Article Text

Abstract
Background Cancer-related pain is a significant and debilitating problem. Non-pharmacological treatments such as acupuncture may have an adjunctive role in controlling pain without the undesirable side effects of drug regimens and yet the evidence base remains limited.
Objectives The main objective of this systematic review was to evaluate the effectiveness of acupuncture in the management of cancer-related pain in adults. Subgroup analyses were planned for acupuncture dose and for the outcome of studies investigating acupuncture for cancer-induced bone pain.
Methods Six electronic databases were searched, including the Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, PsycINFO, AMED and SPORTDiscus. Studies included in the review were randomised controlled trials investigating the use of acupuncture for cancer pain using pain as a primary outcome measure. In total, 253 published references were identified but only three studies met the inclusion criteria and were included in the final review.
Results Of the three included studies, only one was judged to be of high methodological quality and showed auricular acupuncture to be superior to placebo acupuncture and ear seeds at placebo points. However, the study was relatively small and blinding was compromised. The two low-quality studies gave positive results in favour of acupuncture for cancer pain, but these results should be viewed with caution due to methodological limitations, small sample sizes, poor reporting and inadequate analysis.
Conclusion There is insufficient evidence to judge whether acupuncture is effective in treating cancer pain in adults.
Statistics from Altmetric.com
Introduction
Cancer-related pain is a significant and debilitating problem. Moderate-to-severe pain affects around 40% of individuals with early or intermediate stage cancer and 90% of individuals with advanced cancer.1 2 Pain in cancer is complex and may be due to pre-existing pathologies, tumour growth, bone metastases or the treatment of cancer itself.3 Bone pain due to metastatic cancer is often severe, unremitting and poorly controlled.4 Cancer pain management is largely pharmacological,1 5 and yet up to 70% of patients with cancer-related pain do not receive adequate pain relief, thus affecting quality of life.6,–,9 Non-pharmacological treatments such as acupuncture may have an adjunctive role in controlling pain without the undesirable side effects of drug regimens and yet the evidence base remains limited.
Although acupuncture may have a role in the management of cancer pain, an earlier systematic review of acupuncture for cancer pain was inconclusive10 and a more recent systematic review of systematic reviews did not find evidence that acupuncture alleviated cancer pain although it was effective for nausea.11 There is an ongoing debate about the effectiveness of acupuncture for other types of pain. Some systematic reviews have suggested that acupuncture may be superior to placebo or sham12,–,16 while others have found limited efficacy and inconclusive evidence.17,–,20 Dosage in acupuncture might also be important and some researchers suggest that the minimum required for a beneficial effect is six treatments using at least four points at a frequency of at least once a week, although the efficacy of these recommendations has not been investigated fully.13 21 Some research also suggests that needle sensation, ‘de qi’, resulting from manual acupuncture might also be necessary for optimum benefit.13 22 23
The aim of our systematic review, conducted using a Cochrane protocol,24 was to evaluate the effectiveness of acupuncture in the management of cancer-related pain in adults. Subgroup analyses were planned for acupuncture dose and for the outcome of studies investigating acupuncture for cancer-induced bone pain.
