Article Text

Abstract
Background Bereaved people need a supportive response from those around them. Knowing children’s and surviving parents' needs following parental death is the first step to ensuring a supportive response. However, no systematic review has reported on this phenomenon.
Aim To systematically identify and synthesise qualitative literature exploring support experiences of parentally bereaved children and surviving parents.
Methods Systematic review with thematic synthesis, following Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. MEDLINE, Embase, PsycINFO, CINAHL and the British Nursing Database were searched for relevant papers to September 2021. Included studies were appraised for quality and thematically synthesised using Thomas and Harden’s thematic synthesis framework.
Results Fifteen qualitative studies from nine countries were included. There were four analytical themes from the children’s perspectives (1) Openness of communication with children about death and dying, (2) Children’s challenges of managing change, (3) Navigating emotions, and (4) Children’s acceptability, access and engagement with support. There were three analytical themes from the parents' perspectives: (1) Adjusting as a parent, (2) Supporting their children, and (3) Parent’s acceptability, access and engagement with support.
Conclusions Following a parental death, open and honest communication and involvement in what is happening within the family will help children cope. Both children and parents suppress emotions and avoid conversations to protect each other and those around them. A taboo around death exists and constrains the support some families receive. Childhood bereavement is a public health issue, with a need for professionals and communities to better understand and respond to the needs of bereaved families.
CRD42020166179
- bereavement
- communication
- family management
- terminal care
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Bereaved children need a supportive response.
Research must understand how families are supported.
WHAT THIS STUDY ADDS
Children hide grief to protect themselves and friends supporting them.
Support from family’s social networks quickly dwindles.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Parents need guidance to communicate with and support their grieving children.
Research involving children is essential to understand their needs.
Introduction
Children are not protected from death, with many experiencing the death of someone close to them.1 In the UK, a dependent child is bereaved of a parent every 22 min.2 Meanwhile, it has been estimated that 1 in 14 children in the USA will experience the death of a parent or sibling by the age of 18.3 The COVID-19 pandemic has brought death to the forefront of our society,4 with 5 200 000 children worldwide experiencing the death of a primary caregiver to COVID-19.5
Children who experience a parental death are at greater risk of adverse reactions and behaviours, including aggression, despair, anxiety, depression, disruptive behaviours, social isolation, post-traumatic stress disorder and suicide.6–8 Death can cause distress and life changes, and requires adjustments for the bereaved, who draw on their inner resources alongside support from their family and existing networks.9
Bereavement should be understood as a universal issue, acknowledging the individuality of experience and how a child’s social conditions may impact their bereavement.1
Bereaved children require a supportive response from their existing networks; who also need information about how children grieve, what can help, when to seek more support and what services are available.10 Some children will need one-to-one, family, peer or group support, and a few children will need specialist support.10
Evidence suggests that childhood bereavement should be placed within a public health approach to bereavement care to allow a better understanding and response for bereaved children.1 Such an approach emphasises the response of social networks and communities to the bereaved, understanding that bereavement care should be shared between communities and health services based on individual needs.11
However, there are significant gaps in child-centred research,12 particularly on sociological perspectives of bereaved children and surviving parents and how best they can be supported.1 Therefore, this review aimed to systematically identify and synthesise qualitative literature on the support experiences of parentally bereaved children and surviving parents.
Methods
A systematic review was conducted. The review followed an a priori protocol (PROSPERO Registration ID: CRD42020166179) and was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols 2009 guidelines.13
Search strategy
A detailed search strategy was developed in Ovid MEDLINE (AW, SG) (online supplemental table 1) and adapted to other databases, including Embase, PsycINFO, CINAHL (Cumulative Index to Nursing and Allied Health Literature) and the British Nursing Database, using both Medical Subject Heading terms and text word searches to increase inclusivity. Searches were undertaken in January 2020 and updated in September 2021.
Supplemental material
The search strategy combined three concepts: (1) The populations of children, adolescents, young adults, parents, widows and surviving parents, (2) The phenomenon of bereavement and death, and (3) The support experiences and needs.
Grey literature searches using Google Scholar and OpenGrey identified research not indexed in the electronic databases. Forward and backward citation searching of included studies was used to supplement the search: reviewing references and identifying any forward citations via Web of Science.
