Article Text

Abstract
Objective To assess the clinical utility of the Gold Standards Framework Prognostic Indicator Guide (GSF) and the Seattle Heart Failure Model (SHF) to identify patients with chronic heart failure (CHF) in the last year of life.
Design, setting and patients An observational cohort study of 138 community based ambulatory patients with New York Heart Association (NYHA) class III and IV CHF managed by a specialist heart failure nursing team.
Main outcome measures 12 month mortality, and sensitivity and specificity of GSF and SHF.
Results 138 CHF patients with NYHA class III and IV symptoms were identified from a population of 368 ambulatory CHF patients. 119 (86%) met GSF criteria for end of life care. The SHF model identified six (4.3%) patients with a predicted life expectancy of 1 year or less. At the 12 month follow-up, 43 (31%) patients had died. The sensitivity and specificity for GSF and SHF in predicting death were 83% and 22%, and 12% and 99%, respectively. Receiver operator characteristic analysis of SHF revealed a C index of 0.68±0.05 (95% CI 0.58 to 0.77). Chronic kidney disease (serum creatinine ≥140 μmol/l) was a strong univariate predictor of 12 month mortality, with a sensitivity of 56% and specificity of 72%.
Conclusions Neither the GSF nor the SHF accurately predicted which patients were in the last year of life. The poor prognostic ability of these models highlights one of the barriers to providing timely palliative care in CHF.
Statistics from Altmetric.com
Introduction
The epidemiology of heart failure is changing1 as we confront improved survival following myocardial infarction2 and advancing life expectancy.3 The highest incidence and prevalence is in people over 80 years of age.4 5 Complications arising from heart failure account for 4% of deaths in the UK each year, and following a new diagnosis of chronic heart failure (CHF), 40% of patients will survive less than 1 year.5 However, for the remaining 60%, progression of the illness can be variable, although is typically progressive with repeated episodes of decompensation, often requiring hospitalisation. Increased use of life prolonging medications and implantable devices over the past 10 years has increased the average life expectancy of CHF patients.6 Despite this, survival remains worse than many cancers (figure 1).7 However, unlike cancer patients, few CHF patients receive additional supportive or palliative care during the end stage of their disease.
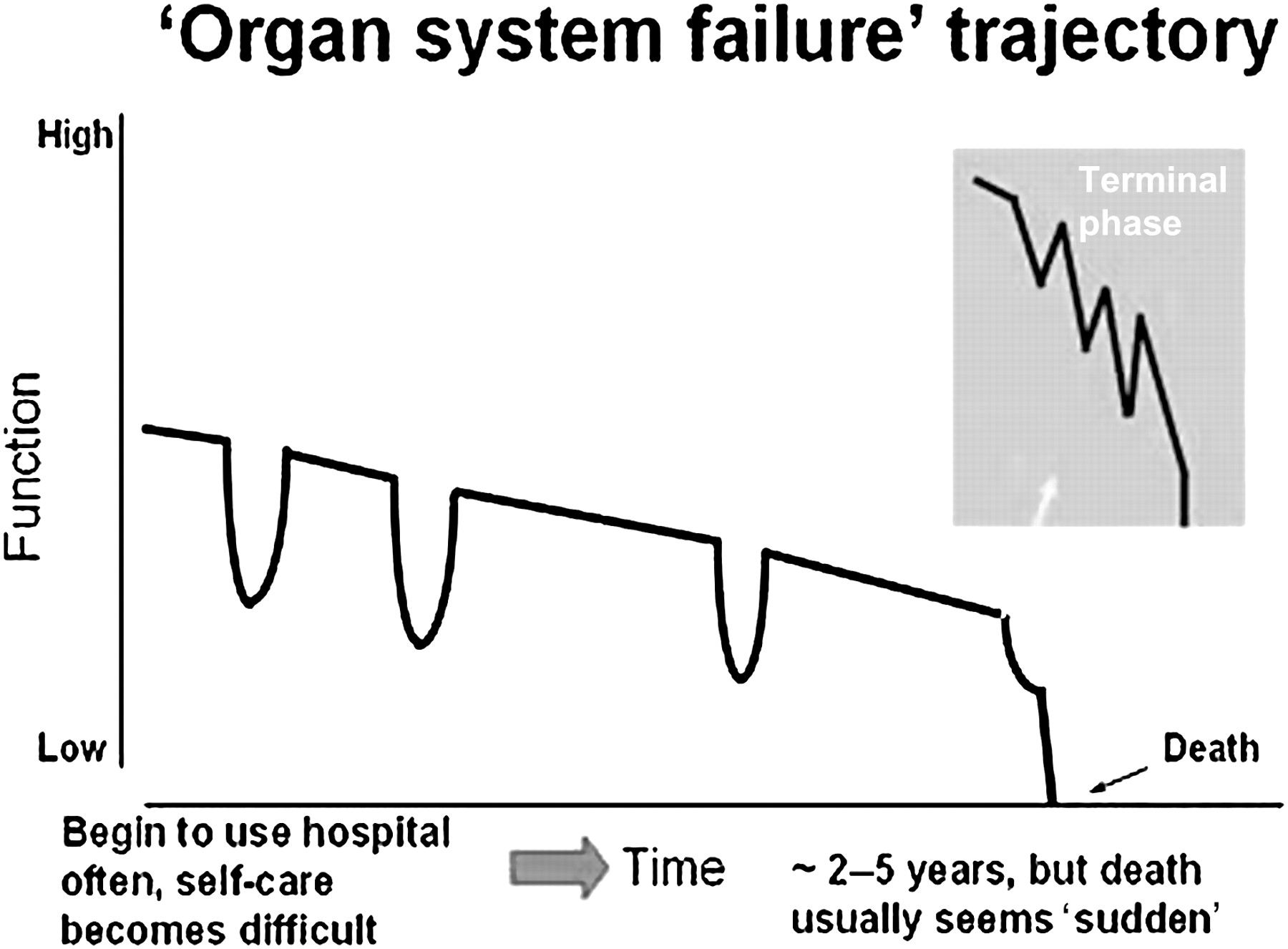
Organ failure trajectory (reprinted with permission from Murray et al6).
In recognition of the current gap in end of life care, both UK and European initiatives have advocated the use of palliative care in CHF patients.8 9 The European Society of Cardiology set up a palliative care workshop to address the issues of palliative care in CHF and to increase awareness.10 In the recently published ‘Clinical standards: for heart disease’,11 it is recommended that “patients that remain symptomatic despite optimal treatment should have access to supportive and palliative care according to their needs”. These standards also recommend the use of the Gold Standards Framework-Prognostic Indicator Guide (GSF)12 to help identify heart disease patients that are reaching end of life. The GSF published in 2006 in England recommended a series of simple criteria to help identify patients nearing end of life. For CHF, these guidelines set out four criteria, two of which the patient must meet in order to be considered for palliative care (see appendix 1). Although these criteria are being recommended for use in CHF patients, to date, there is no published evidence on their predictive accuracy in identifying patients in the last year of life.
