Article Text

Abstract
Objective Patient safety studies have identified older adults as a high-risk group for adverse events (AEs). As frequent users of the emergency department (ED), they are vulnerable to the negative consequences of ED crowding. The study objective was to determine whether a prolonged ED stay is associated with an increased risk for the occurrence of AEs for older patients admitted to hospital.
Methods This retrospective cohort study was conducted at the largest adult tertiary care facility in Atlantic Canada (1 July 2005–31 March 2006). All community-dwelling persons 65 years and older admitted to an acute inpatient unit from the ED were eligible. The exposure of interest was total length of stay (LOS) in the ED. The primary outcome was the occurrence of an AE in-hospital. AEs were identified from administrative diagnostic data using previously validated screening criteria.
Results The average age of 982 eligible participants was 77.8 years (SD 7.8). The majority (75.0%) experienced a prolonged ED LOS as defined by national guidelines. There was evidence of at least one AE in 140 (14.3%) records. After adjustment, for every hour spent in the ED, the odds of experiencing an AE in-hospital increased 3% (OR 1.03, 95% CI 1.004 to 1.05). Those with an AE had twice the hospital LOS (20.2 vs 9.8 days, p<0.00001).
Interpretation A prolonged ED stay for older admitted patients is associated with an increased risk of an in-hospital AE. The longer hospital LOS associated with AEs further reduces the availability of acute care beds, thus exacerbating ED crowding.
- Adverse events
- patient safety
- older adults
- emergency medicine
- epidemiology
- adverse event
- emergency department
- patient outcomes
Statistics from Altmetric.com
- Adverse events
- patient safety
- older adults
- emergency medicine
- epidemiology
- adverse event
- emergency department
- patient outcomes
Every major patient safety study of adverse events (AEs) has identified older patients (≥65 years) as a high-risk population, but little is known about the emergency department (ED) setting.1–5 Seniors are frequent and appropriate users of the ED. They are more likely to arrive by ambulance, have more acute illness, undergo more diagnostic tests and procedures, stay longer in the ED and be admitted to hospital.6 7 The ED poses unique challenges for older adults.
Superimposed on those challenges is the problem of hospital and ED crowding. International data suggest that a major cause of ED crowding is a lack of inpatient beds for admitted patients.8 9 There is a growing body of evidence demonstrating the relationship between crowding and poor patient outcomes.9–14 ED crowding has been associated with ambulance diversions, delays in care for time-sensitive conditions, increased ED and inpatient length of stay (LOS), the inadvertent spread of infectious disease and inpatient mortality.8–14 The objective of the study was to determine if a prolonged stay in the ED is associated with an increased risk for the occurrence of AEs in-hospital for older patients admitted to acute care.
Methods
Design and setting
This retrospective cohort study was conducted at the largest academic health sciences facility for adults in Atlantic Canada. The ED has an annual census of approximately 60 000 patients. The Capital District Health Authority Research Ethics Board approved the study.
Population
All community-dwelling persons 65 years and older who were admitted to an acute inpatient bed from the ED at the Queen Elizabeth II Health Sciences Centre between 1 July 2005 and 31 March 2006 were eligible for inclusion. To restrict the study population to relatively healthy, community-dwelling persons, patients with an ED visit or hospitalisation in the previous 6 months were excluded.
