Article Text

Abstract
Introduction If palliative care is to lead the way towards a new model for integrated care, the ability to share information across the whole of health and social care is essential. Coordinate My Care (CMC) is a service dedicated to preserving dignity and autonomy at the end of life. Its care pathways enable health professionals from primary and secondary care to put the patient at the centre of health care delivery. This service is underpinned by an electronic solution. The CMC record can be accessed 24/7 by all health and social care professionals who have a legitimate relationship with the patient.
Patients and methods The record displays diagnosis, prognosis, advanced care plan, resuscitation status and patients wishes for end of life care patients across London. This article is a review of CMC use and outcomes from August 2010- March 2012.
Results 1087 CMC patient records were analysed. The primary diagnosis was non-cancer in 52.3%, cancer in 46.3% and unknown in 1.4%, 42% of all patients were cared for by generalist only and had no specialist palliative care involvement. At the time of analysis 207 had died. Actual place of death was home 38.6%, care/nursing home 16.4%, hospice 12.1% and 30% in hospital. This equates to 55% of patients dying in their usual place of residence and reflects that 70% died outside of hospital.
Conclusion The CMC service has a well defined pathway underpinned by an electronic solution. It has been shown to change culture and deliver fully integrated, personalised end of life care. A pan-London CMC roll out will take place over the next 12 months.
Statistics from Altmetric.com
Introduction
If palliative care is to make a giant leap, and lead the way towards a new model for integrated care, the ability to share information across the whole of health and social care is essential. The ability to capture and, crucially, share information across all facets of the patient pathway is a fundamental requirement that underpins any aspiration to forge a sustainable model of integrated palliative care. There has been much talk in recent months of the concept of the so-called ‘disruptive technologies’—the notion that something very simple can transform the way we do things and, at the same time, make the process more efficient. The term is used to describe innovations that improve a product or service in ways that were not expected.1 The consumer world is full of examples of disruptive technologies that were dismissed when they were first introduced but have gone on to become an essential way of life. Automated teller machines (ATMs) are a perfect example.
In England, the End-of-life Care Strategy highlighted the national agenda to improve care for patients, irrespective of diagnosis, during the last year and ultimately at the end of their life. We know that the majority of people would prefer to be cared for and ultimately to die at home.2 ,3 However, 2 years on from the introduction of the End-of-life Care Strategy and despite over £286 million of investment, in the UK 53% of deaths still occur in hospital.4
The National Health Service (NHS) needs to make unprecedented savings in the next 5 years and more care is being shifted into the community setting which is in line with the end-of-life care agenda. Current plans to merge hospitals will not automatically lead to efficiency savings, and ongoing financial constraints can no longer only be met by treating more patients while trying to cut costs. The DEMOS report5 on UK end-of-life care published in 2010 highlights this and advocates that services should be commissioned by end-of-life trusts in an integrated way that bring together public, private and voluntary providers within a community. Blank and Van Hulst6 assessed the impact of 63 groups of healthcare innovations and found that only one—the adoption of information and communication technology for hospital processes—both saved costs and led to statistically significant efficiencies. In the current climate, new technology holds the greatest potential for increasing productivity. We believe that the availability of cost-effective affordable technology and its integration into patient care will be crucial in facilitating coordination and delivery of high quality end-of-life care.
At the moment, palliative patients with complex needs are cared for by multiple service providers. In addition, there is no consensus between geographical areas in the way key services are provided, with delivery by different professionals or organisations and effectively a postcode lottery for care. The mismatch of the needs of patients with individual services is enhanced by poor coordination across different settings, resulting in huge frustration for patients, service users and carers. The disproportionate access to scheduled (within working hours) and unscheduled (out-of-hours (OOH)) care for these patients remains a key challenge given that their health needs are often rapidly changing. It is recognised that ‘achieving integrated care would be the biggest contribution that health and social care services could make to improving quality and safety’.7 For palliative patients, who by definition have a limited prognosis, there is some urgency to address issues and make real changes to meet individual needs.
Patients with complex needs, particularly at end of life, should be entitled to an agreed care plan, a named key worker responsible for coordinating care and access to the benefits that modern technology can provide. This concept is the basis of previous initiatives such as the Gold Standards Framework. The UK end-of-life care Quality, Innovation, Productivity and Prevention initiative work stream aims for cost savings in end-of-life care by concentrating on identifying people who are approaching the end of life and planning for their care in their preferred place.4
Our priority is to provide integrated health and social care both for individual patients and at a population level, by bridging the divide between community and acute care settings, with integration of the voluntary sector who remain key providers in end-of-life care. The challenge is to improve patient outcomes by working together—different professionals in different settings—providing a seamless and patient centred cost-effective service. A recent report by the Kings Fund to the Department of Health and the NHS Future Forum suggests that integrated care can be delivered without further legislative change or structural upheaval and that the aims of integrated care are widely supported by NHS staff as well as patient groups and key stakeholders.7
Something fundamental needs to change to move this forward and we propose that the adoption of a disruptive technology to revolutionise care is a promising way forward. The Department of Health has supported the development of locality end-of-life care registers called Electronic Palliative Care Co-ordination Systems (EPCCS). We have developed the EPCCS into a multi-professional service called Coordinate My Care (CMC). This review outlines the progress from inception, development and piloting of the CMC Programme which is now being rolled out across London.