In contrast, the Seattle Heart Failure Model (SHF) (available online http://depts.washington.edu/shfm/app.php)13 uses clinical data to statistically predict likelihood of survival in CHF patients. The model has been validated in over 10 000 patients with reasonable predictive value, and is now considered a ‘gold standard’ for clinical prognostication in ambulatory CHF patients. However, there have been criticisms of the SHF due to the fact that it was developed solely on data from patients taking part in randomised clinical trials. However, smaller subsequent studies have indicated it may be useful in community based heart failure patients when additional factors such as brain natriuretic peptide or renal function are added into the model.14
The primary aim of this study, therefore, was to evaluate the GSF criteria for heart failure as a simple qualitative method of identifying patients in the last year of life and compare this to an established quantitative model based on detailed clinical and biochemical data, the SHF.
Methods
Patient selection
Community based, ambulatory patients with CHF were identified from a clinical database used by the specialist heart failure nursing team in the local health authority. Patients were included if they had New York Heart Association (NYHA) class III or IV symptoms and were currently managed by the specialist heart failure nurse. Patients were excluded if they were due to be discharged from the heart failure nursing service within the following 6 weeks.
Gold Standards Framework criteria for heart failure
Each of four specialist heart failure nurses was interviewed, independently, with regard to the patients under their care. Nurses were asked to provide an answer to the GSF ‘surprise question’—that is, “Would you be surprised if this patient died in the next 6–12 months?”; and to indicate whether or not the patient continued to have difficult physical or psychological problems, despite optimised treatment. The additional two criteria, NYHA class III or IV symptoms and two or more heart failure related hospital admissions within the last 12 months, were obtained from the clinical heart failure database (appendix 1).
The Seattle Heart Failure Model
Data required for the SHF were obtained from a local clinical heart failure database and a central patient electronic record system, including date of diagnosis; aetiology of heart failure; number of all-cause and CHF related hospital admissions during the 12 months before and after enrolment; total number of days spent in hospital during the 12 months before and after enrolment; and degree of left ventricular dysfunction. The most recent values for systolic blood pressure (mm Hg), weight (kg), haemoglobin concentration, total white blood cell count, lymphocyte count (percentage of total white cell count), urea and electrolytes, plasma cholesterol (mmol/l), plasma uric acid (if available), serum creatinine (sCr, μmol/l) and current medications were recorded. QRS duration on the most recent electrocardiogram, other medical diagnoses and comorbidities were also documented. These variables were imputed for each individual patient using the online SHF (http://depts.washington.edu/shfm/) to generate a value for 1 year predicted survival and mean life expectancy at baseline (appendix 2).