Study inclusion and exclusion
Only studies relevant to the review aim were included (table 1). No minimum age criteria were set to develop an understanding of all research undertaken with bereaved children and what different age groups have participated. No restrictions were placed on the year of publication to allow a comprehensive understanding of the literature.
Study inclusion and exclusion criteria
Screening process and study selection
Screening and study selection were conducted by four authors (AW, BP-S, SG and OB). Covidence software14 identified any conflicts during screening, which were discussed with two authors or mediated by a third author (JWB).
Quality appraisal and data extraction
The Critical Appraisal Skills Programme guided the quality assessment of studies15 (online supplemental table 2) and was independently carried out by AW and SG. Studies were not excluded based on the quality assessment,12 16 as there is no evidence to suggest this improves the quality of the review,17 and it may exclude those studies with relevant results but low reporting quality.18 Data from included articles were extracted from Covidence by the first author (AW) and independently verified by a second author (SG). Full-text papers were uploaded to NVivo software.19 The results sections of the included studies, participant quotes and any text describing findings were included as data for synthesis.
Supplemental material
Data synthesis
Data were analysed using thematic synthesis, which involved three stages.20 First, findings from each study were coded line-by-line by the first author (AW), and then similar codes were organised into descriptive themes which remained close to the data. Lastly, new analytical constructs were constructed by exploring patterns, similarities and differences in the descriptive themes, and interpreting those in relation to the review aim. Discussions between the research team (AW, SP, BP-S, FM, BW and JWB) facilitated mutual agreement on the descriptive and analytical themes developed. Children’s and parents' perspectives were analysed separately.
Results
Search results
The searches yielded 16 130 articles, from which 5829 duplicates were removed (figure 1). Titles and abstracts for the remaining 10 301 studies were screened for eligibility, and 9997 papers were excluded. Full texts of the remaining 304 studies were screened for eligibility, and 289 papers were excluded. Fifteen studies were eligible for inclusion. The 15 qualitative studies were published between 1975 and 2021 and conducted in nine countries: USA (4), Canada (2), Denmark (2), UK (2), Iran (1), South Africa (1), Sweden (1), Taiwan (1) and Uganda (1). Culture can influence how bereavement and grief are dealt with in relation to help-seeking and coping and cultural traditions surrounding death, bereavement and mourning.21 Furthermore, social and welfare systems and policies vary drastically between countries, affecting