonia WHO demonstration project for PC implementation (1990–2010)
Twenty years ago, WHO, in collaboration with the Catalan Department of Health, began a WHO Demonstration Project (WHO DP) in PC, and achieved high coverage in Catalan health districts.20 One of the aspects for improvement that was identified consisted of extending early PC provision for non-cancer patients into conventional services in all settings of the HCS. The NECPAL (from Necesidades Paliativas in Spanish [Palliative Needs]) Programme is addressing this challenge as a PC public health programme.21 ,5
Aims of this feature article
This feature article describes the initial actions of the NECPAL Programme in Catalonia. The main aims are to improve the quality of PC in the region. It focuses on the early identification and improved care of patients with advanced chronic conditions in the community. We summarise the preliminary results of this Programme in Catalonia. The initial focus is on constructing the NECPAL tool (NECPAL CCOMS-ICO©) (based on the PIG/GSF and SPICT experiences, introducing other dimensions and adapted to our clinical and cultural context) to identify patients with these advanced chronic conditions (see online supplementary appendix 1). We present the preliminary results of the prevalence of these patients in the general population in the County of Osona (north of Barcelona). The current state of the Programme focuses on developing a predictive model for 12-month risk of death for patients with chronic advanced diseases and life-limiting prognosis while implementing different phases of the NECPAL Programme. Future communications will describe the end results of the prevalence study, the results of a prospective cohort study to explore the model's predictive capacity based on the NECPAL tool, and the results of the NECPAL Programme for improving PC in three pilot areas.
The NECPAL Programme
Implementation
The NECPAL Programme is implemented by the Catalan Department of Health22 within the context of the Programme for the Prevention and Care of Persons with Chronic Diseases (Programa per a la prevenció i atenció de persones amb malalties cròniques). It proposes to identify patients with an advanced chronic condition in all settings of the Catalan HCS, and activate an early palliative approach oriented towards improving the patients’ quality of life. The general aim of this Programme is to improve quality of PC in all settings of the Catalan HCS, with focus in the community.
Palliative care needs assessment
The initial steps of the NECPAL Programme have the main aim of assessing PC needs, via the framework of two research studies (PI10/01512 and 2010/PREVOsona), and consisting of three parts:
-
Part I: construction of a tool to identify patients with chronic advanced diseases needing palliative measures (the NECPAL tool).
-
Part II: determination of the prevalence of patients in need of palliative measures in the population of the County of Osona using the NECPAL tool, and to explore the prevalence in different settings of the HCS (primary care services (PCS), acute bed hospitals, social-health centres (SHC) and nursing homes).
-
Part III: exploration of the model's predictive capacity for 12-month risk of death based on the NECPAL tool, either globally or for selected chronic diseases and settings. The study is prospective in a cohort of patients with advanced chronic diseases.
The NECPAL research studies have been designed by the WHOCC at the Catalan Institute of Oncology (Institut Catala d'Oncologia) in Barcelona. They are developed jointly with primary, geriatric and palliative care healthcare professionals in PCS, at the Vic District General Hospital (DGH) (Consorci Hospitalari de Vic) and at the Santa Creu Hospital in the County of Osona. The projects are sponsored by a start-up grant from the Health Investigation Foundation (Fundacion Investigacion de Salud) of the Spanish Ministry of Health, and from the Catalan Department of Health.
Both studies have been formally approved by the ethical research committees of institutions involved in their execution (PI10/01512: PR200/10 and 2010/PREVOsona: P10/65 and EO65)
Construction of the NECPAL tool
Selection of reference tools
Following a literature review, including a revision of a similar tool tested in a Spanish acute bed hospital,23 the PIG/GSF and SPICT tools were selected for their relevance, feasibility and experience as sources from which to derive the main criteria for the NECPAL tool.
Translation
A translation into Spanish of the relevant items of PIG/GSF and SPICT was performed using a dual panel approach without back translation. Cultural and clinical adaptation, cultural understanding and appropriateness of questions in the Spanish language, and the addition of new questions relevant for Spanish healthcare professionals were taken into account. The process involved three successive rounds of adaptation (from initial translation into Spanish to the inclusion of cultural and clinical modifications).
Assessment of content validity
The proposed tool was evaluated by a multidisciplinary expert panel and included 18 semi-structured interviews (see online supplementary appendix 2). Opinions were solicited from the experts in terms of overall, and specific, appropriateness of the tool in identifying patients in need, and the comprehensiveness and feasibility within the individual contexts. Additionally, opinions were collated regarding the tool's ability to identify terminally ill status within the individual clinical specialties.