Length of stay in the ED
Using the Canadian Association of Emergency Physicians 2007 Position Statement Guidelines, a prolonged stay was defined as exceeding 6 h for those with emergent or urgent conditions and 4 h for those with less urgent or non-urgent conditions.15
Outcome measures
The primary outcome measure was the occurrence of an AE during an acute care hospital admission as identified by screening criteria developed by the Wisconsin Medical Injury Prevention Program (WMIPP). The screening criteria use a combination of ICD-9-CM diagnosis and external cause of injury codes applied to administrative hospitalisation data. In comparison with retrospective health record review by a clinician, a validation study determined the screening criteria were 59.9% sensitive (95% CI 42.8 to 75.0) and 97.4% specific (95% CI 94.1 to 98.8).16 In addition, geriatric-specific screening criteria were developed to identify hospital-acquired conditions: infection, delirium, fall-related injuries and pressure sores (Online Appendix 1). An acute hospital admission was defined as the time from leaving the ED to go to an inpatient bed until the patient was discharged from hospital, transferred to non-acute care or died. AEs identified in this study only include events that occurred in-hospital after the patient left the ED. Secondary outcome measures included the nature and type of AEs as well as disposition and hospital LOS.
Data sources
The cohort was identified through the electronic ED Information System and linked to data on hospital admissions. ED data included presenting complaints, ED diagnosis data and time intervals (eg, from arrival to admission). The hospital admission data included up to 19 diagnostic codes, in-hospital procedure codes, admission to the intensive care unit (ICU), disposition and LOS data (in-hospital and ICU). The inpatient diagnostic data were coded using ICD-10-CA. The Canadian coding system uses diagnosis-type indicators that allow for identification of pre-existing conditions (type 1 diagnosis) and conditions that arise after hospital admission (type 2).17 Two measures of hospital and ED crowding were calculated for the study period. The first was the “overcrowding hazard scale”, which tests the combined effects of hospital and ED crowding. The possible scores range from 1 to 9, with the higher score indicating greater crowding.14 The second was the “arrival density index”, designed to measure how busy the ED was when a patient arrived (ie, number of patients who arrived in the ED in the preceding hour for every patient). This is then averaged for all patients arriving on a calendar day.18
Data analysis
To detect a 10% difference in the proportion of older patients experiencing an AE between the two groups (prolonged stay or not), with a power of 90% and an α of 0.05, a sample of 354 per group was needed (total n=708). Differences between the groups were compared using the χ2 test for categorical data, an unpaired t test for normally distributed continuous data and the Mann–Whitney U test for data that were not normally distributed. A stratified analysis was performed for age and acuity using the Mantel–Haenszel technique to assess for effect modification.
Multiple logistic regression modelling was performed using manual forward stepwise procedures. Covariates were selected a priori for models on the basis of their clinical relevance and availability in administrative datasets (Online Appendix 2). The Elixhauser19 method was used to adjust for pre-existing co-morbidities using validated coding algorithms developed by Quan et al 20 to translate the Elixhauser diagnoses to ICD-10-CA.
LOS in the ED was first modelled as a dichotomous variable (ie, achieving time guidelines or not), and in a second set of models, as a continuous variable (ie, total LOS in ED in hours). The best-fitting models were achieved using ED LOS as a continuous variable. Goodness of fit was assessed with the Hosmer–Lemeshow test. Crude and adjusted ORs and 95% CIs were estimated. All analyses were conducted using STATA v.9 statistical software (STATA Corp., College Station, Texas).
Results
A total of 982 patients met the eligibility criteria (figure 1). This represents 10.5% of older adults who presented to the ED during the study period and 28.8% of those who were admitted to hospital from the ED. The majority of study patients (75.0%) experienced a prolonged stay in the ED as defined by Canadian guidelines. The average time from ED arrival to departure was 12.2 h (95% CI 11.5 to 12.8, range 0.6–64.3). Average daily hospital occupancy was 92.3% (95% CI 92.2 to 92.5). With respect to measures of crowding, the average overcrowding hazard scale during the study period was 1.9 (95% CI 1.85 to 1.9) and the average arrival density index was 7.6 (95% CI 7.3 to 7.9). The baseline characteristics of the two groups (prolonged stay in the ED or not) are presented in table 1. The majority of patients were discharged home (81.3%) despite an average hospital LOS of 11.3 days (95% CI 10.4 to 12.2 days). Only 3% were discharged to long-term care. There were 136 in-hospital deaths.