What is CMC?
London has an estimated population of 7.8 million people, with 31 primary care trusts (PCTs), 34 acute/specialist trusts, 14 inpatient hospice units and three mental health trusts. CMC is a service dedicated to preserving dignity and autonomy at the end of life for all patients across London. In line with the dying matters ‘find your 1%’ campaign8 if all end-of-life patients are correctly identified and given a CMC record this will equate to approximately 78 000 patients across London. CMC's care pathways enable health professionals from primary and secondary care to put the patient at the centre of healthcare delivery at this most sensitive time, together with their carers. The service focuses on working with patients and families to understand their wishes and preferences for place of treatment and death, and ensures that this is honoured, even when the instinct is to elevate the (unwanted) level of care. Its aim is to provide better coordinated services by improving communications between hospital and community teams. The teams are joined together through CMC to deliver the care that is designed specifically for each individual patient9 (figure 1).

The Coordinate My Care approach. GP, general practitioner; PCT, primary care trust.
This service is underpinned by an electronic solution (figure 2). The Scottish Supportive and Palliative Care Indicator Tool (SPICT) aids the identification of patients.10 A CMC record is then created at this point when the patient is identified as being in the last year of life. The record is electronic and displays the patient's diagnosis, prognosis, current problems, anticipated problems, advanced care plan, resuscitation status and patient's wishes. All patients prospectively consent to having their details added to CMC. If patients do not have capacity they may be added ‘in best interest’. The CMC record can be accessed 24/7 by all health and social care professionals who have a legitimate relationship with the patient. The information technology (IT) solution is a central password protected web-based record accessed through a secure N3 network allowing professionals access to only that information which is relevant to them and their geographical areas of work.9 One reason for choosing a web-based solution is to allow future development to incorporate access to CMC through a wide range of configured hand held devices, with the potential to revolutionalise community care.
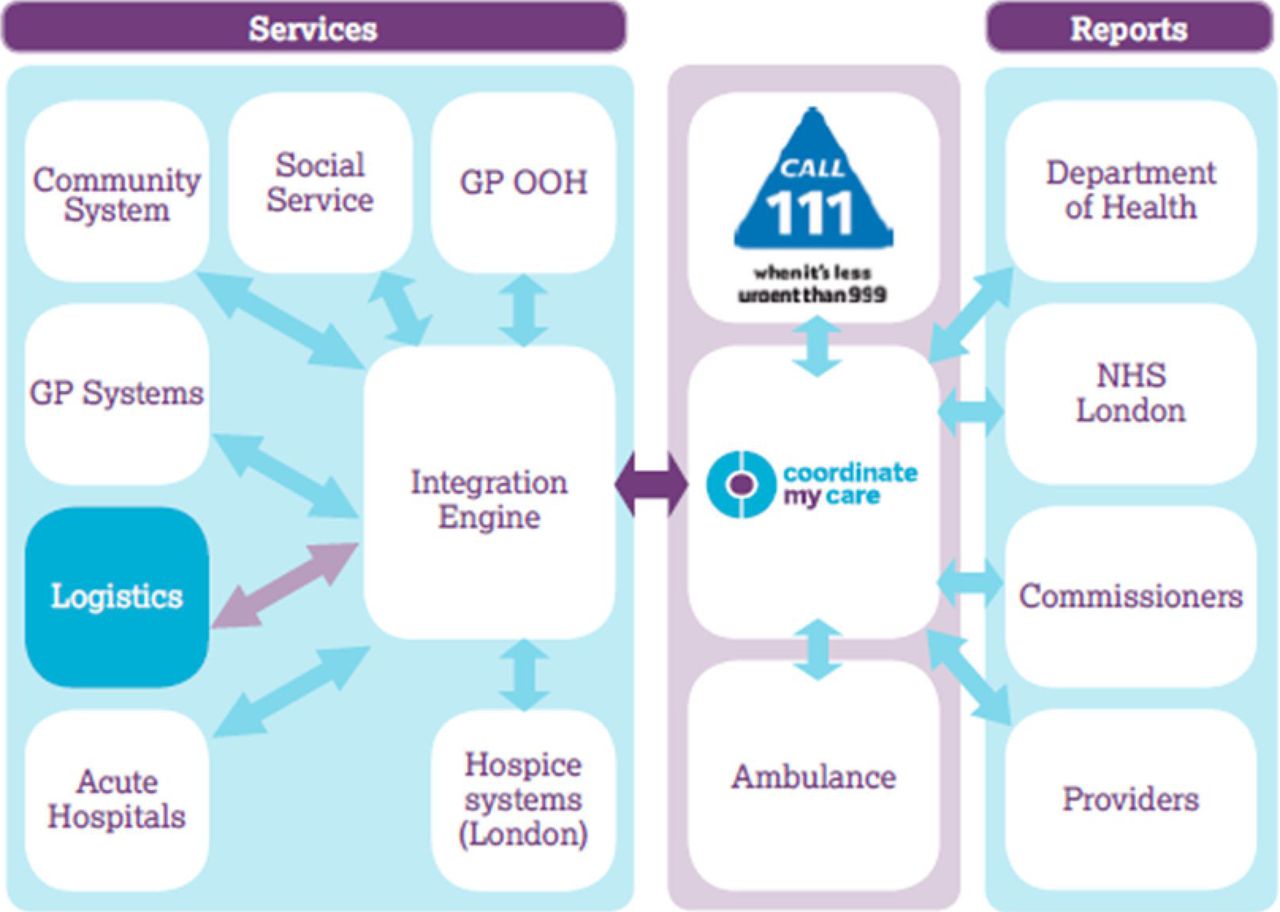
Diagram of Coordinate My Care integration with service providers (9) (logistics still to be added). GP OOH, general practitioner out-of-hours; NHS, National Health Service.