Pretest
The process of pretesting the NECPAL tool for comprehension and face validity included primary care settings in which 18 interviews were performed. Following five versions of the tools being tested (from pretest to final version), this phase concluded with the definitive NECPAL tool being put together ready for use.24
The NECPAL tool
The NECPAL tool translated into English is shown in table 2. Compared with the GSF and SPICT, the main differences are as follows:
-
The ‘surprise question’ is maintained for the next 12 months.
-
The ‘choice question’ has the concept of ‘demand’ introduced, and has been adapted to our Latin-Mediterranean cultural context in which the family members (or carers) are more involved in decision-making regarding the patient. We introduce the concept of ‘need’ for limiting therapies, or the introduction of PC, as perceived/indicated by the healthcare professional.
-
The clinical parameters had the psychosocial area (severe persistent emotional distress or adjustment disorders) introduced and the commonest geriatric syndromes (disphagia, falls, persistent pressure sores, repeated infections, delirium).
-
The combinations of the concepts of severity and progression not linked to an acute process were introduced.
-
Frailty was introduced as a general and transversal indicator.
-
The proposed parameter of resource use refers to emergency department access in the previous 12 months.
-
There are proposals to identify advanced illness status in several specific conditions.
The NECPAL tool (differences from the PIG and SPICT tools highlighted in bold)
Additionally, two further formats have been edited and adapted for different purposes,25 that is, leaflet format: designed to be easily available in clinical practice; and research version format: oriented towards studies promoting the spread of epidemiological and clinical data collection, and quality improvement in services.
The NECPAL document
A guide (termed the NECPAL DOC) has been edited to consist of the NECPAL tool, with an introduction and two additional sections: six basic recommendations for care provision for identified patients (oriented towards practical actions for patient care); and six basic recommendations to improve the quality of PC in the HCS (oriented towards implementing actions for improving the quality of PC in any healthcare service).
Determination of prevalence
The study was implemented in the County of Osona, a region of 1260 km2 located to the north of Barcelona. The mixed urban–rural population consists of 147 138 inhabitants; 21.4% >65 years of age and an overall mortality of 8.81‰. The County of Osona has a complete range of healthcare and social care resources, including 11 PCS, a DGH of 160 beds, two social health centres (SHCs) including rehabilitation, PC, long-term care and dementia-care facilities, and 22 nursing homes. It also has a comprehensive system for geriatric, dementia, palliative and chronic care. All facilities within the HCS are linked by a common computerised information system, the Osona Integrated Health System (Sistema Integral de Salut de Osona).
Sample and recruitment of services and patients
A representative random sample consisting of three PCSs stratified as urban, rural and rural–urban; the inpatient units of the acute bed hospital; one of the two SHCs; and the nursing homes registered at the PCS were selected for the prevalence study. All care centres selected (nine of nine contacted) accepted the invitation to participate in the prevalence study.
Methodologies for recruitment of patients were similar in all selected settings (figure 1). Patient recruitment was based on interviews with healthcare professionals (doctors and nurses) using all conventional clinical information available. The process encouraged enhancing/ promoting sensitivity in recruiting all patients with chronic conditions and highlighting the ‘advanced’ (or ‘severely affected’) in every disease or condition (first level). To determine the prevalence of patients with advanced chronic conditions in need of PC measures, we defined the ‘negative’ response (ie, ‘I would not be surprised…’) to the Surprise Question (or ‘SQ+ patients’) as the second level and having at least one more positive parameter (or ‘NECPAL+ patients’) as the third level.

Recruitment of patients (doctor and nurse in every setting). NECPAL, Necesidades Paliativas [Palliative Needs].
Patients are followed up for survival every 3 months for a period of 1 year. Overall mortality in the studied area is recorded and compared whether the individual had been identified, or not, in each level.
Determination of population-based/community prevalence
Prevalence was calculated from all patients recruited by the selected PCS using the SQ+ with at least one additional parameter. To this was added the number of patients recruited over the same period at the SHC, acute-bed hospital and nursing homes registered in the PCS. Once identified, the prevalence was calculated with the formula: number of patients identified ÷ the total population ÷ the adult population over 16 years of age.
The most relevant preliminary results are shown in tables 3⇓–5. The complete results are currently undergoing detailed analysis.