how children are supported. For example, Danish schools have bereavement response plans which guide how to respond to grief and what needs to be done to support a child following a bereavement.22 In contrast, children bereaved in Uganda have little school and other resources available to them due to the country’s limited domestic funds and health infrastructure.23
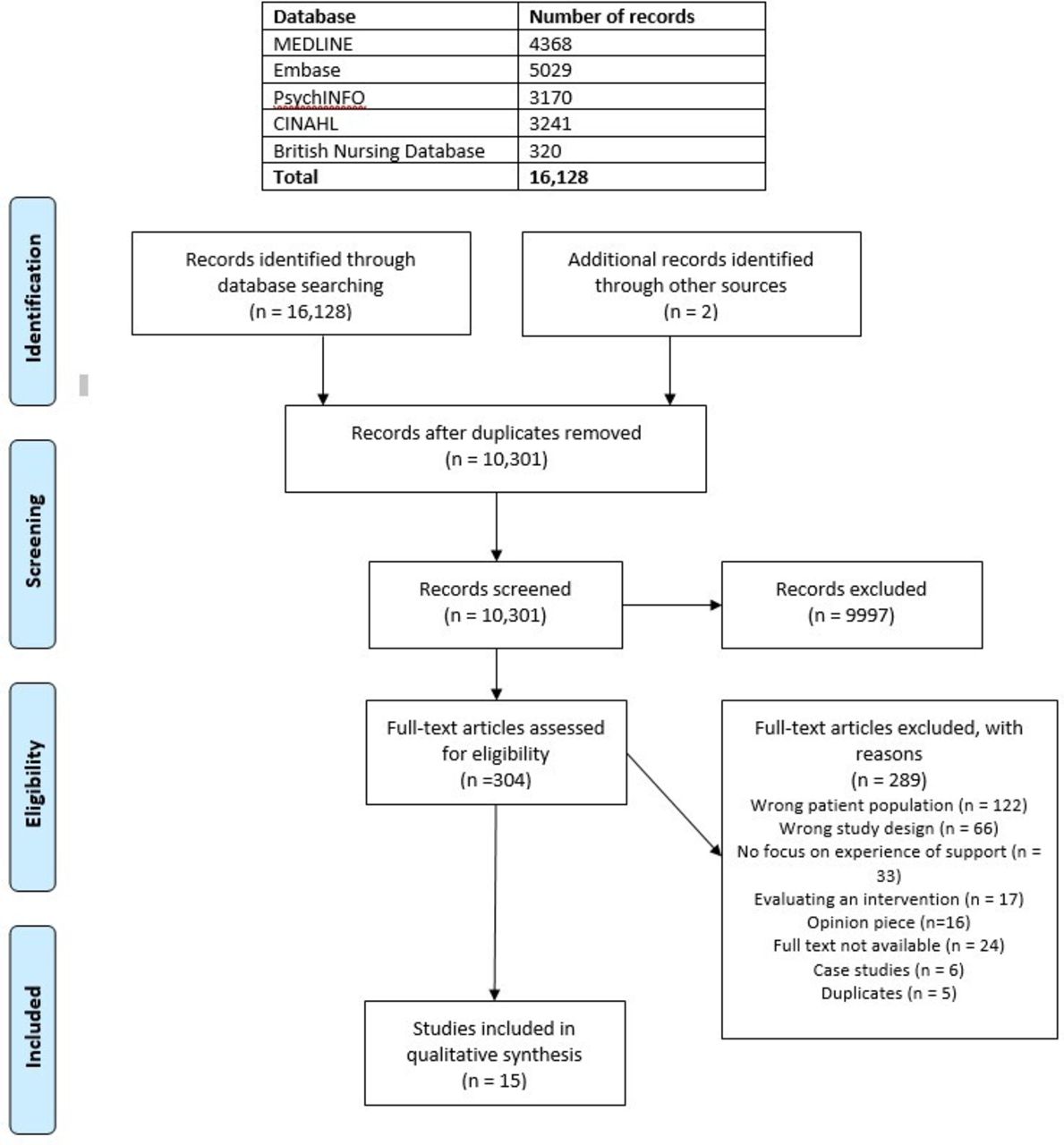
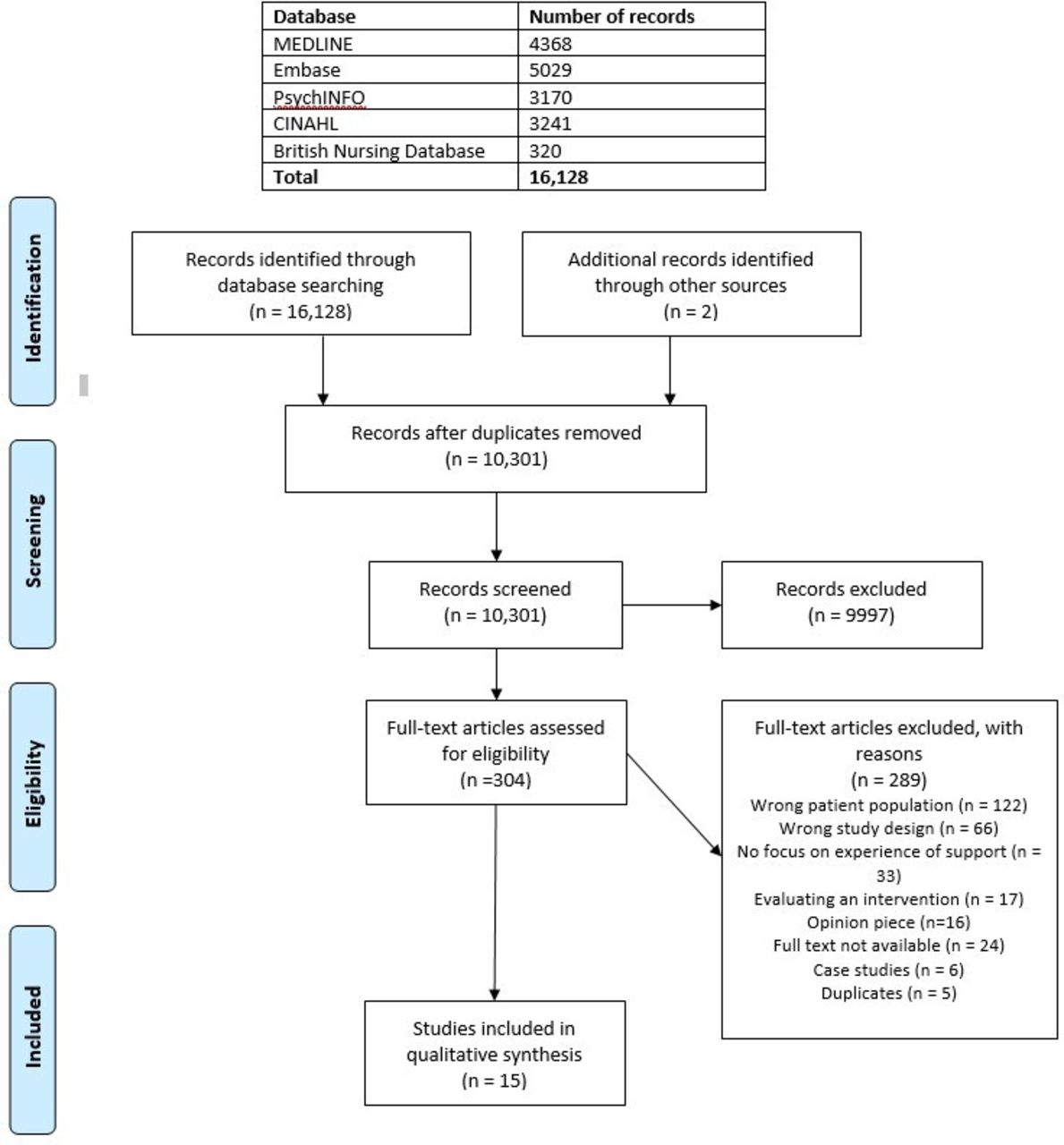{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).
Seven studies collected data directly from children,23–29 three collected data from children and parents,30–32 and the remaining five collected data from parents only.33–37 Sample size ranged from 4 to 39 participants per study, with 210 child participants aged 6–18 years (female=80, male=56, gender not stated=74) and 57 parents included. Not all studies reported the number of parent participants.30 31 Children and parents were interviewed between 2 months to 13 years after their bereavement. Studies interviewed children alone,26–28 or with parents present.32 For most studies, it was not clear who was present. The full characteristics of the included studies can be found in online supplemental table 3.
Supplemental material
Overview of developed themes
Descriptive themes were developed and further categorised separately into four broad analytical themes relating to children’s perspectives of support (table 2), and three from the parent’s perspective (table 3).