CMC integrates end-of-life care pathways across London between health and social services both in and OOH, including: general practitioners (GPs), community nurses, community palliative care teams, hospitals, hospices, social workers, London Ambulance Service (LAS), 111, intermediate care and nursing/care homes. The service is clinician led with clinical governance embedded into its framework. Information added by any healthcare professional is immediately viewable by all the other legitimate professionals. The NHS 111 service is an urgent care response service that patients and carers can ring for help. It provides information and, if required, referral to a commissioned urgent care service identified from the London Directory of Services or CMC.9 The service is free and operates 24 h a day, every day. CMC is interoperable with 111. The 111 call handlers have direct links to CMC. If the patient is on CMC, the 111 system flags their details and the call is handed over to a nurse within the NHS 111 service who will be able to navigate the caller through the CMC record to help the patient access the right care in the right place at the right time.
CMC is a progressive technology that requires a clinical culture change in terms of delivery of the service. As such, CMC includes a highly defined clinical teaching and training package which encompasses identification, consenting, medical plan (current problems and anticipated problems), Advance Care Plan, resuscitation status, patient's specific wishes and guidance on how to input data onto CMC. This training is achieved through providing each user with a CMC training pack (produced by a multi-disciplinary team) alongside access to workshops delivered by experienced palliative care clinical nurse specialists (CNSs). The CMC implementation team consists of a clinical lead, a GP lead, an information governance lead (all clinicians), developmental manager, project manager, data manager and administration support alongside three whole time equivalent specialist CNSs.
The CMC integrated pathway
Identifying patients
CMC advocates identifying patients appropriate for CMC by using the SPICT.10 SPICT is a clinical tool developed to identify patients with one or more advanced, progressive illness and a limited prognosis (likely less than 1 year) who may have unmet supportive and palliative care needs.10 Training in the use of the SPICT tool is provided to community teams by the CMC trainers (specialist palliative care CNSs). GP practice and community nursing team meetings (eg, palliative care, supportive care, long-term conditions) can act as a prompt to highlight or review patients who meet the criteria of SPICT and are appropriate for inclusion or updating on CMC.
Consent
All patients are prospectively consented. If the patients lack capacity, they may be consented ‘in best interest’ when it is encouraged, wherever possible, that the patients’ relatives or next of kin are informed and involved. CMC provides a patient information sheet and advocates that the consenting process forms part of a wider necessary discussion about end-of-life care issues. This should always be patient-centric and embarked on at an appropriate time for the individual patient.
Completion of the CMC record
CMC is a contemporaneous record. Thus, it is not essential to complete all fields immediately. There are 11 mandatory fields on the CMC template that must be completed in order for a patient's details to be successfully added to CMC. These mandatory fields include patient demographic details (forename, surname, date of birth, GP and address), diagnosis, preferred place of care and death, resuscitation discussions and resuscitation status. If it is not an appropriate time to have a definitive answer to the mandatory fields entered, for example, preferred place of death (PPD), CMC has a drop down menu for this and the response ‘not yet discussed’ may be entered. In addition, the St Christopher's Advance Care Plan and the Do Not Attempt Resuscitation form taken from the Resuscitation Council, BMA and Royal College of Nursing joint statement 2007 have been integrated into CMC electronically.11 ,12
When a new patient record is uploaded onto CMC, the OOH teams (including GPs and 111), LAS and the patient's named GP all receive an automated, encrypted email alert and the patient details can be immediately viewed on CMC. The patient is also offered a paper copy of the CMC entry. In the full course of CMC development it is planned that patients will be able to access MY SPACE, that is, their own CMC record using a PIN number.
In line with recommended good practice, CMC supports GPs to review and update CMC when clinically guided. A minimum of 3 monthly review dates is recommended to ensure the information is still valid and up to date.
