Article Text

Abstract
Objective Advance care planning (ACP) is widely advocated to contribute to better outcomes for patients suffering from heart failure. But clinicians appear hesitant to engage with ACP. Our aim was to identify interventions with the greatest potential to engage clinicians with ACP in heart failure.
Methods A systematic review and meta-analysis. We searched CINAHL, Cochrane Central Register of Controlled Trials, Database of Systematic Reviews, Embase, ERIC, Ovid MEDLINE, Science Citation Index and PsycINFO for randomised controlled trials (RCTs) from inception to January 2018. Three reviewers independently extracted data, assessed risk of bias (Cochrane risk of bias tool), the quality of evidence (GRADE) and intervention synergy according to Template for Intervention Description and Replication. ORs were calculated for pooled effects.
Results Of 14 175 articles screened, we assessed the full text of 131 studies. 13 RCTs including 3709 participants met all of the inclusion criteria. The intervention categories of patient-mediated interventions (OR 5.23; 95% CI 2.36 to 11.61), reminder systems (OR 3.65; 95% CI 1.47 to 9.04) and educational meetings (OR 2.35; 95% CI 1.29 to 4.26) demonstrated a favourable effect to engage clinicians with the completion of ACP.
Conclusion The review provides evidence from 13 published RCTs and suggests that interventions that involve patients to change clinical practice, reminder systems and educational meetings have the greatest effect in improving the implementation of ACP in heart failure.
- palliative care
- systemic review
- health care delivery
- meta-analysis
Statistics from Altmetric.com
Introduction
The proportion of patients suffering from treatment refractory, end-stage heart failure is growing.1 These patients have significant palliative care needs.2 Advance care planning (ACP) is widely advocated as a way of addressing these needs and facilitating better end-of-life care.3–5 But studies show that clinicians often do not engage with ACP6–8 and patient care is affected. Patients might be motivated to discuss their care preferences and engage with future care planning, yet they require the cooperation of their clinicians.9 10 Interventions have been used in the past to change clinicians’ practice pattern.11 While the effect of interventions to engage patients with ACP has been systematically evaluated in systematic reviews,12 13 a rigorous assessment of the effect of interventions targeting clinicians is missing.
Furthermore, no past review considered a detailed analysis of different intervention approaches according to the Template of Intervention Description and Replication (TIDieR) in supporting clinicians in the delivery of ACP.14 TIDieR has been used to explain intervention content and how their components might change clinicians’ behaviour.15 Not investigating and understanding how interventions might work can hinder efforts to intervention design, replication and efficiency.16 The aim of this review was to synthesise the evidence for interventions with the greatest potential to engage clinicians with ACP in heart failure. The objectives were:
To determine the effectiveness of interventions targeting clinicians to engage with ACP in heart failure.
To examine which intervention components might be associated with intervention synergy and which might be not.
Methods
This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA-P),17 the Cochrane Collaboration reporting items for systematic reviews and meta-analysis,18 and the Grading of Recommendation Assessment, Development and Evaluation (GRADE) for the quality of evidence in selected trials.19 The description intervention content followed TIDieR and intervention effect was reported based on CONSORT guidelines.20 Online supplementary file 1 shows the review protocol.
Supplementary file 1
Eligibility criteria
We included only randomised controlled trials (RCTs) and cluster randomised controlled trials (cRCTs) of clinician-targeted interventions compared with standard professional development. We excluded studies that did not explicitly include patients suffering from heart failure or only dealt with the effect of the intervention on the implementation of ACP in paediatric but not in adult end-of-life care.
Studies were required to have a sufficiently detailed description of intervention components. Where this was not the case, we used the following approach: If the study identified that the intervention was a defined strategy, we searched online for details of the strategy and used these to classify the study components. Where insufficient details were available online, we contacted the authors directly, asking for a response by a given date. If the study seemed of interest but did not contain identifiable intervention components, we contacted the study authors with a template email asking them to provide any details they might have on the intervention.