Child perspective themes
Parent perspective themes
Children’s perspective of support
Openness of communication with children about death and dying
The preparation and communication children received regarding parental death varied across the studies. Open communication allowed time together, acknowledging the reality of the impending death.23 30 31 However, the death was a shock, even when forewarned.23–25 30 Being unprepared left children feeling isolated,23 25 30 even children who witnessed the death felt isolated and dissociated from what was happening.23 24
Following the death, some children were quickly informed,29 while others were not told until after the funeral.23 25 Reasons for delaying included a desire to protect the child and beliefs that children were too young to understand.23 24 Unhelpful euphemisms for death, such as 'going to sleep', 'he’s gone', 'he’s up there'25 30 were frequently used, with families often avoiding conversations, leaving children with unanswered questions about death, with some blaming themselves for the death.29
Regardless of their cultural backgrounds, children appreciated open communication within the family about their experiences and grief.24 29 Expressions of feelings and offers of support were helpful.32 Children from studies published in the UK, Canada and South Africa were helped when given information and involvement in funerals, viewing the body or planning to return to school.25 28–31 This was not mentioned in other studies. However, it is important to note that the way children are involved in communication and death rituals varies by culture. Seeing their parent helped children stop feeling scared, offered a chance to say goodbye and helped them to accept the finality of death, often described as a relief.25 29 30 Children appreciated friends and teachers attending the funeral and took comfort in the number of people present.25
Review findings further showed that many children enjoyed returning to school and appreciated friends acknowledging their loss and showing they cared.27 28 31 Some found it overwhelming, and others had no acknowledgement of their loss from peers and teachers.28 Empathy from peers made children feel less isolated and different.27 It was important to children that peers were authentic and approached their loss naturally and genuinely.27 Children sensed the taboo around death.28 For many peers, this was their first encounter with death,24 27 and the lack of knowledge and experience about death and grief was often felt.24 25 27 28 31 Peers were often unprepared to deal with their grief, not knowing what to say or how to react, adding to their isolation.24 27 28 This led some to withdraw from their social circles.29 Half the children in the Ugandan study were no longer attending school; some had to take on caring roles within the family and others had no money for school fees.26
Most children found that speaking with bereaved peers who could empathise, and relate to their loss, helped them cope by normalising their experience.24 27–31 Siblings were an important source of support, sharing similar emotions.30 Peers who had experienced parental divorce could empathise and understand somewhat the internal and social experience of losing a parent.27 However, children recognised that others who had not experienced a catastrophic loss could not understand the impact, making it more difficult to talk to them.27 28 30 31
Children’s challenges of managing change
Children returned to school while their families remained in disarray, experiencing drastic change, uncertainty and instability.27 28 Children reflected on changes to their perceived identity; they felt different from peers and were perceived as such, either 'fatherless' or 'motherless'.23 25 27 28 Increasing feelings of isolation made children feel incomplete, experience discomfort and unease, feel less than others, and embarrassed.23 27 28 Some hid the death, so they were not different and did not have to talk about their loss;23 24 27 29 they feared being rejected, causing upset or showing emotions.23–25 27 30 31 Children perceived they were treated differently, avoided, excluded from play or ignored because they were different.27 28 Some were treated as normal as if it had not happened, which helped.27 28 Although some were able to speak to peers about how they felt and were well supported,25 28 30 31 others refused to discuss the death with anyone.23 27 Conversely, for some the worst response was too much attention; they appreciated others' empathy, but perceived unwanted physical contact, excessive questioning and being forced to talk about their loss as uncomfortable.27 28
Children redefined their new normal, experiencing further losses and yearning for what they had lost in their deceased parent.23 25 29 32 Some moved home,23 25 26 and relationships and roles changed.25 27 28 Those orphaned faced increased responsibilities, lacked stability, lost childhood, education, future hopes, and worried about who would care for them.26 Children who were living with different relatives often felt unwanted.25 26 Some experienced family conflict, social stigmatisation, and physical and emotional abuse.23 26 Social stigmatisation or being treated differently because of their bereavement was not found to be related to the cause of death or country.23 26–28
A consistent relationship with their parent or another adult was crucial.24 31 However, relationships with their parents changed, the family restructured itself, and their individual and family needs could not be met in the same ways, with strains on relationships.23 32 Some felt fortunate to have a parent to care for them29 and had a strong need for their attention.32
Navigating emotions
Family dynamics changed following a parental death, resulting in insecurity and worry.23 25 Some children saw parents struggling, hearing them secretly crying, failing in their new roles, and witnessing psychological breakdowns, including self-harm, attempts of suicide and depression.23 Some children modified their behaviour and were 'good' to prevent their parents from becoming upset,25 or did more to help their surviving parent.29 30 32 Others acknowledged how well their parents coped and adapted to their new roles.25