Reports
The automated reporting facility embedded in CMC provides potential for CMC to enhance current systems within the community and hospital settings for monitoring patients approaching the end of life, auditing clinical practice and can also aid case load management. Automated reports can be generated at the level of an individual nursing home, GP practice or district nursing area, for an individual specialist palliative care team or at a PCT/CCG level. Outcome reports include number of patients with a CMC record, number of deaths, details of PPD, along with actual place of death and reason for variance between actual and PPD.9
Results
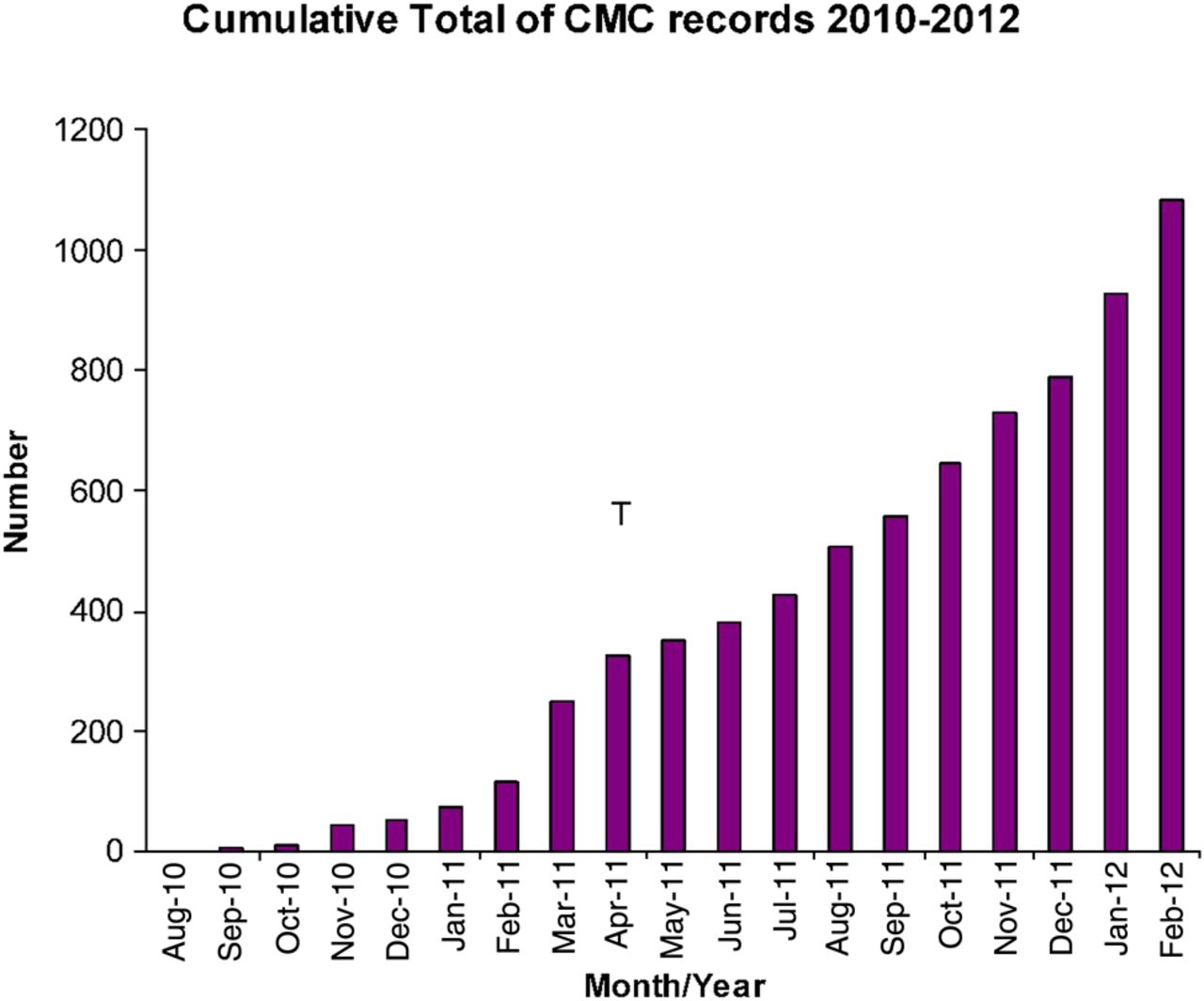
CMC records were created from August 2010 and censored on 1 March 2012 during implementation in two London PCTs (total population of approximately 600 000 people). Over this period, there were 1087 patients entered (figure 3). Of these 207 had died.

Cumulative total of patient records added to Coordinate My Care (CMC) over August 2010–March 2012.
The demographics of patients with a CMC record are shown in table 1. The mean age of patients was 80 years (SD 13), 59% were female and in four cases the gender was not complete. The primary diagnosis was non-cancer in 569 (52.3%), cancer in 503 (46.3%) and unknown in 15 (1.4%). In all, 15% of patients had dementia and 12% were frail elderly.
Details of cancer and non-cancer diagnosis of patients with a CMC record
Record entry
The consent field is mandatory and hence consent is completed for every CMC entry (table 2). Overall, 84% of CMC records were initiated in the community. The CMC team uploaded a proportion (19.7%) for professionals with no N3 link. The median length of time on CMC for all patients was 106 days (1–567) and for those patients who have died it was 38 days (1–455). Less than 5% of patients requested a copy of their CMC record.