Patient flow through the study. ED, emergency department.
Baseline characteristics in 982 patients ≥65 years of age admitted to acute care in a tertiary hospital from the ED in an 8-month period
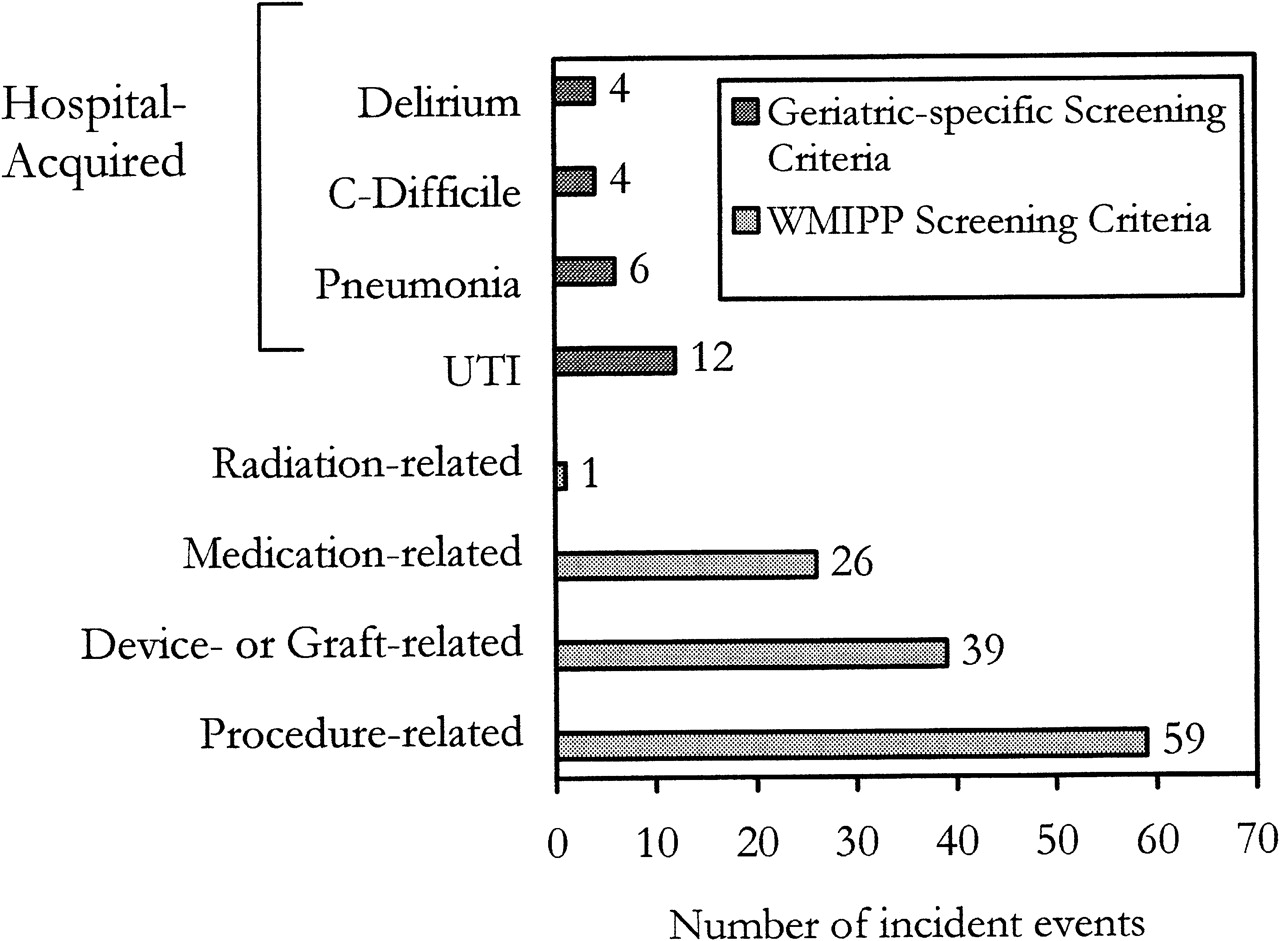