Methods
Data sources and study selection
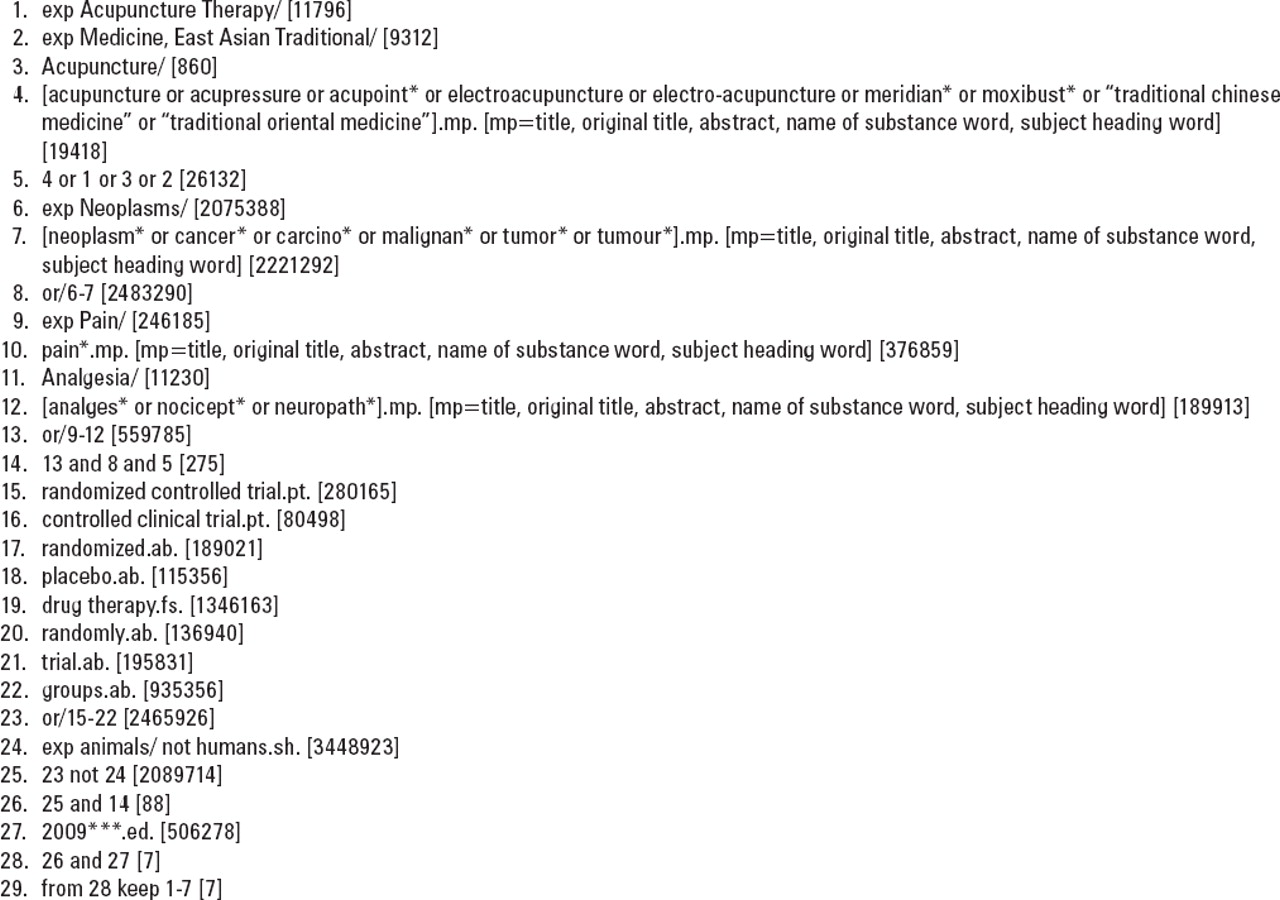
Six electronic databases were searched, including the Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, PsycINFO, AMED and SPORTDiscus. The MEDLINE search strategy is summarised in figure 1. This was combined with the Cochrane Sensitive Search Strategy for randomised controlled trials (RCTs).25 Search strategies based on the MEDLINE strategy were devised for the remaining databases. Foreign language papers were translated if they were identified for possible inclusion in the review via their abstracts.

MEDLINE search strategy for randomised controlled trails of acupuncture for cancer pain.
Studies included in the review were RCTs investigating the use of acupuncture for cancer pain and had to contain clinical data. Studies that evaluated any type of invasive acupuncture for cancer-related pain in adults were included, for example, manual acupuncture, electro-acupuncture, auricular (ear) acupuncture and either Western style or traditional Chinese acupuncture. Those comparing non-invasive techniques such as laser acupuncture or acupressure were excluded. Comparators included no treatment, treatment as usual, non-penetrative sham (non-invasive treatment), penetrative sham (invasive treatment at non-acupuncture points) or other active interventions, including oral medication. Case reports, abstracts and letters were excluded.
The primary outcome measure was patient-reported pain intensity using validated scales such as visual analogue or numerical rating scales. Secondary outcome measures included pain relief as measured by validated pain scales (eg, Visual Analogue Scale (VAS)), patient satisfaction, quality of life, analgesic consumption and changes in concurrent treatments, hospital attendance/admission (including Hospice admission) or adverse events (major or minor).