Types of participants
We included studies of clinicians who worked in either primary or secondary care, the community or hospice setting and looked after patients suffering from heart failure. A clinician was defined as a person whose prime function was to manage a sick person with the purpose of alleviating most effectively the total impact of the illness on that person.21
Types of interventions
Clinician-targeted interventions were defined as interventions designed to bring about changes in the behaviour of healthcare professionals according to the Cochrane Effective Practice and Organisation of Care Group (EPOC) Taxonomy22 (online supplementary file 2). EPOC provides a common language to categorise intervention components targeting clinicians. There was no limitation in terms of theory informing the intervention, the person delivering the intervention (eg, research staff, trained clinician, social worker, counsellor, religious representative) or the healthcare setting. We included interventions that promoted the implementation of any type of ACP like advance directives, future care plans, durable power of healthcare attorney, living wills or healthcare proxies and interventions aimed at influencing professional practice by using patients as the agent for changing a clinician’s behaviour. ACP was defined as a co-ordinated and comprehensive approach of care for patients early, during or towards the end of suffering from a terminal illness.6 Authors had to explicitly state ACP intentions or this had to be evident in the composition of their study. Interventions that only looked at do-not-attempt-cardiopulmonary-resuscitation orders were excluded from the review because they on their own did not represent the complexity of ACP.23 Furthermore, interventions that were solely aimed at changing the behaviour of patients without affecting clinicians were not within the scope of this review.
Type of outcome
We selected a priori as our primary outcome the completion of an ACP document to determine whether a clinician engaged with the process of ACP as a result of the intervention. ACP completion rates related to any outcome that described data on the completion, recording or modification of any part of an ACP document. This outcome tended to indicate significant progress with discussing and deciding on various aspects of end-of-life care between clinicians and patients.
Search strategy
We searched the following databases from their inception until January 2018: CINAHL, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, Embase, ERIC, Ovid MEDLINE(SP), Other Non-Indexed Citations and Ovid MEDLINE(R), Science Citation Index, Social Science Citation Index & Conference Proceedings and PsycINFO. Together with a specialist health science librarian (NR), we used filters to reliably identify RCTs. A MEDLINE search strategy is presented in online supplementary file 3. We checked the reference lists of 15 relevant reviews and all potential cross references and records (online supplementary file 4). We contacted authors of main trials and experts in the field who were known to conduct research for additional papers or to provide missing or unpublished study data.
Selection of studies, data extraction and management
Titles and abstracts were independently screened against inclusion criteria by three reviewers (MS, IO, SB). Disagreements were resolved by discussion or referred for arbitration to a fourth author (BW). Full texts of screened papers were assessed for inclusion criteria and study quality. We pilot tested eligibility criteria and included a flow diagram of study selection and reasons for exclusion to conform to the PRISMA statement. We kept a list of excluded trials and documented reasons for exclusion in the ‘Characteristics of Excluded Studies’ (online supplementary file 5).
We assessed the overall quality of the trials’ methods by using the GRADE system V.3.6.1.24 A GRADE profile was created for each pooled estimate. Two authors (MS, IO) independently extracted data from papers and documented findings on a data extraction form. Two reviewers (SB, MS) independently coded interventions in each trial using the EPOC taxonomy.22 Online supplementary file 1 describes the intervention scoring and coding procedures.