Preliminary results of the NECPAL prevalence study
Some characteristics of ‘surprise question’ (SQ+) patients
Distribution of ‘surprise question’ (SQ+) patients by main disease or condition
Qualitative analysis of the impact of the study conducted in PCS
In the three PCS included in the prevalence study, two focus groups of eight healthcare professionals were organised. The composition was multidisciplinary, with a conductor and an observer. The dimensions discussed included process of selecting patients; feasibility of the instrument; impact of the SQ; use of subjective and objective parameters. These sessions were followed by discussions on types of interventions for the care of the patients identified, clinical priorities, decision-making, training needs and demands. All discussions were video taped and reviewed during post-discussion analysis.
There was consensus regarding the positive influence of the NECPAL tool application and its implementation in the quality of care. The most relevant aspects were ‘sharp awareness’ of the high prevalence of these patients in primary care practices; practical feasibility; value of the surprise question as a qualitative approach which modifies personal and professional attitudes; value of the interdisciplinary approach; need and demand for education and training; need for changes in organisation of PC services and their relationship with specialist services.
Development of a predictive model for 12-month risk-of-death study
Patients from acute-bed hospitals, SHCs, nursing homes and PCS with the most common chronic diagnoses are currently being recruited into an observational, analytic, prospective cohort study to develop a predictive model for 12-month risk of death, based on identification of patients using the NECPAL tool. The model's overall predictive capacity will be studied, and segregated by disease and setting. The data will be presented in future communications.
The NECPAL Programme at the Department of Health
The initial phase of insertion of the NECPAL project into the Programme for Chronic Care at the Department of Health consisted of defining the Programme as one of the issues to be implemented within the context of the Chronic Care Programme, and the selection of three demonstration areas: County of Osona (mixed urban/rural area); Girona (urban area); Barcelona South (metropolitan area). The current process of implementation consists of developing an action plan for every area, including systematic actions (context and quantitative analysis, managerial workshop, clinical workshop, prevalence survey), implementation (clinical and organisational measures) and evaluation (establishing monitoring indicators).
Discussion
Construction and cultural validation of the NECPAL tool
The NECPAL tool has incorporated some issues to be adapted to our cultural context, such as the inclusion of the family members (and team members) in the ‘choice question’, in a paternalistic context where the patients are less autonomous and families take responsibility for information and decision-making.26 The inclusion of the combination of severe and progressive frailty is due to its high prevalence (not necessarily linked to individual diseases) and the severe psychological distress (or difficulties in adjustment to the clinical condition) based on the assumption that these dimensions are also indicators of the need for PC interventions.
Regarding the assessment of frailty, there are three significant differences between the NECPAL tool and PIG/GSF and SPICT:
-
The NECPAL tool presents frailty not as a separate clinical entity, but as a general and transversal indicator of mortality, beyond the patient's illness trajectory. This fact is related to the reality of patients at the end of life, when the most prevalent chronic situation is multimorbidity27
-
PIG/GSF and SPICT measure frailty mainly based on Fried criteria28 (weakness, slow walking speed, low physical activity, weight loss, reduced weight loss, self-reported exhaustion), basically oriented for the detection of initial/moderate frailty. For the detection of advanced frailty, which is the common path towards the end of life for many patients (especially those over 75 years), the most rational approach is based on deficits accumulation.14 Four out of the six general indicators correspond to deficits caused by advanced frailty, emphasising geriatric syndromes (with increasing evidence as an independent prognostic marker),29 and use of resources and nutritional and functional markers, as already considered in PIG/GSF and SPICT.
-
In the NECPAL tool, severity and progression criteria have been proposed as the backbone of measurement of proposed variables, including those related to the disease and, especially, when assessing general indicators, which are increasingly seen as the most reliable markers of advanced situation, especially in a ‘geriatric profile’ population,30 with a dynamic perspective, including the temporal dimension.
These changes could explain the increased length of the NECPAL tool compared with the reference ones. The preliminary results of the prevalence study emphasise the importance of including the geriatric syndromes in the NECPAL tool and actively searching for these conditions in the identification process.
Preliminary results of the population prevalence study
The sample of services and patients is representative of the county. The most striking result is the high figure obtained for overall prevalence (1.45%), possibly due to the higher proportion of older people (21.4% vs 17%) in the area, and the inclusion of advanced geriatric pluri-pathology and frail patients in the recruitment. This is reflected in a prevalence of advanced frailty and dementia >50% of SQ+ patients, and the mean age of SQ+ of >81 years. The proportion of patients with cancer is consistent with our previous estimations. The prevalence by settings (PCS, hospitals, SHCs and nursing homes) could be a local feature, and needs to be evaluated in other contexts. Most of the patients live within the community and nursing homes, and are followed up by the PCS, with few interventions by specialist services. This feature is crucial for planning and developing policies to improve PC with a PH approach. The complete results of the prevalence study and the preliminary results of the survival study are currently being analysed.