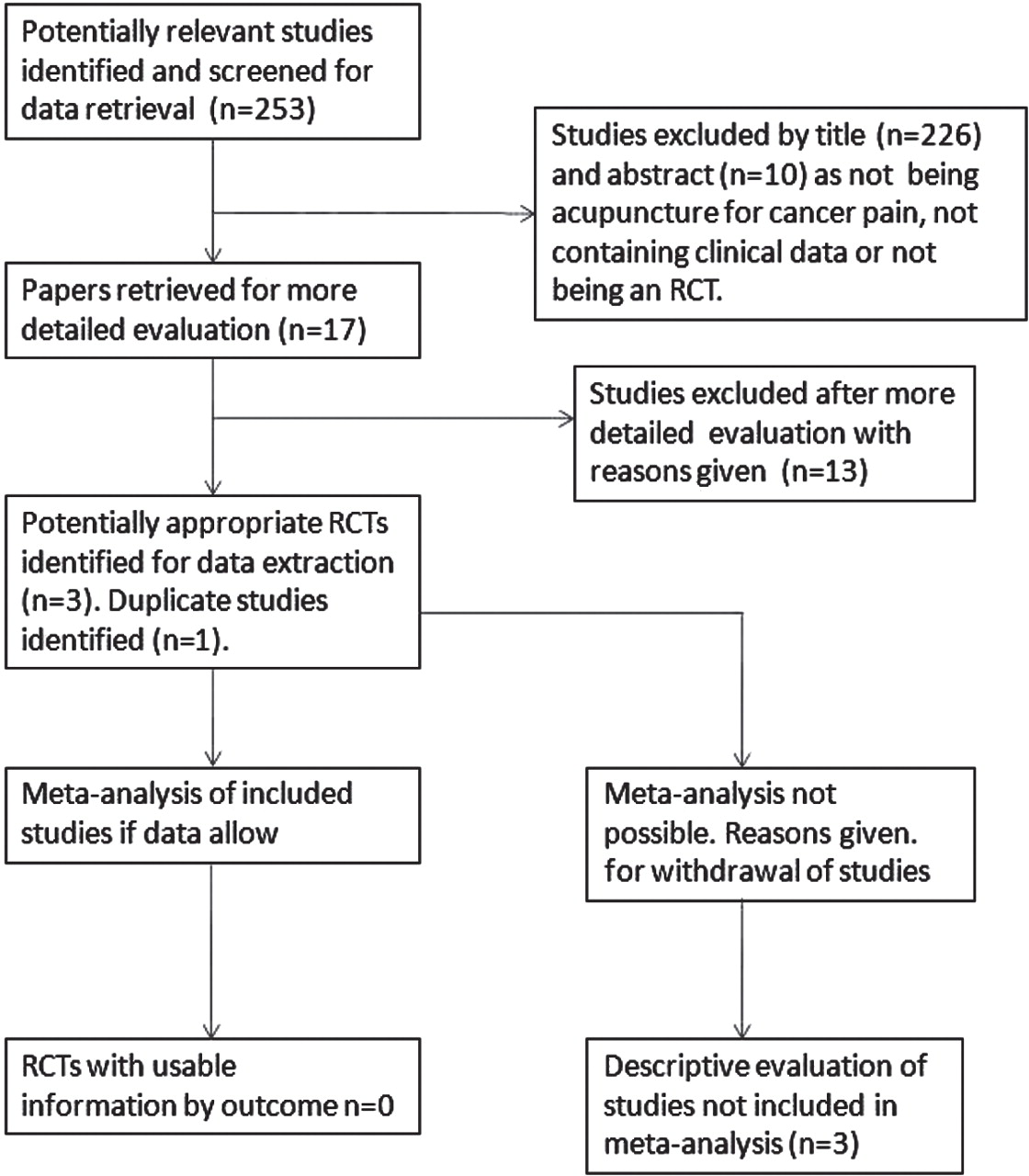
In total, 253 published references were identified and it was possible to exclude 236 after initial screening by title and abstract as not meeting our eligibility criteria. Full study reports were obtained for the remaining 17 studies and a further 13 were subsequently excluded. Two of the four remaining papers reported the same study and therefore three papers were included in the final review.