Data analysis
We performed quantitative meta-analysis with RevMan V.5.3.525 using random-effects models and assessed publication bias by performing Egger’s test26 with STATA V.14.27 For individual studies with dichotomous data, we calculated ORs with 95% CIs between the intervention and control group as recommended by Cochrane.18 We calculated effect sizes for each EPOC category. Significance was set at p value <0.05. We conducted sensitivity analyses to explore the effect of trial quality on the primary outcome, to investigate reasons for heterogeneity and to assess the effect of outliers on the outcome data. We did not adjust sample sizes to account for clustering in the included cRCT28 as this study reported adjusted effect estimates, which took the intraclass coefficient found into consideration. We used a generic inverse variance approach and random-effects meta-analysis to include the estimate into the meta-analysis. When multiple time points were reported, we used the one closest to 3 months postintervention based on research practice in palliative care29 and the premise that it would require a reasonable length of time for ACP to take effect. We analysed the content, timing, frequency and synergy of clinician-targeted interventions that resulted in high and low effect sizes according to TIDieR.14
We assessed heterogeneity using the I2 statistic stating the percentage of variability in effect estimates that is due to heterogeneity rather than to chance.30 Thresholds for the interpretation of heterogeneity were based on Cochrane guidance18 as follows: 0% to 40%, might not be important; 30% to 60%, moderate heterogeneity; 50% to 90%, substantial heterogeneity; 75% to 100%, considerable heterogeneity. Two reviewers (MS, IO) independently assessed the risk of bias using the Cochrane Collaboration’s tool for risk of bias domains.31
Results
Of 14 175 articles screened, we reviewed the full text of 131 papers. Thirteen RCTs including one cRCT representing 3709 participants met all the inclusion criteria (figure 1). We excluded 102 studies with reasons provided in the ‘Characteristics of Excluded Studies’ (online supplementary file 5). A detailed description for each trial is presented in table 1.
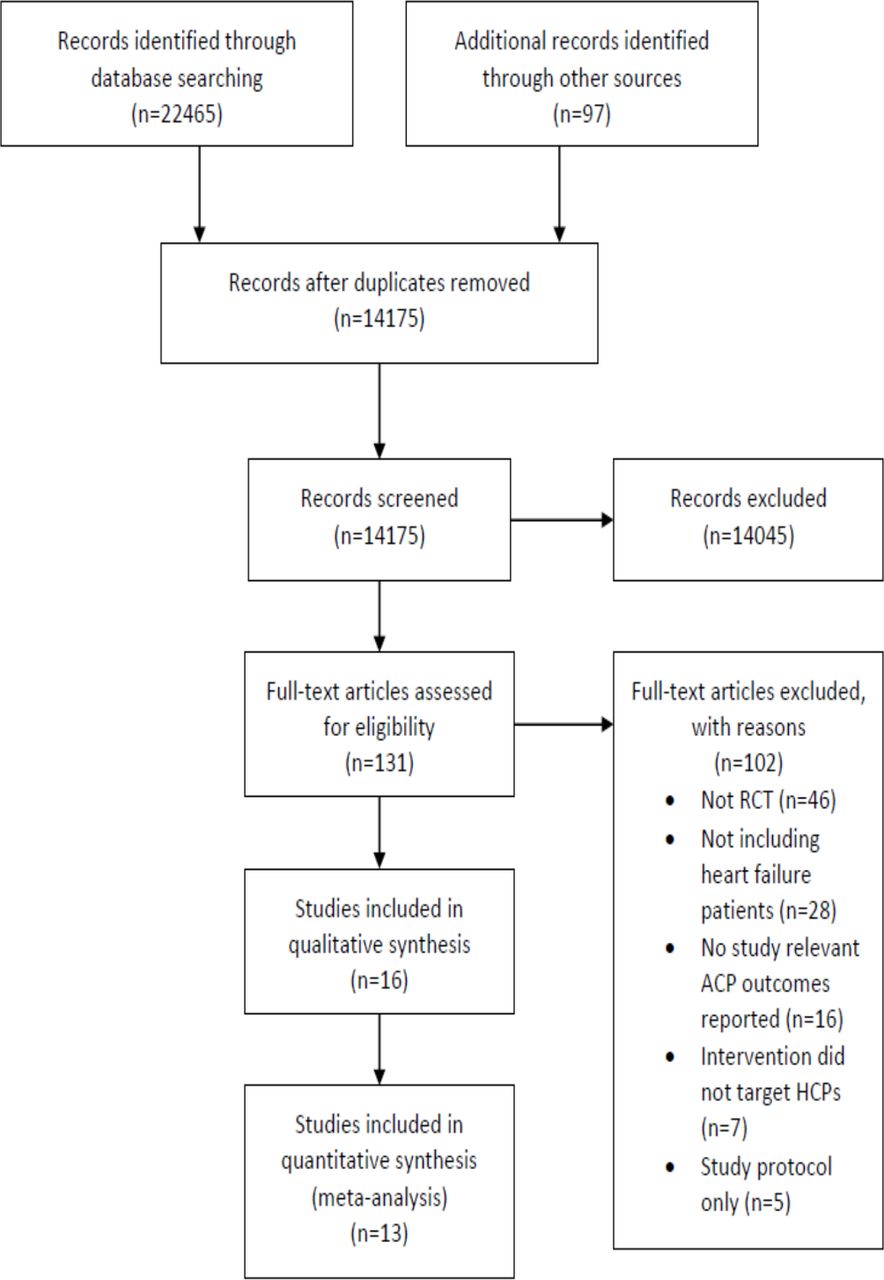
PRISMA flow diagram. ACP, advance care planning; HCP, healthcare provider; RCT, randomised controlled trial.