Data handling and statistical analysis
Data were analysed using SPSS (V.17) software. Data with continuous variables and a normal distribution were analysed using an independent samples t test. For nominal or categorical data, a χ2 analysis with a Pearson's test for significance was used. Sensitivity and specificity analysis was performed on nominal data in comparison with death at 1 year. The predicted survival data yielded from the SHF were also analysed using a receiver operator characteristic, area under the curve analysis using SPSS. All data for the study were acquired in accordance with the Data Protection Act (1998) and stored anonymously within secure National Health Service computer systems. The study was granted ‘audit’ status by a member of the South East Scotland Research Ethics Committee and was therefore not considered to require full ethical review.
Results
Patient characteristics
One hundred and thirty-eight patients were identified as meeting the inclusion criteria from a total of 368 being actively managed by the specialist heart failure nurse service. Baseline characteristics (table 1) demonstrated a typical elderly Caucasian heart failure population with a mean age of 77 years, predominantly male, ischaemic heart disease as the dominant aetiology and most patients having moderate or severe left ventricular systolic dysfunction. Three-quarters of patients were taking angiotensin converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARB) and nearly 60% were currently prescribed β blockers. Patients who were not taking these drugs had documented contraindications, including hypotension, bradycardia and renal impairment, or had been symptomatically intolerant of these drugs. Forty-five per cent of patients (62/138) were in persistent or permanent atrial fibrillation.
Baseline demographics and clinical characteristics
Gold Standards Framework criteria
For 120 (87%) patients, the specialist heart failure nurses reported ‘no’ to the surprise question, indicating that they would not be surprised if the patient died within the next 6–12 months. In addition, 32 (24%) patients had repeated (≥2) hospital admissions for symptoms of heart failure in the previous 12 months; and 113 (82%) were judged to have difficult clinical symptoms despite optimised therapy. Overall, 119 (86%) patients therefore met GSF criteria for palliative care (meeting two or more of the four criteria). At the time of baseline assessment, patients that met GSF criteria had spent significantly longer in the heart failure service (p=0.031); had significantly more all-cause hospital admissions over the previous 12 months (p=0.001); and had spent significantly more days in hospital over the same time period (p<0.001).
The Seattle Heart Failure Model
Based on the SHF, only 6/138 patients were predicted to have a life expectancy of 12 months or less. The majority of patients (113/138) had a predicted life expectancy of >2 years, and 57/138 were predicted to live at least 5 years. Figure 2 illustrates the discrepancy in the predicted 1 year mortality between the GSF and SHF. However, patients meeting GSF criteria did have a significantly lower likelihood of surviving 1 year based on the SHF prediction (76±16% vs 82±11%; p=0.038).

{kind=link}
{kind=link}
Comparison of the Gold Standards Framework Prognostic Indicator Guide (GSF) and the Seattle Heart Failure Model (SHF) in predicting life expectancy of less than or greater than 12 months.
Overall mortality at 12 months
All patients were followed-up for 12 months from the initial nurse interview for death, cause of death and place of death. For patients who died in hospital, this information was obtained from a central electronic patient record system. For those who died out of hospital, the patient's GP was contacted, by letter, and asked to provide the information. At 12 months, 43 (31%) patients from the initial cohort of 138 had died.
Place and cause of death
The place and cause of death were identified in 37 of 43 deaths (86%). The remaining six patients died in the community and we were unable to trace the cause of death although it was likely to be sudden in nature. With regard to place of death, 23 (53%) died in hospital, 11 (26%) died in the community and nine (21%) died either in hospice care or in a respite nursing home. With regard to cause of death, 28 (76%) died due to progressive heart failure, nine (21%) died with a sudden death syndrome and three (8%) died from cancer. One patient died of renal failure which was not thought to be directly attributable to heart failure, one from severe sepsis and one from head injury. Those who died were older, had more severe symptoms and had a shorter life expectancy, as predicted by the SHF (table 2).