Data extraction
Two reviewers independently scrutinised each paper and completed a detailed data extraction log that included information on participants, intervention characteristics, comparator, analgesia, adverse effects, outcome measures and withdrawals. Decisions were also made on methodological quality using a modified Jadad score.26 27 Final scores were discussed and agreed between the two reviewers with a third acting as arbiter.
Results
The review process is shown in figure 2. Only 3 of the 17 studies selected from the original 253 identified met the eligibility criteria for the review.28,–,30 One study31 was used as a secondary reference to one of the included papers as it was an earlier report of the same study.30

{kind=link}
{kind=link}
Review flow chart.24 RCT, randomised controlled trial.
Descriptive analysis of studies
A summary of the three included studies is presented in table 1.
Summary of included studies
Alimi et al28 recruited 90 participants with chronic peripheral or central neuropathic pain related to cancer and assigned them to three groups: auricular acupuncture using semipermanent needles (n=30), auricular acupuncture using semipermanent needles administered at non-acupuncture (placebo) points (n=30) and non-invasive auricular ‘seeds’ administered at non-acupuncture (placebo) points (n=30). Mean pain intensity on VAS was similar in each group at baseline (57–58 mm). Each group received two courses of treatment with needles or seeds left in situ and were asked not to modify their analgesic medication during the course of the study. The duration of each course was determined by the time it took for the needles to fall out or for the ear seeds to become unstuck and fall off. Pain scores were recorded at 1 month (termed D30 in the report) and 2 months (termed D60 in the report). Measures of electrodermal response at points on the ear were also taken at the same intervals. No adverse events were reported by either participants or their doctors. The main outcome measure was pain at 2 months, with secondary outcomes being pain at 1 month and electrodermal response at 1 and 2 months.
The reported results showed a decrease in pain intensity of 36% (58–37 mm on VAS) from baseline at 2 months in the acupuncture group with only a small change in the group having acupuncture at placebo points (58–55 mm on VAS). The difference between the acupuncture and placebo acupuncture groups was statistically significant (p<0.0001). Pain scores at 1 month were also lower in the true acupuncture group than either of the other two groups.
Chen et al29 conducted a parallel group study comparing acupuncture to analgesic medication. This paper was written in Chinese and was translated independently by two colleagues, one from the Languages Department within our university and one from The Hong Kong Polytechnic University. Sixty-six adult participants (age range of 41–70 years) with pain associated with ‘late’ but unspecified types of cancer were categorised into groups according to pain severity—‘mild’, ‘moderate’ and ‘severe’. Participants received either acupuncture applied at three to five ‘tender’ acupuncture points or analgesic medication based on the WHO three-step principle that included aspirin for mild pain, codeine for moderate pain and morphine for severe pain. No placebo control group was included. Pain intensity was measured by change in Visual Analogue Score. Participants were categorised into groups according to the change in pain intensity relative to baseline as follows:
▶ Complete relief = Visual Analogue Score changes of 91–100% reduction in pain intensity from baseline.
▶ Average relief = Visual Analogue Score changes of 61–90% reduction in pain intensity from baseline.
▶ Partial relief = Visual Analogue Score changes of 31–60% reduction in pain intensity from baseline.
▶ No relief = Visual Analogue Score changes of less than 31% reduction in pain intensity from baseline.
The percentage of participants falling into each of the above categories was calculated and recorded and a cut-off point of pain relief of 31% or more was set as the criterion for ‘general effectiveness’. It was concluded that the analgesic effect of acupuncture was markedly more effective than medication with the total effectiveness of acupuncture reported as 94% in the acupuncture group and 87.5% in the medication group (p<0.05). It was not possible to extract data because neither raw data nor SDs were reported.