Characteristics of included studies
Characteristics of included studies
Twelve of the 13 studies were conducted in the USA and one in Australia.32 Nine trials were performed in a hospital setting, three studies in the community and one study involved hospital and community settings.33 All thirteen included studies using a RCT design. The one cRCT reported baseline cluster sizes at the practice level.28 The median sample size was 411 participants. The smallest number of participants randomised at baseline was n=29.34 The largest sample size was n=1101.35 The median follow-up period was 14.38 weeks (range from 1 week to 28 weeks).
Comparator to the intervention was standard professional development like chronic disease management for patients with heart failure. If clinicians were the target of the intervention, the control group was not included in the intervention training or exposed to any form of the intervention.
Risk of bias assessment
Key descriptors for the risk of bias assessment of the 13 RCTs are summarised in the risk of bias graph (figure 2) and presented for each study in online supplementary file 6.
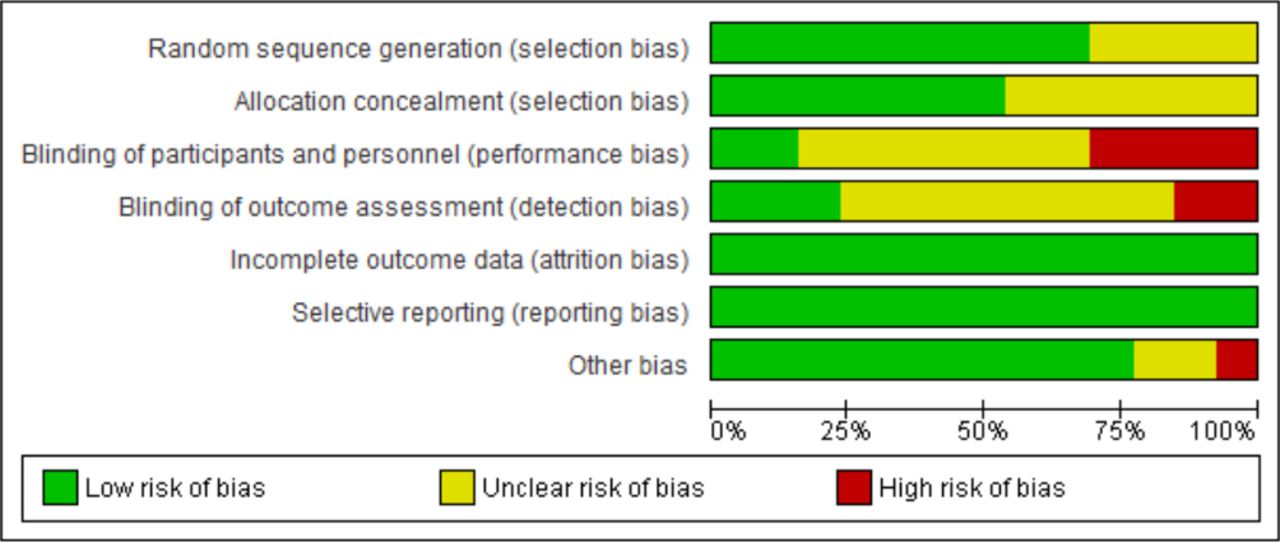
Risk of bias graph.