Many children suppressed their emotions23 25 27 30 32 and felt isolated, grieving alone.23 30 Children’s reactions to grief were individual and included physical, behavioural, emotional and spiritual reactions, while some showed little or no emotion at times.24 29–31 Some children struggled to understand that their grief responses and needs differed from their siblings, while others recognised that grief is unique and individual.31 Some children believed that managing their emotions, clarifying values and goals, accepting what had happened, and coping strategies contributed to their psychological well-being.24 Following their loss, some children found they expressed their own emotions more and were more thoughtful of the needs of others, with increased sympathy and sensitivity towards others' feelings, especially their immediate family, which brought them closer together.24 32
Children’s acceptability, access and engagement with support
Some children found their grief was a constant companion, never going away, and worsening at times, while others found it took time to recover, accepting they would always miss their parents.24 28 Children in the studies reported the support they received did not match their needs and quickly dwindled28 and their loss was soon forgotten by others.28 Children missed being asked how they were and needed to know that people still cared.28 Children felt teachers lacked awareness, resulting in insensitive and unintentional hurtful comments or situations.23 28 31 However, some described teachers' understanding of grief and ongoing support in remembering birthdays and anniversaries.28 31 Such children highlighted the school as a good source of support, a safe place, providing a sense of belonging, routine and emotional escape through extracurricular activities.24 25 28 31
Children did not always understand the sources of support, and their perceptions of who should or could support them varied, including parents,27 31 themselves or friends.27 Professional support, although mentioned infrequently, was described as helpful. Children described professional support from counsellors, psychologists and the healthcare professionals caring for their parent.24 30 31 Professionals were seen as helpful when they were being honest with them, checking on their well-being, helping them develop coping strategies, being open and flexible to their needs, and being available quickly.24 30 31 Although children wanted professionals to converse with them, it was important that they were not forced to talk.30 Some children appeared unaware of professionals as a source of support.30
The most helpful types of support came from people who were well known to children before their loss.23–25 27 28 30 31 Friends knowing the deceased parent provided special conversational support, as it was easier to talk to them and share memories.27 Children also felt more secure speaking with close friends, with less worry of being teased or hurt.27
Distraction with friends helped children cope by offering a temporary escape and emotional release.27 29 31 Usual routines provided security and stability, explaining why many children wanted to return to school soon after their loss.25 29 31
Continuing a relationship with their deceased parent provided comfort and helped children cope.23–25 29–32 Relationships were maintained using mementoes to keep their parent’s legacy and memory alive,29 31 and speaking to the deceased in the present, letting them know what was happening in their lives, and asking for advice or protection provided comfort, stability, unity and a sense of belonging.23 25 29 32 Some children hid these conversations as they did not want to make others upset or were from a culture where discussing death was discouraged.23 Remembering them together with happy and positive memories, avoiding talking about sad or scary times that made them feel sad or distressed,32 or having an image of the deceased helped some feel more whole, filling the void their parent left.23
Some children were comforted and supported by their faith and belief in an afterlife, sensing God’s presence helping them overcome their problems.24 25 29 30 In contrast, other children lost faith, felt angry and blamed God.24 26 29 Some of the children who initially lost faith found later that their faith did help them overcome the trauma, and they subsequently felt a stronger relationship with God.24
Parent perspective themes
Adjusting as a surviving parent
Review findings showed that parents lost their 'normal' lives, family dynamics changes and they were forced into life as single parents.32–37 Parents felt heavy demands on their time and mental resources, struggling to share their time between their children, which often led to arguments and misunderstandings.32 33 Other parents had too much time, leaving them feeling alone, frustrated and craving companionship.33 35 36 Fathers' jobs were often incompatible with childcare, meaning some changed working hours, jobs or stopped work altogether.33 35 Some parents found that previous social networks disappeared altogether. They were treated differently by friends, with one common explanation being that friends felt uncomfortable.34 35 37 These reactions were unexpected, leaving parents feeling abandoned and let down.34 37 Not all parents had this experience; some had continued and sustained support from friends.34 37
While adjusting to new parental roles and family life, parents were grieving themselves. It was challenging and took time to accept their loss and address their new realities.33 34 36 Parents had sole responsibility for their children, which was often daunting and scary; parents felt alone, helpless and vulnerable, struggling to make decisions.33–37 Parents worried about what was best for their children. Some questioned most decisions they made for fear of getting it wrong; some turned to extended family or others for advice.35 36