Professionals initiating the CMC record and number of patients requesting a copy of their record
Outcomes
Preferred place of death
In all, 62% of the 1087 patients PPD was their usual place of residence, home 33% or nursing/care home 29%. Overall, 11% requested a hospice, 2% hospital and 3% other locations. For 21% of patients, this question had not yet been asked and in 1% the clinician deemed it inappropriate to ask.
Actual place of death
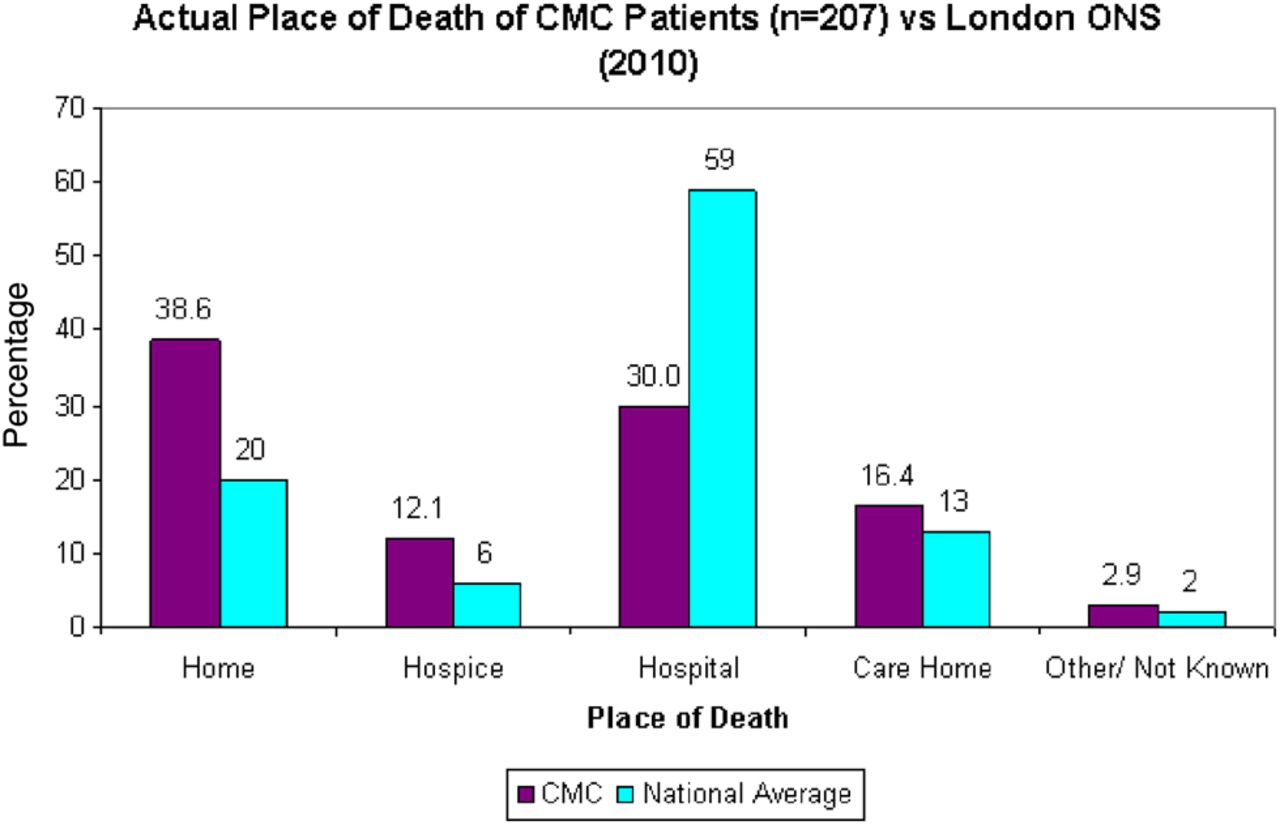
Actual place of death (n=207) was home 38.6%, care/nursing home 16.4%, hospice 12.1% and 30% in hospital. This equates to 55% of patients dying in their usual place of residence and reflects that 70% died outside of hospital (figure 4).