Characteristics of patients dead versus alive at 12 months
Sensitivity and specificity of GSF and SHF in predicting 12 month mortality
The GSF and SHF were evaluated for sensitivity and specificity for identifying patients who would not survive 12 months. For the GSF, meeting two or more of the four criteria yielded a sensitivity of 83% and a specificity of 22%, with a positive predictive value (PPV) of 33% and negative predictive value (NPV) of 5%. This provided an overall accuracy of 41%. For the SHF, having a mean life expectancy of <1 year yielded a sensitivity of 12% and a specificity of 99%. The PPV was 83% and NPV 71%, providing an overall accuracy of 72%. A receiver operator, area under the curve analysis performed on the SHF data yielded a C index of 0.68±0.05 (95% CI 0.58 to 0.78) (table 3).
Sensitivity and specificity analysis of the Gold Standards Framework Prognostic Indicator Guide, the Seattle Heart Failure Model and renal function
Hospital admissions
During the 12 month follow-up period, 22% of the cohort had one heart failure related hospital admission, 10% had two and 4% had two or more. There was no significant difference in the number of admissions during the follow-up period for patients who met GSF criteria compared with those that did not (p=0.836). Patients who had repeated heart failure admissions (≥2) prior to the baseline assessment had significantly more readmissions during the 12 month follow-up (0.94±1.2 vs 0.46±0.8, (n) p=0.008).
Renal function and mortality
Serum creatinine (sCr), as a single factor, demonstrated the highest sensitivity and specificity for predicting death at 12 months. A cross tab analysis dividing patients into those with a sCR less than or greater than 140 μmol/l had a sensitivity of 56% and a specificity of 72% (p<0.001) with a PPV of 56% and a NPV of 79%, and an overall accuracy of 72% for predicting death at 12 months. Receiver operator curve analysis using sCR with a cut-off of >140 μmol/l yielded a C index of 0.76±0.05 (95% CI 0.61 to 0.80). A comparison of the mean sCr for patients alive and dead at 1 year showed a significant difference, with those patients alive at 1 year having lower sCr (123.3±44.8 μmol/l vs 186.3±106.5 μmol/l; p<0.001). Patients with chronic kidney disease in stage 4 or 5 were significantly more likely to be dead at 1 year (p<0.001).
Medications and mortality
Patients prescribed either ACE inhibitors or ARB medications were significantly more likely to be alive at 12 months than patients who were not taking either drug (p=0.019). This association was not observed for either β blockers or aldosterone antagonists although the numbers were small for these groups (p=0.510 and p=0.142, respectively). Patients receiving ACE inhibitors or ARB also had a significantly higher mean estimated glomerular filtration rate than patients on neither medication (on ACE inhibitors/ARB 44.5±13.6 vs 38.5±16.1 ml/min/1.73m2; p=0.033) reflecting a lower use of angiotensin inhibition/antagonism in patients with lower estimated glomerular filtration rate.
Discussion
This study sought to evaluate a pragmatic clinical approach to identifying CHF patients that might benefit from supportive and palliative care, using two different prognostic tools. The tools chosen represent two contrasting approaches and are reflective of the differing views and beliefs held by cardiologists and palliative care physicians. One tool, the SHF, utilises a complex data algorithm derived from large clinical trial databases, and the other, the GSF, is based on a consensus panel of physicians attempting to identify complex needs using simple criteria readily accessible in the clinical setting. Our study clearly shows that neither approach is accurate in predicting which CHF patients will survive 12 months. The findings highlight the difficulties in predicting end of life in CHF patients and the limited utility of currently available tools.
Gold Standards Framework criteria
The GSF was developed by a consortium group to address the increasing need for palliative care in non-cancer patients. Their aim was to develop a set of ‘triggers’ to identify patients nearing the end of life using simple questions (eg, the ‘surprise question’) and specific indicators of end stage organ failure. However, in this patient sample, the GSF greatly overestimated the number of patients nearing end of life. The lack of specificity of this tool is highlighted by the ‘surprise question’ which was positive in 87% of our cohort. The heart failure nurses commented that their answer to this question was strongly influenced by the fact that these patients were typically elderly and frail and so the risk of sudden death was high and, in their experience, not uncommon.
The Seattle Heart Failure Model as a practical prognostic tool
In contrast with the GSF, the SHF under estimated 12 month mortality. Possible reasons for this include the question of applicability of the SHF to this unselected CHF population. The SHF was developed and validated on data from CHF patients entered into clinical trials, and thus these patients tended to be younger and have fewer comorbidities than the average community based CHF patient. Previous studies using the SHF in patients with advanced heart failure, awaiting cardiac transplant, found the SHF moderately predictive of mortality although, as in our study, it tended to underestimate mortality risk.15
More recently, Nutter et al14 published a comparison of six different prognostic models in a cohort of elderly heart failure patients in order to predict 30 day mortality following acute admission to hospital. Each of the six models, including the SHF, significantly underestimated mortality, with marked variability between the models. Similar to our findings, this study highlights the practical difficulties of using such models to predict mortality in a typical high risk elderly CHF population.