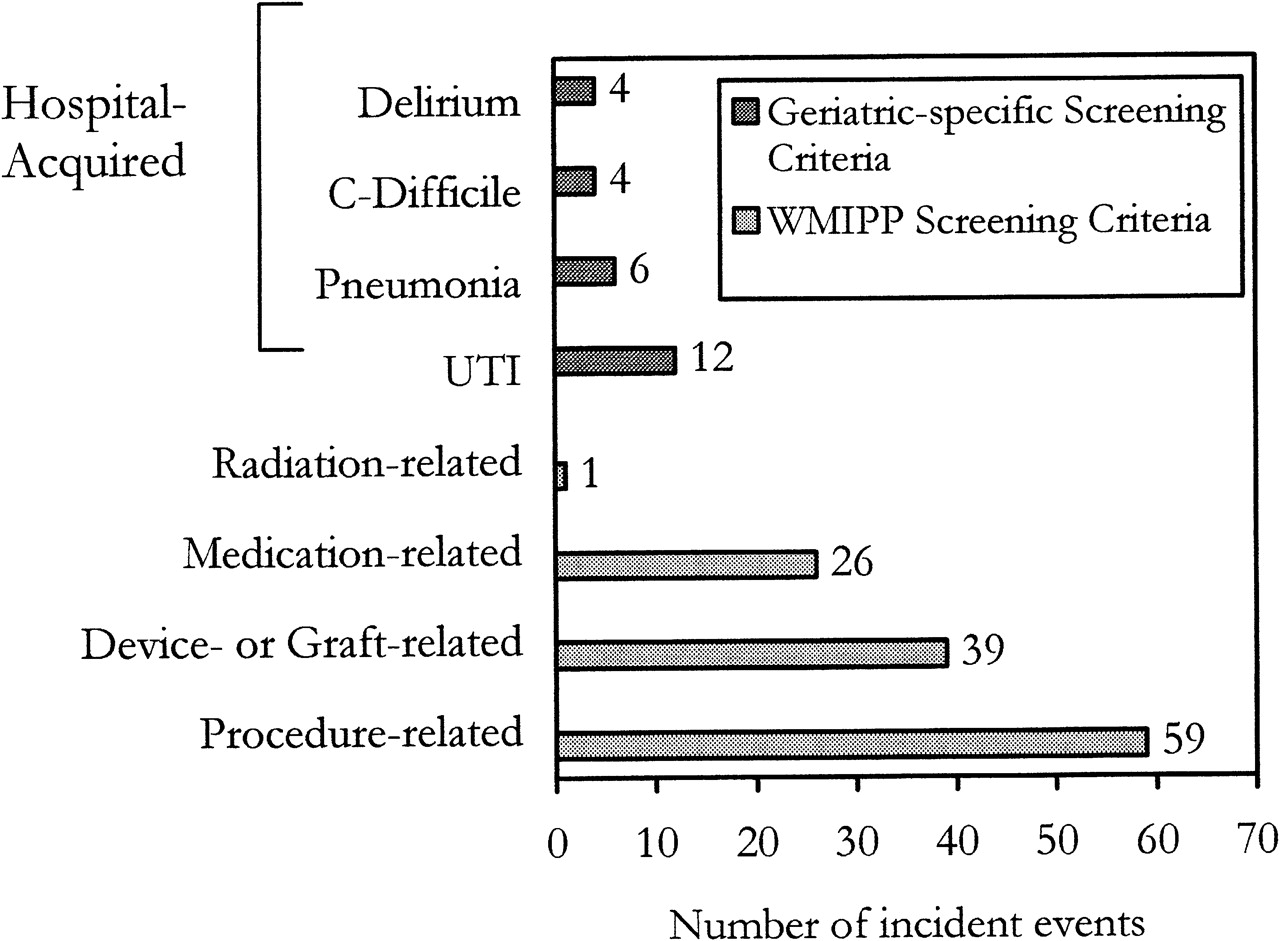
Of the 982 patients, 140 (14.3%) had evidence of an AE. One hundred and twenty-five (89.3%) were identified using the WMIPP criteria (table 2) and 15 records (10.7%) had codes consistent with a geriatric-specific AE.