No trial reported inadequate methods of random sequence generation. Allocation concealment was unclear in six included trials as authors did not describe methods. Blinding of participants seemed not possible in four trials because of the nature of the interventions used resulting in a high risk of performance bias. Outcome assessors were likely to be aware of the allocation of participants to control or intervention groups in one trial.33 Incomplete outcome data (attrition bias) and selective reporting were adequately addressed in all studies. Eight patients from the control group of Sidebottom et al’s study received the intervention indicating issues with contamination.
Egger’s test and the inspection of funnel plot symmetry showed no evidence of a small study effect or publication bias for studies (n=4) including only patients with heart failure (p=0.117). Mixed study populations (n=13) demonstrated a small study effect (p=0.006) (online supplementary file 7).
Quality of evidence
The mean score for the overall quality of evidence across all studies was moderate after rating all GRADE criteria because many participants could not be blinded to the nature of the intervention. We identified four EPOC intervention categories targeting clinicians:
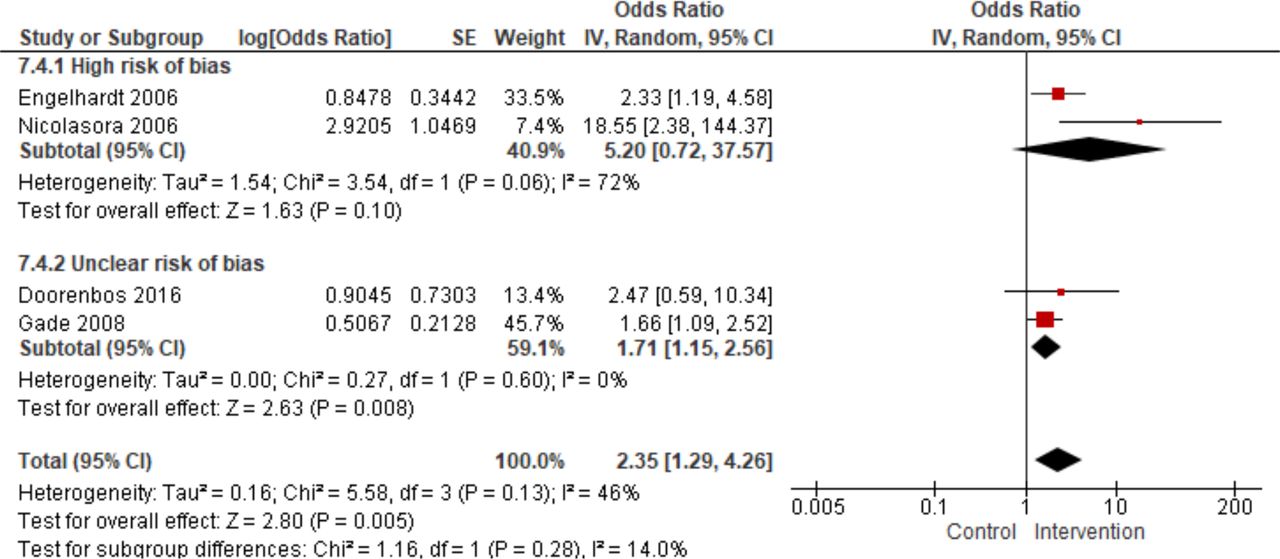
Patient-mediated interventions used patients to change clinicians’ behaviour had the greatest effect (OR 5.23; 95% CI 2.36 to 11.61, p<0.0001) on the implementation of ACP in heart failure (figure 3) followed by reminder systems (OR 3.65; 95% CI 1.47 to 9.04, p=0.005) (figure 4), educational meetings (OR 2.35; 95% CI 1.29 to 4.26, p=0.005) (figure 5) and academic detailing (OR 1.66; 95% CI 1.09 to 2.52, p=0.02).