Dang and Yang30 randomly allocated 48 participants with pain from stomach carcinoma to receive acupuncture (filiform needle), acupuncture point injection with human transfer factor or Western medicine (analgesic medication based on the WHO analgesic ladder). An additional group of 16 healthy normal participants were used as a control and received no intervention. Acupuncture was administered at four to five ‘main points’ and two to four ‘auxiliary points’ according to traditional acupuncture points and based on the patient's signs and symptoms. Needles remained in situ for 20 min. Treatment was given ‘continuously’ (treatment duration not specified) for 2 weeks followed by a gap of 2–3 days before continuing. The total treatment period was 2 months. Each acupuncture treatment course consisted of one treatment per day for grade I pain and two to three sessions per day for grade II or III pain (according to the WHO criteria). For the point injection group, an injection of 0.5 ml of freeze-dried human transfer factor aqueous solution was administered into four acupuncture points selected in a similar manner to the acupuncture group. This was done twice per week. Participants in the Western medicine group received analgesics including aspirin, indomethacin, AP-237, codeine, dihydrocodeine and dolantin, based on the WHO three-step ladder. Transient effects (30 min after treatment) and long-term effects (12 h post-treatment) were calculated for the first 10 days of treatment and the final 10 days of treatment over a 2-month period. At each stage of the study, participants were categorised into groups according to the effectiveness of treatment: ‘markedly effective’, ‘improved’ and ‘ineffective’. The percentage of participants in the ‘markedly effective’ and ‘improved’ category groups were used as a measure of effectiveness. No explanation was given as to how pain was measured and how participants were categorised into these groups.
The results indicated that medication provided more effective analgesia during the first 10 days of treatment when considering both transient and long-term effects. During the final 10 days of treatment, the transient effects of the acupuncture and point injection group were similar to the medication group and the long-term effects were equal (p> 0.05). However, taking only the long-term ‘markedly effective’ scores for the acupuncture (48.8%) and point injection (51.9%) groups during the final 10 days of treatment, these were significantly higher than that in the medication group (33.8%) (both p<0.05).
The three studies included in the review were heterogeneous in terms of pain states, patient populations and acupuncture protocols, and this prevented meta-analysis. Only one of the three studies28 was judged to be of high methodological quality on the Modified Oxford 5-Point Quality Scale (table 2).
Modified Oxford 5-Point Quality Scale for assessment of methodological quality of the three included studies
Discussion
The results of this systematic review are inconclusive. Only three studies met the eligibility criteria, and heterogeneity prevented meta-analysis. Only one of the three studies included was deemed to be of high methodological quality on the Modified Oxford Scale,28 but this study was relatively small and there were methodological problems in that the ear seeds group were effectively unblinded because the seeds were applied with tape and some eventually fell off during the course of the study. The two acupuncture groups were initially blinded but again, if and when the needles fell out, participants were unblinded. The remaining two studies29 30 reported positive results, but the inadequacy of outcome measures, the absence of a reliable statistical methodology and a failure to report blinding undermines this evidence. Both of these studies were inadequately reported.
Only one systematic review on acupuncture for cancer pain has been previously published.10 This identified seven studies as meeting the eligibility criteria, but the one study judged as being of high methodological quality was the study conducted by Alimi et al,28 which was also identified during the present review. The authors concluded that there was insufficient good quality evidence to determine the effectiveness of acupuncture for cancer-related pain.
None of the studies considered during the present review considered optimal acupuncture dose or considered needle sensation (de qi).32 It has recently been suggested that low implementation fidelity (bias leading to an underestimation of treatment effects) might be present in studies using suboptimal doses of Transcutaneous Electrical Nerve Stimulation (TENS) and the same might be true of other non-pharmacological interventions such as acupuncture. Future studies should ensure adequate dosage and use appropriate outcome measures to avoid this problem.33 The design of future studies should also be adequately powered via the use of sample-size calculations, and investigators should consider the use of homogenous cancer populations. It has also been noted that none of the included studies considered cancer-induced bone pain specifically, although the physiological evidence is promising.34 As bone metastases are the main cause of cancer pain and difficult to adequately control,35 this represents an important area for further study.
Conclusion
The evidence from one high-quality RCT is insufficient to provide a judgement on whether acupuncture is effective in treating cancer-related pain. Acupuncture is widely used to treat this type of pain,36,–,40 but the available evidence is inconclusive or of low quality. Therefore, a judgement on whether acupuncture is effective for cancer-related pain cannot yet be made and more large, well-designed RCTs are required.
Acknowledgments
The authors would like to express their gratitude to Prof. Yi Young from Leeds Metropolitan University and Dr Alice Jones from The Hong Kong Polytechnic University for assisting with the translation of the Chinese paper.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.