Early identification in the community
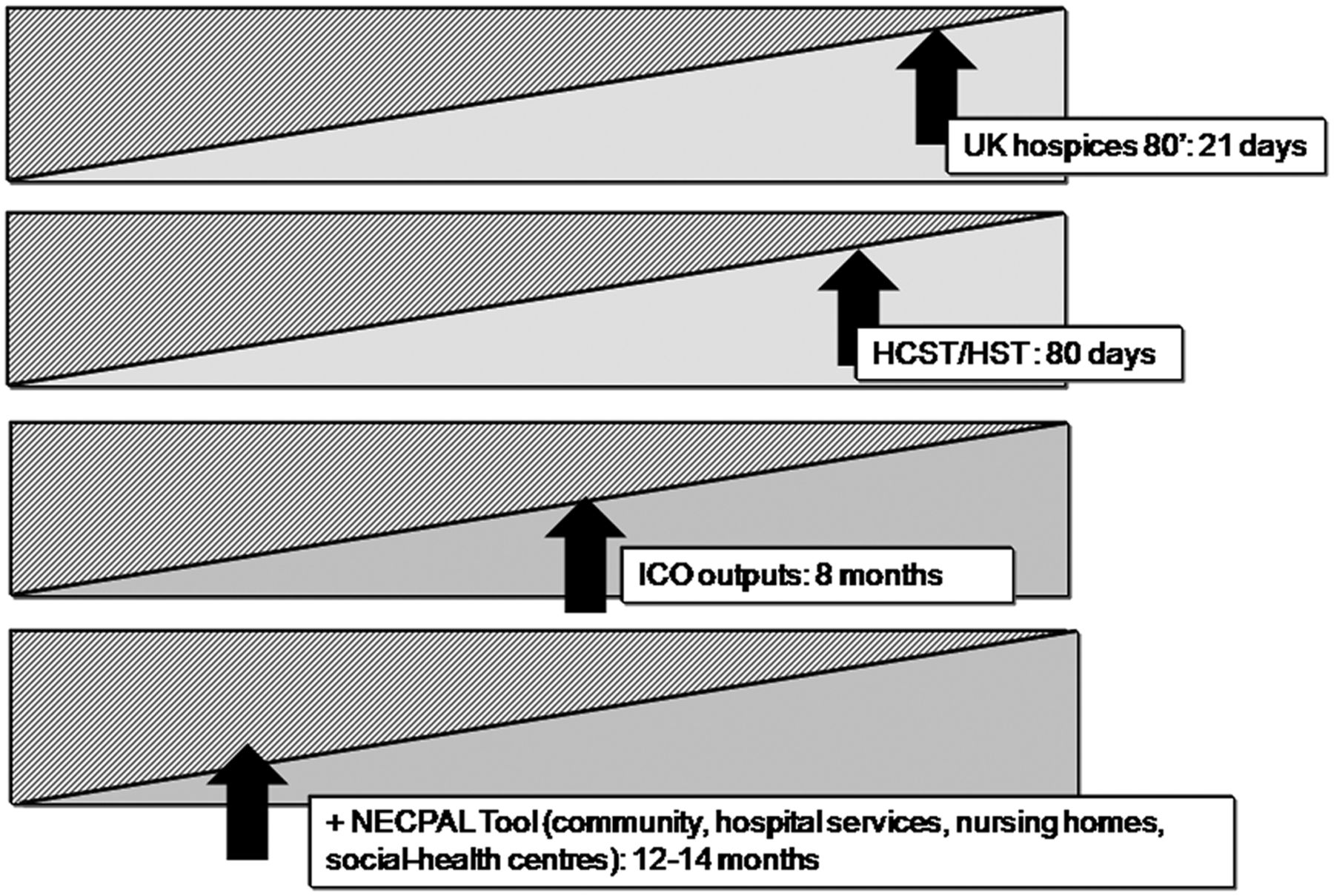
The pattern of PC of these patients needs to change towards an earlier, gradual and flexible approach in which PC and all other measures must be combined, and initiated in community services months before death (figure 2).