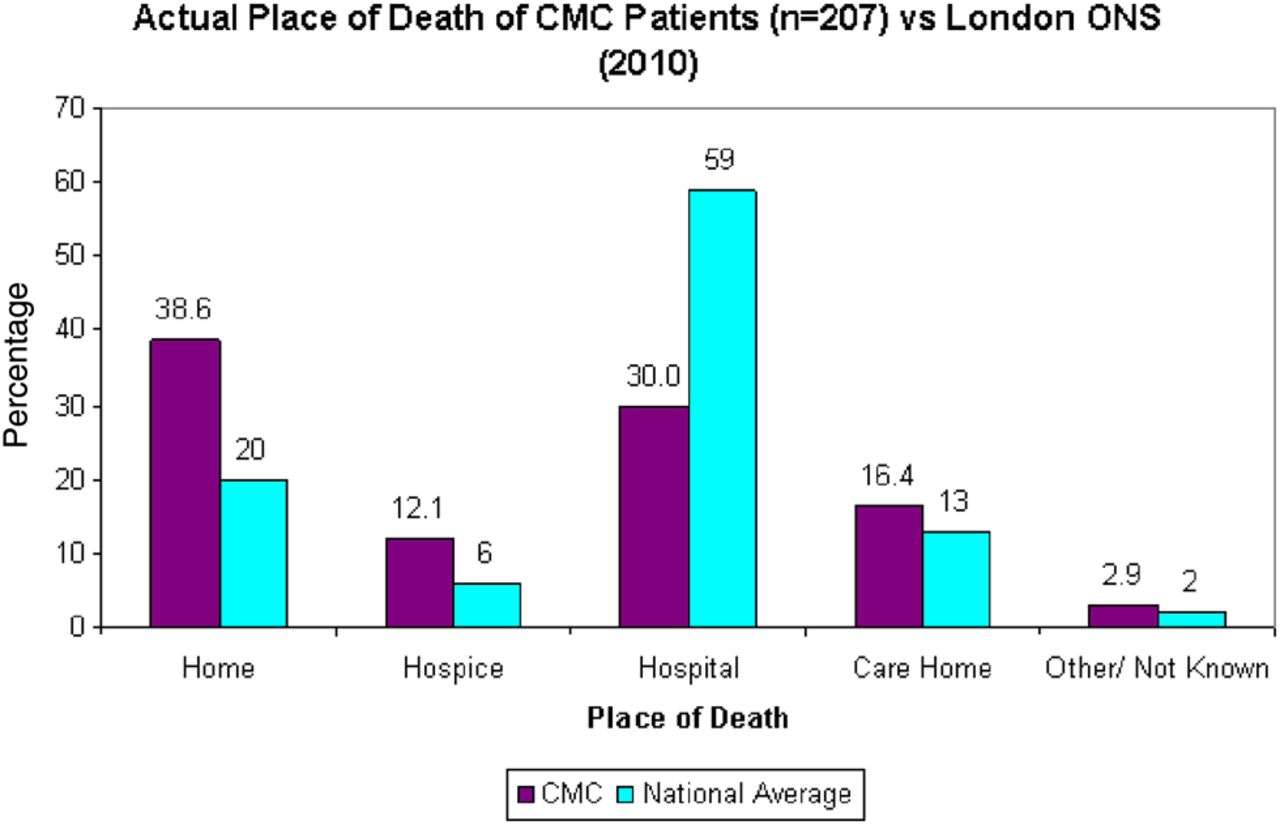
Actual place of death for Coordinate My Care (CMC) patients (n=207) versus The Office of National Statistics (ONS) National data 2010 (3,18).
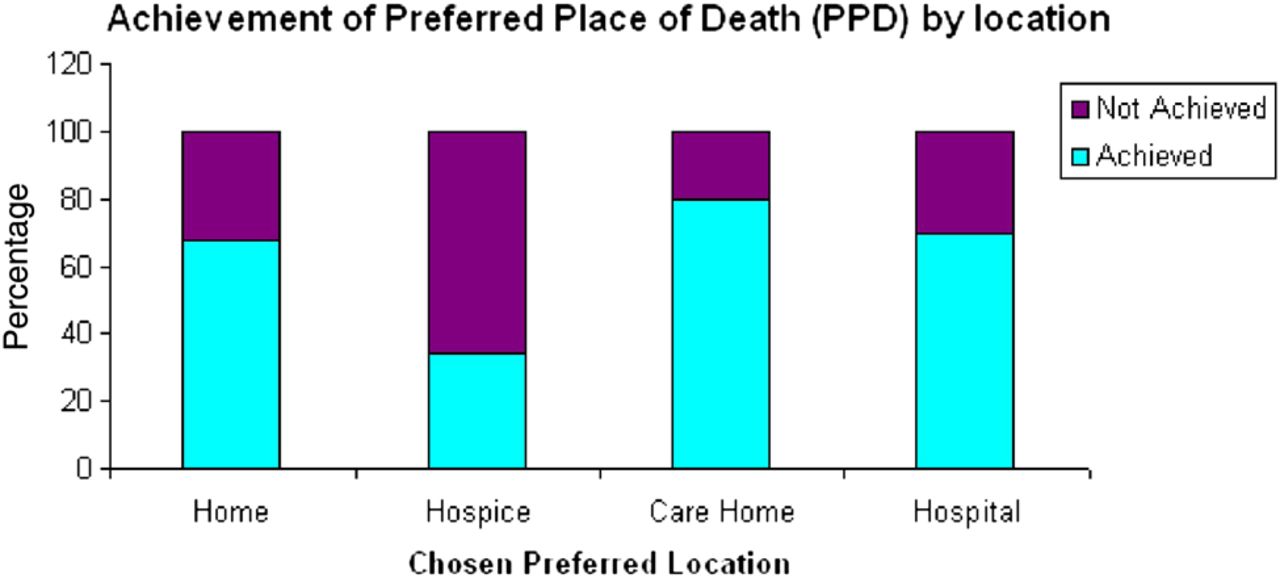
Figure 5 shows how the actual place of death equates to patient's PPD. If patients did express a preference this was achieved as follows for the main locations: home 56/82 (68%), hospice 11/32 (34%), care home 20/25 (80%) and hospital 7/10 (70%). In 26% of patients who died, PPD had not yet been discussed or was deemed to be inappropriate to discuss. Of those in whom preferences were not yet discussed at the time of death, 49% (26/53) died in hospital.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Achievement of preferred place of death by location of choice.