Patient-mediated interventions.

Reminder systems.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Educational meetings.
Synergy of intervention components
Based on the effect sizes of included studies, table 2 provides a summary according to TIDieR of the most effective and the least effective interventions found in the review. The column labelled ‘Synergy’ considers how intervention components might have interacted with each other to determine higher or lower effect sizes. Interventions with the highest effect sizes included components that targeted clinicians and patients simultaneously to engage with ACP. The timing of the most effective interventions of engaging clinicians was nearly always during significant milestones in a patient’s disease trajectory. Typically, this took place before or after a hospital admission, before or after a change in the patient’s health status or in the context of a scheduled appointment.
Intervention synergy
Sensitivity analyses
Several sensitivity analyses including studies restricted to only patients with heart failure34 36–38 (OR 1.95; 95% CI 1.30 to 2.91, p<0.001, I2=0%), trials at low risk of bias32 34 37 39 40 (OR 3.17; 95% CI 1.30 to 7.76, p=0.01, I2=70%), and the exclusion of the three highest32 35 41 and lowest outliers37 40 42 (OR 2.99; 95% CI 1.97 to 4.51, p<0.00001, I2=0%) confirmed the consistency of the results of the primary analyses (online supplementary file 8).
Discussion
Previously, there was no firm evidence for the effect of clinician-targeted interventions to engage healthcare professionals with ACP in heart failure. This literature review and meta-analyses investigated 13 RCTs including 3709 participants and demonstrated that patient-mediated interventions (OR 5.23; 95% CI 2.36 to 11.61), reminder systems (OR 3.65; 95% CI 1.47 to 9.04) and educational meetings (OR 2.35; 95% CI 1.29 to 4.26) were the most effective intervention components. Academic detailing demonstrated only small effects (OR 1.66; 95% CI 1.09 to 2.52). Several sensitivity analyses confirmed the consistency of the results of the primary analyses.
Relation to other studies
This review is the first to analyse the effect of interventions targeting healthcare professionals on the delivery of ACP in heart failure in a meta-analysis. A number of reviews had investigated the effectiveness of interventions to implement ACP,12 13 43–47 but none focused on healthcare professionals or interventions with the greatest potential in changing clinicians’ behaviour in heart failure. For example, the review by Houben et al 12 only presented data on the efficacy of interventions targeting patients to improve the implementation of ACP but did not analyse which intervention components made a difference to clinical practice.
Our results concurred with findings from a number of Cochrane reviews on the effectiveness of interventions targeting clinicians. For example, we found that educational meetings were often combined with other interventions to maximise their impact. This finding agrees with a review by Forsetlund et al.48 They demonstrated that training clinicians was rarely used as a stand-alone tool and was nearly always combined with other techniques. A number of other Cochrane reviews had investigated the evidence base for the effect of reminder systems and academic detailing.11 49 Again, authors concluded that these interventions appeared effective in improving clinical behaviour across a number of settings preferably when combined with other methods. Their findings largely concurred with our results: reminder systems were always combined with other intervention categories. The strong effect sizes for and frequency of patient-mediated interventions was a surprise. Published data on the effect of patient-mediated interventions to improve professional practice were sparse.50
Strengths and limitations of the study
The strength of this review and meta-analyses consisted of the use of a robust search strategy, assessing the quality of the evidence with the GRADE system, rating risks of biases, pooling data across studies for each intervention category, exploring intervention synergy according to TIDieR and performing sensitivity analyses. The overall quality of evidence was moderate to low mainly due to a high risk of performance and detection bias. Egger’s test for the heart failure-only studies did not show any publication bias; the bias for mixed population studies was significant. This may have introduced a beneficial effect of the interventions compared with standard training. Almost all studies were based in the USA. This has implications of the generalisability of the results to other countries where different definitions and legal frameworks exist.