{kind=link}
{kind=link}
Earlier detection, longer time of intervention/survival and place and type of service of patients with palliative care needs 1985–2011. HCST, home care support team; HST, hospital support team; ICO Outpat, palliative care outpatient clinic at the Catalan Institute of Oncology; +NECPAL tool, patients identified by the NECPAL (Necesidades Paliativas) tool.
Piloting the NECPAL tool in PCS
The NECPAL tool has been considered feasible, practical and useful by primary care doctors and nurses in identifying patients with advanced conditions in need of PC measures.
The qualitative study showed that the use of the NECPAL tool has a considerable impact on the perceptions, and eventually in clinical practice, of primary care professionals, as has been observed in other experiences.31 The identification of patients, and their high prevalence in the community, produces a ‘sharp awareness’ in primary care professionals, and leads to identifying an unexpected level of needs even in the absence of demands (the ‘surprised team’). Of considerable interest is that one of the most relevant parameters in identifying patients is the ‘surprise question’ which, when contemplated by doctors and nurses, involves them more personally than other parameters or tools.
Another relevant feature is the identification of the need and demand for training of the healthcare professionals in the community to manage these patients from an early stage. The organisation and quality of the PCS need to change to adjust to the prevalence. The role of specialist services acting in the community also needs to change, especially when patients are identified earlier and, presumably, are less clinically complex.
Conclusions, recommendations and further progress
The first steps of a Programme to improve PC in Catalonia are described. Included are the construction of the NECPAL tool, the preliminary results of the prevalence study and the impact on primary care professionals.
The NECPAL tool is adapted to our (Mediterranean) cultural settings. It is feasible, and is accepted by primary care professionals. It can identify quite easily patients in need of PC measures from among those suffering from advanced chronic conditions living in the community. Identification is at an early stage and the estimated survival time is around 12–14 months. It is recommendable as a screening tool to identify these patients in primary care and also in all the conventional resources in the HCS.
The process of identifying patients has a considerable impact on primary care professionals and service providers. It increases awareness of prevalence and needs of the patients. Also highlighted is the need for specific training of the healthcare personnel and for adapting the organisation of PCS and other healthcare and social care settings to the needs of the population.
In our ongoing research studies, we are determining the prevalence of patients with PC needs in specific settings (hospitals, nursing homes, SHCs) in other districts, we are seeking to identify the most relevant clinical features, including the description of those needs, and the predictive capacity of the parameters included in the tool, so as to select the most relevant and reliable, and conducting the longitudinal study on the causes of death of the identified patients.
There is enough evidence already to recommend implementation of the NECPAL Programme in Catalonia in all services. The objective is to combine the NECPAL tool with measures that respond to the individual needs of these patients which, together with general measures, would improve the quality of PC in all settings. The sectorised approach would enhance a population-based PH vision, adapted to local needs.
Knowledge of the prevalence of patients with advanced chronic diseases with limited prognosis in need of palliative measures in populations and settings of the health and social organisations is fundamental for planning and implementing PC programmes, and measures to achieve coverage for all patients.
Limitations of this feature article
This article describes the initial actions of a Programme, including the construction and adaptation of a tool to identify patients with chronic advanced diseases in need of PC in a County within Catalonia. Also described are the preliminary results of the prevalence rates in a population-based study. These actions are the first steps (needs assessment) of the NECPAL Programme.
Although the tool is not currently undergoing a formal process of validation, there is considerable agreement among the relevant experts regarding its use. The results of the prevalence study and the qualitative survey of the focus groups reflect this agreement. The preliminary results of prevalence are derived from one specific district in Catalonia, and further studies are ongoing in other settings to evaluate the reproducibility of our findings.
Acknowledgments
Data contained in this article are drawn from studies that have been supported financially by the Spanish Ministry of Health and the Catalan Department of Health. Editorial assistance was by Dr Peter R. Turner of Tscimed.com.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors XGB conceived the study. CB, MMM, LV and MF developed the design, participated in the discussion and elaboration of the manuscript. AV and XC collected the data. CC acted as the administrative leader of the NECPAL programme. All authors revised and edited the paper. XGB is the guarantor.
-
Funding The development of the NECPAL tool was funded by the Instituto de Salud Carlos III (grant number: FIS PI 10/01512) which is a research funding arm of the Spanish Ministry of Health. The prevalence study of patients in need of palliative measures in the population of the County of Osona was funded by the Catalan Department of Health. Both funding bodies had no involvement in the study design or in the collection, analysis and interpretation of data, or in the decision to submit the manuscript for publication.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.