In Sutton and Merton, one of the early adopters of CMC, the After Death Audit (ADA) 200913 showed that 32% of patients on a GP paper end-of-life care register died in their PPD, compared with 62% who had their preferences documented electronically on CMC (2012).
Discussion
Key findings
Consent
In 2010, an audit of 154 faxed handover forms14 sent to the LAS showed that 112 (72.7%) forms had the consent questions answered. The answer to ‘Do you have the consent of the patient for the transfer of information?’ was ‘no’ in 36 (32%). Notwithstanding the lack of consent, details were shared with other providers. In CMC, consent is mandatory, and a patient's details cannot be shared unless consent is given or it is in the patient's best interest.
Healthcare professional engagement
In all, 86% of CMC records were initiated by community professionals, with generalists (GPs, district nurses and community matrons) responsible for 67%. This shows a high level of healthcare professional engagement for the concept of information sharing and integrated care. Previous research into the Scottish Emergency Palliative Care Summary (ePCS) supports this, showing patient, carers and HCPs all view the ePCS positively, none raising concerns about confidentiality.15
Interestingly, among the negative concerns regarding the ePCS was the reluctance to engage in new technology requiring additional computer skills. These negative concerns are repetitive themes in evaluations of IT across healthcare worldwide.16 ,17 However, 77% of CMC records were uploaded onto the IT system by the clinicians themselves showing that, in contrast to this previous work, it is clinician engagement in the IT system that underpins the CMC service. GPs interviewed regarding ePCS expressed difficulty in knowing when in a patient's illness trajectory it is appropriate to complete the ePCS.15 At the time of analysis, CMC held active records for 0.15% (880/600 000) of the PCT population. This is below the 1% of the population likely to be approaching the end of life and, alongside the relatively short time from record creation to death (38 days), highlights that one main barrier is the appropriate identification of end-of-life patients. Education and training around identification of end-of-life patients and communication about sensitive issues must go hand in hand with any electronic register implementation.
Social care professionals are now being trained to enter patients onto CMC. There is a specific template for social care involvement on the record.
Data quality
Overall, the data quality of information on CMC has improved compared with the audit of 2010 faxed handover information to London Ambulance.14 However, this report highlights areas for improvement pertaining to the design and set up of the IT used to store the CMC records. The main area of concern is blank/missing data. Diagnosis is unknown/blank for 1.4% of CMC records. Although the field in mandatory it is currently a free text box. This has resulted in some diagnoses being ambiguous. The new version of CMC has mandatory coded diagnoses on a drop down menu along with free text. This will resolve the problem. Also, the professional entering the data is unknown/blank in 3.7% of records. This is because this field currently relies on the users entering their details manually onto the record. In the new version of CMC, an ‘e signature’ will be automatically generated whenever a user logs onto the system. This will be viewable by all other users to allow professionals to be aware of exactly who added or edited patient details.
Advantages in Coordinate My Care
Patient and carer
-
Patient-centric care plan: right care, right place, right time
-
Wishes and preferences available to all care providers
-
Ability to access own copy of record
-
Ongoing process: no need to have to make decisions at any specific time
-
Able to access clinician at 111 directly
-
Brings end-of-life care services to patients who do not require specialist palliative care
-
Delivers greater equity to patients with non-malignant diseases
-
Delivers greater equity to patients cared for by generalists rather than palliative care specialists
Health and social care professionals
-
A range of care providers can update record
-
No need to repeat discussions–information each time they see a new health professional
-
Ensures that all health and social care providers receive the same information
-
Opportunity for specialists to train generalists
National Health Service
-
Provides real time data to support commissioning
-
Potentially saves costs in preventing unnecessary hospital admissions and interventions
-
Provides auditable outcome measures that support a governance infrastructure
Patient outcomes
CMC is a useful service for all patients with multiple diagnoses entering the pathway from many settings. Over half (52%) of the patients with a CMC record had a non-cancer diagnosis. Overall, 15% had dementia.
It is difficult to find previous baseline data to make direct comparisons with CMC data. The Office of National Statistics (ONS) publishes yearly figures for place of death. For London, these data were as follows for 2010: hospital 59%, home 20%, hospice 6% and care home 13%.18 This equates to 33% dying in their usual place of residence, and 55% of patients with a CMC record died in their usual place of residence. However, ONS data are for all deaths, including acute deaths and patients not identified as end of life. Therefore, a comparison with CMC has limitations. Nonetheless, when compared with the ONS London data for 2010, the overall CMC data do show an emerging change in trend with more care being delivered outside of hospitals (41% vs 70%).