Types of adverse events identified by the Wisconsin Medical Injury Prevention Program screening criteria in 125 patients ≥65 years of age admitted to acute care in a tertiary hospital from the emergency department in an 8-month period
There were 11 records (7.9%) with evidence of both types of AEs (figure 2). The average number of AEs was 1.6 (95% CI 1.4 to 1.7). There was no evidence that any of these conditions existed before hospital admission. Those with an AE had twice the hospital LOS (20.2 vs 9.8 days, p<0.00001). After adjustment for age, gender, pre-existing co-morbidities, admission to an ICU, having a surgical procedure, hospital LOS, illness acuity and severity, the total LOS (hours) in the ED was associated with an increased risk of any single AE (OR 1.03, 95% CI 1.004 to 1.05), a medication-related AE (OR 1.04, 95% CI 1.01 to 1.08) and the occurrence of multiple AEs (OR 1.05, 95% CI 1.02 to 1.09). Table 3 presents the adjusted results for multiple AEs, a potentially worse outcome than a single AE.
{kind=link}
{kind=link}
Number and types of adverse events. UTI, urinary tract infection; WMIPP, Wisconsin Medical Injury Prevention Program.
Patient-related and system/environment-related factors for multiple adverse events in patients ≥65 years of age admitted to acute care in a tertiary hospital from the ED in an 8-month period
Discussion
Seventy-five per cent of the study patients experienced a prolonged stay in the ED as defined by the recommended Canadian guidelines. After adjustment, the ED LOS was associated with an increased risk of AEs. Although the risk estimates appear modest, the odds increase 3% for any single AE, 4% for medication-related AEs and 5% for multiple AEs for every hour spent in the ED. In the current study, there were large baseline differences between those with and without a prolonged stay. The results suggest that the system of dealing promptly with high-acuity patients is generally effective. There was no difference in hospital disposition, LOS or mortality between the groups.
Slightly more than 14% of the study patients experienced at least one AE during their inpatient stay. Studies have described age-adjusted incidence rates in older patients ranging from 5.9% in the USA to a high of 40.7% in New Zealand.1 5 The current study included a homogeneous population of relatively healthy, community-dwelling seniors. It is likely the incidence would have been higher if frailer patients had been included in the study. Patients who experienced an AE had twice the hospital LOS as those patients who did not, and these additional days were spent in acute care. Lack of inpatient beds has been identified as a major contributing factor to ED crowding, a finding often attributed to patients awaiting long-term care placement.8 9 However, data from the current study suggest that the occurrence of an AE in-hospital may also make a significant independent contribution to reducing the availability of acute care beds, thus potentially exacerbating ED crowding. The nature of the causal relationship between AEs and hospital LOS is complex. Hospital LOS was included as a covariate in adjusted models to statistically control for its potential contribution to the occurrence of an AE. Further study is needed to elucidate the nature of this relationship.
Data on time spent in the ED for study patients clearly support that crowding is an issue. A Canadian study examined the relationship between hospital occupancy and ED crowding. It was determined that ED LOS for admitted patients was associated with hospital occupancy (p<0.01) and that most of the increase happened when hospital occupancy exceeded 90%.18 In the current study, the average daily hospital occupancy was 92.3% and the average arrival density index was 7.6—both figures are highly consistent with the findings by Forster et al.18 In a study of Australian inpatients, a clear linear relationship was demonstrated between an overcrowding hazard scale score of greater than 2 and inpatient mortality, even after adjusting for age, diagnosis, referral source, urgency and mode of transport to the hospital.14 On average, the overcrowding hazard scale in the current study did not exceed 2. This may explain, in part, why ED and hospital crowding measures did not contribute significantly to the adjusted estimates.