Our study highlighted the association between abnormal renal function and increased mortality. Renal function is not included in the SHF. The reason for this is that the model was derived and later tested on patients without significant renal dysfunction. Consequently, the SHF may underestimate the importance of declining renal function in unselected CHF patients. Other studies have demonstrated the importance of renal function in predicting outcome in ambulatory heart failure patients.12 16–18 Brain natriuretic peptide added to the SHF has been shown to improve prediction of mortality18 and although we did not measure this, it is likely to add prognostic accuracy19 20 although in more elderly patients the predictive power may be less conclusive.21
Cause and place of death in end stage heart failure
Prior to death, these patients had very few heart failure hospitalisations, probably as a result of intensive and specialised care from the heart failure nursing team. Despite this high level of care, over half of our cohort (53%) died in hospital due to progressive heart failure and only nine died in either a hospice or respite care. There is clearly scope to reduce the number of patients dying in the acute hospital setting while increasing the number receiving more appropriate end of life care planning. It has been proposed by palliative care teams that CHF patients placed on a primary care register of palliative care are more likely to receive better end of life care22 but this remains untested in clinical trials.
Limitations
The total number of patients in this study was relatively small and it represents the experience of only a single health authority in Scotland with limited ethnic diversity. A recent study did highlight ethnic differences in mortality23 but our cohort was almost exclusively Caucasian and we are therefore unable to comment on any interaction between ethnicity and these prognostic tools. Despite this limitation, the cohort was selected on the basis of advanced NYHA class, representing the most severe symptoms and with the highest overall risk of death. Furthermore, as the patients were well known to the heart failure nurse team, this facilitated the decisions and judgements required to assess the GSF criteria. The patients, and the setting in which the study was performed, are therefore representative of those in other multidisciplinary heart failure services and the overall patient demographics are similar to those observed in the recent National Heart Failure Audit for England and Wales.24 The findings should, therefore, have widespread significance and applicability within this defined setting.
Conclusions
This study highlights the difficulty in predicting the last year of life in patients with CHF even where they are well known to the caregiver and where extensive clinical data are used to predict prognosis. Prognostic tools should be seen as complementary to careful clinical assessment with strong emphasis on the multidimensional needs of the patient and their family.
Key messages
Currently available prognostic tools are inaccurate in predicting last year of life in community based chronic heart failure patients.
What is already known on this subject
Advanced chronic heart failure is associated with poor prognosis and few patients receive appropriate end of life care. This is partly due to difficulty in identifying which patients are most likely to die within the next 12 months.
What this study adds
Two tools that are currently advocated as useful to identify patients approaching end of life, the Gold Standards Framework and the Seattle Heart Failure score, are not able to accurately predict mortality in an unselected cohort of ambulatory heart failure patients.
Appendix 1 The Gold Standards Framework Prognostic Indicator Guide
New York Heart Association (NYHA) stage III or IV heart failure
The ‘surprise question’ (to be asked of a healthcare provider familiar with the patient) “Would you be surprised if this patient died in the next 6–12 months?”
Repeated hospital admissions with symptoms of heart failure
Difficult physical or psychological symptoms despite optimised tolerated therapy
Appendix 2 Components of the Seattle Heart Failure Model
(1) Clinical information
Gender
Age
NYHA class
Weight (kg)
Left ventricular ejection fraction (%)
Ischaemic aetiology for heart failure
Systolic blood pressure
(2) Medications (yes/no for each)
β blocker
Angiotensin converting enzyme inhibitor
Angiotensin receptor blocker
Allopurinol
Statin
Aldosterone blocker
(3) Diuretics (mg)
Furosemide
Bumetanide
Torsemide
Metolazone
HCTZ
(4) Laboratory data
% Lymphocytes (lymph/total white cell count)
Haemoglobin (g/dl)
Total cholesterol (mg/dl)
Uric acid (mg/dl)
Total cholesterol (mg/dl)
QRS >120 ms
(5) Devices (yes/no)
Biventricular pacemaker
Implantable cardiac defibrillator
Biventricular pacemaker + implantable cardiac defibrillator
None
References
Footnotes
See Editorial, p 523
Linked article 301753.
Funding KH was partially funded by a bursary from the University of Edinburgh.
Competing interests None.
Ethics approval The study was granted ‘audit’ status by a member of the South East Scotland Research Ethics Committee and was therefore not considered to require full ethical review.
Provenance and peer review Not commissioned; externally peer reviewed.