Using the EPOC taxonomy was an important first step towards providing a common language to describe intervention categories and attempt an analysis of intervention effectiveness. Among a number of categories, EPOC highlighted the importance of patient-mediated interventions, reminders and educational meetings to change clinicians’ practice. However, EPOC provided only a superficial level of detail in describing intervention content and application. This made their replication very difficult. TIDieR addressed that limitation to some extent by a more detailed consideration of the content, timing, frequency and synergy of interventions components. The content of the most effective interventions included multiple components that simultaneously targeted clinicians and patients to talk about ACP.
The right timing for a clinician to engage with and deliver ACP was often associated with significant milestones in a patient’s disease trajectory, for example, before patients had a scheduled appointment with their clinician,28 at the point of admission to a medical ward41 or after a recent hospitalisation.35 The involvement of patients as part of a strategy to change clinicians’ behaviour seemed even more important. This included interventions that provided support for patients and their families by enabling them to ask their clinicians questions about their care preferences and start the process of completing an ACP document.35 41 A lack of support of patients seemed predictably associated with lower effect sizes in the completion of ACP.40 42 A comparison between the studies of Rubin et al 35 and Reilly et al 40 highlights that fact. Rubin et al’s intervention might appear similar to Reilly’s components. But there were two significant differences: Rubin et al’s35 study included telephone support for patients for the duration of the study in case patients had any questions about their healthcare proxy form. Patients and family members could discuss their care preferences with their clinician before they completed the form in Rubin’s study. Reilly et al’s intervention did provide either of these.
Based on findings from the literature review, table 3 summarises intervention components with the greatest potential to change clinical practice according to TIDieR. These components, their content, timing and format might inform policy and be useful when considering the engagement of clinicians with ACP in routine clinical practice.
Clinician-targeted interventions
Conclusions
The review provides evidence from 13 published RCTs and suggests that interventions that involve patients to change clinicians’ behaviour, reminder systems and educational meetings have the greatest effect in improving the implementation of ACP in heart failure. Almost all studies were based in the USA affecting the generalisability of the results. However, findings may have the potential to be highly useful for services to consider how best to introduce ACP among healthcare professionals.
Key messages
What is already known on this subject?
Advance care planning (ACP) is widely advocated to provide better care at the end-of-life for patients suffering from heart failure.
However, clinicians appear hesitant to engage with ACP.
Interventions to better engage patients with ACP have been evaluated. But a systematic review and meta-analysis of clinician-targeted interventions is missing.
What might this study add?
Clinician-targeted interventions can help healthcare professionals to engage with ACP for patients suffering from heart failure.
Interventions that involve patients to change clinicians’ practice, reminder systems and educational meetings seem to be among the most effective approaches to facilitate ACP.
This effect was observed especially when the intervention simultaneously enabled both clinicians and patients to engage with ACP.
How might this impact on clinical practice?
Interventions that enable clinicians to engage with ACP in heart failure need to be developed.
Given the constraints of clinical practice, barriers and facilitators for a such a complex intervention need to be identified.
Patients with heart failure hold a key to change clinical practice and need to be enabled to engage clinicians with ACP.
Acknowledgments
We thank Nia Roberts, health science librarian, Bodleian Library, University of Oxford, for running the literature database searches.
References
Footnotes
Contributors The list of authors including the main author, MS, and the coauthors, BW, RP, IO, CA and SB, represents all those who can legitimately claim authorship by making a substantial contribution. MS had the idea for the review; wrote the protocol, extracted, evaluated and analysed the data; wrote, critically revised and submitted the entire manuscript. BW critically supervised the conduct of the review and revised the entire manuscript. RP critically revised the study protocol, the statistical meta-analyses and publication bias sections as well as the TIDieR analysis of intervention characteristics. IO independently screened papers, extracted data and evaluated risk of bias and study quality according to GRADE and the Cochrane risk of bias assessment tool. CA independently identified and coded and synthesised intervention evidence for the intervention synergy analysis. SB independently identified and coded Cochrane EPOC intervention components and synthesised the evidence for the intervention synergy analysis. All coauthors approved the version to be published.
Funding RP holds a grant from the UK NIHR Program of Applied Research for a different project during the conduct of the study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.