Although a causal relationship has not been established, there are a number of factors that may have contributed to the positive association found between ED LOS and the occurrence of AEs in-hospital. These factors include prolonged immobility on a stretcher, potential exposure to infectious agents in the ED, the disorienting effects of noise and lighting conditions in a busy ED for an extended period of time, care by multiple providers, and potential delays in diagnosis and/or access to specialised inpatient care.6 21–23 Although already compromised because of acute illness, the overall physiologic reserve of the patient may be further diminished by a prolonged stay in the ED, thus tipping the balance towards an increased risk of experiencing an AE. The genesis of an AE may be related to conditions and factors in the ED; however, it may not manifest itself until the patient is in the inpatient unit (eg, pressure sore from extended immobilisation on a stretcher). A prolonged stay in the ED extends exposure time to contributing factors. Alternately, an AE may occur in the ED but not be identified until the patient is admitted to the hospital (eg, adverse drug event).
Much of the early patient safety literature emphasised identification of error; however, the screening criteria are based on an alternate focus on identification of injury.24 The different paradigm is important because it opens up new approaches to identification of AEs, including the use of diagnostic codes in administrative data. This approach should not replace other strategies; however, it can ensure efficient use of scarce resources by identifying priorities for focused attention.
Limitations
This is the first study to apply the screening criteria outside of the USA. It has demonstrated the feasibility of using routinely collected data to screen for AEs. Although their sensitivity is less than optimal, more sensitive measures of detection are prohibitively resource intensive. The screening criteria were validated using ICD-9-CM. Cross-walk tables were used to translate ICD-9-CM codes to ICD-10-CA. Further research is needed to validate the WMIPP criteria in non-US settings as well as to refine and validate the geriatric-specific screening criteria. There is evidence of some selection bias in the study in that sicker patients had a shorter LOS in the ED. However, illness acuity, severity and co-morbid conditions were controlled through a number of covariates in the regression models.
The results are likely an underestimation of the problem. In addition to the limited sensitivity of the screening criteria, the approach does not permit the identification of diagnostic-related AEs or any events that are not documented (thus, not coded). Although the findings from a single tertiary care facility can only be generalised to a similar study population and setting, the potential vulnerability of older adults to AEs in healthcare is relevant regardless of hospital type, size or location, and merits further research.
Conclusion
According to national guidelines, a majority of patients spent too long in the ED. Moreover, a prolonged stay in the ED for older admitted patients is associated with an increased risk of an AE in-hospital. The longer hospital LOS associated with AEs further reduces the availability of acute care beds, thus exacerbating ED crowding. As the evidence grows on the deleterious effects of hospital and ED crowding, this issue must be viewed as a credible and growing threat to patient safety.
Acknowledgments
The authors gratefully acknowledge the contributions of Drs Pat Croskerry and Peter Layde and the invaluable assistance of the Decision Support staff at Capital District Health Authority.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
Funding Financial support for doctoral studies (SA-S) was received from the Canadian Institutes of Health Research (Ottawa, Ontario, Canada) Strategic Training Fellowship Program (Transdisciplinary Understanding and Training on Research-Primary Health Care (TUTOR-PHC)) and from the Nova Scotia Health Research Foundation (Halifax, Nova Scotia, Canada). The funding agencies did not play a role in the study design, data collection, analysis or interpretation.
Competing interests None.
Ethics approval This study was conducted with the approval of the Capital District Health Authority, Halifax, Nova Scotia, Canada.
Provenance and peer review Not commissioned; externally peer reviewed.