The closest comparator data available for a single locality is from the ADA conducted in 2009 across the UK.13 This was a snapshot retrospective audit of GP records for all deaths over February and March 2009. Sutton and Merton PCT, one of the early adopters of CMC, participated in this audit prior to implementing CMC. Within Sutton and Merton, out of hospital deaths increased for patients on CMC compared with those on a GP paper register for the ADA data (79% vs 65%)13 and the proportion of patients dying in their place of usual residence has also increased for CMC (63%) compared with the ADA data (37%).13 Of those on a GP practice register, the ADA data13 show 56% had preferred place of care recorded compared with 80% of Sutton and Merton patients on CMC with a documented PPD. Preferred place of care and PPD were not documented separately in the ADA audit.
Documentation of a PPD is not always complete. End-of-life care discussions are sensitive, and CMC reflects that such discussions and decisions, including PPD, are an iterative process. For this reason, the CMC record is easily editable and also allows clinicians to share with others that these discussions have yet to be embarked upon. While it may not be appropriate to discuss PPD at the time of entering a patient on CMC, more training needs to take place to encourage professionals to have these discussions and update the PPD when appropriate.
Overall, CMC rates of achieving patient preferences for place of death are lower than recently published data19 for patients known to a community palliative care service. This is to be expected as only just over half of the patients (58%) on CMC are known to a specialist palliative care team, and the remainder are under the care of generalists in the community. This, along with the fact that 49% of patients who did not discuss their preferences died in hospital, highlights the need for ongoing training in communication skills and advance care planning for community professionals.
Only 34% of patients on CMC who chose hospice as their PPD achieved this preference. This is an area of concern, and may indicate a lack of availability of hospice beds for end-of-life care alone (as most hospice units are now specialist units in symptom control/complex needs) and a lack of access to admit to a hospice unit OOH or in an emergency setting. Rapid response community teams may be needed to care for these patients in their usual residence, and hospice as a choice may not always be a realistic option.
Although the numbers are small (no of deaths in care homes n=20), recent implementation of CMC in care homes has showed a positive trend. Where patients in care homes express a preference to die in the care home, it is achieved in 80% of cases. To build on this, a new CMC accredited training package is being developed to empower the staff to deliver end-of-life care in the homes.
Unanswered questions
There are some unanswered questions. First, this review only gives information about the patients for whom a CMC entry was completed. It is unable to tell us whether the introduction of the CMC has had an impact on the sharing of information with OOH teams for the patients on GP practice paper registers. There may be patients on GP registers who have not been entered onto CMC. Second, the Department of Health report on the eight locality end-of-life register pilots concluded that at the time of the report none of the pilots were at the point where they had evidence that locality registers improve quality of patient care.20 This is true of the CMC data presented here. At the present time, only an association can be made with having a CMC record and achievement of PPD, and although compared with previous available data, patients with a CMC record have an increased home death rate, place of death is only a surrogate marker for a good quality end-of-life care. Surrogate markers may not necessarily give an accurate representation of the quality of care. Data collection regarding other markers of quality at the end of life is ongoing and for future publications.
The London Ambulance Service
The LAS is the only pan-London Trust. It covers 31 PCTs. CMC offers a standardised record that alerts the ambulance crew to the patient's wishes, resuscitation status, care plan and which professional to contact for ongoing care. This empowers the crews to deliver care according to the plan and avoids them taking the patients to Accident and Emergency.
Implementation and next steps
A pan-London CMC roll out will take place over the next 12 months. All areas in London will have a CMC service by April 2013. This roll out will be synchronised with the 111, unscheduled care telephone number. The implementation of CMC is endorsed by NHS London.
Conclusions
CMC is a ‘disruptive technology’ and shows potential to transform the way we do things and, at the same time, making the process more efficient and less expensive. CMC has been shown to change culture and deliver fully integrated, personalised end-of-life care. It can streamline the provision of health and social services that require complex interventions from multiple professionals across multiple settings (box 1). CMC service represents a change of culture. Changing a culture requires facilitation and training. The CMC service has a well-defined pathway that is underpinned by an electronic solution. The vision is that CMC will be to end-of-life care what the ATM has been to banking.
Acknowledgments
We would like to acknowledge the Coordinate My Care clinical team and in particular Ian Haig, Kate Mansell, Jayne Wood, Anna-Marie Stevens, Berit Moback, Meena Valambhia and Tom Bridgeman for their assistance. We also like to acknowledge Debra Swann, St Christopher's Hospice, the Resuscitation Council and the University of Edinburgh for use of the SPICT.
Footnotes
-
Contributors Planning and conduct of CMC design and data collection: JR, LH, CCC and CM-S. Planning of original article design and content: JR, CS, JR and MT and ES. Data collection and analysis: JRR, CS and JR. Article amendments and revisions: JR, MT and CS. Contributor responsible for overall content as guarantors: CS and JR
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Additional unpublished data are available from Dr Clare Smith, Palliative Care Research Fellow; clare.smith@rmh.nhs.uk