Parents considered their mortality and re-evaluated how they lived, prioritising their children.33 35 Parents often feared future relationships, worrying about children’s reactions, if a new partner would accept the role of the deceased within the family and the chance of losing someone again.33 34 Despite this, parents spoke of missing companionship and wanted their family to feel whole; some were open to new relationships.33–35 Parents reflected on the future they had lost, including loss of hopes and dreams, growing old together, being a 'traditional' family, and feeling sad that the children had lost a parent.34
Parenting alone was stressful,35 undertaking roles and responsibilities previously filled by the deceased. Some struggled with becoming the primary caregiver and disciplinarian, and providing emotional support.32–36 Some mothers noticed their sons assuming the father role, some stopped this, while others actively encouraged their son to be like their father.36 Fathers in one study spoke of newfound respect for their partners; having taken on their roles, they felt regret that they had not appreciated them more.35 Parents in several studies reported their children took on more responsibilities, helping around the house and caring for siblings.32 36
Parents' acceptability, availability and engagement with support
As with the children, parents received immediate support from family, friends, community, and their faith-based community, offering help and practical support.34 36 37 Initially, it was common for parents to struggle to accept support, even when needed and beneficial.32 33 35–37 Trying to show others they could cope, asking for help was a weakness, making some feel ashamed.32 34 However, fathers in one study were more accepting of support, acknowledging they could not manage without help.35
Parents in several studies found flexibility and understanding from their workplace and networks to be helpful, as these allowed them to be available for their children while still financially supporting their families.31–33 35 36
Some parents struggled finding appropriate professional bereavement support, reporting a mismatch between needs and help provided, with some professionals not equipped to deal with their needs or situation.33 37 Parents desired more professional help and information both prebereavement and postbereavement.30 33 In particular parents wanted professionals to be honest, deliver information which the family could handle, and show concern for the families individual needs.30 Some parents needed reassurance and would have liked a professional to check in on their family to ensure they were coping adaptively and provide information about their options, practical help and guidance on supporting the family.33 Some parents found others expected them to seek professional support, and if they chose not to, this was questioned.33 Parents had mixed experiences with school support, with some appreciating the tremendous support they received from teachers.31 35 36 Others found a lack of communication and understanding at school.31 School support was not mentioned by a study with widowed fathers in Denmark,33 despite those schools having bereavement response plans.22
Like the children, many parents experience dwindling support and a belief that they must cope with their loss alone and not burden others.31 33 36 37 Parents desired continued and sustained support from those within their networks and the professionals around them.31 33 36 37 It was important to have people around them who cared. However, some parents found that friends were unable or unwilling to provide the support they anticipated.34 People did not always know how to support them, causing offence rather than comfort.37
Faith helped some parents, receiving a positive response from the church community,34 who provided support, sympathy, advice, and practical and financial help.33 35 36 Some parents found praying helped bring them closer to God.34 However, not all parents found their faith helpful; some felt anger towards God, feeling let down and questioned if there was a God.34
Like the children, parents found those with a shared loss experience to be most supportive. Parents actively sought out bereaved peers and peer support groups who understood and could relate, sharing similar struggles and feelings, normalising their own experiences, and helping them adapt to their new lives and the challenges they faced.31 33–37 With these peers, they could be vulnerable; did not feel a burden and saw hope for the future, realising that grief was time-limited.33 36
Supporting the children
For many parents, their children brought meaning to their lives, a reason to carry on, and they focused on putting the children first.33 35–37 At times, this came at a cost, leaving parents with no time for themselves.35
Parents seldom asked children about their needs and used their judgements to handle situations, with some unaware of the support children received from teachers and siblings.30 36 Others misunderstood their child’s reactions and believed denial, disbelief and shock to be signs that the child did not understand and were not in mourning.36 Even when parents saw changes, they often felt ill-equipped to deal with changes and support their children.36
Many parents described difficulties breaking news of the death.36 37 Some felt guilty for not preparing the children for the death.31 Some were in denial; others felt the children’s lives would be affected soon enough, so why do that sooner.31 Those who talked to their children gave comfort and support and were open with their own emotions, finding this led to less conflict in the family.32 However, not all families could have open and honest communication, and some parents did not speak to their children or put effort into hiding their emotions to protect one another.36
Carrying on a relationship with the deceased was important to ensure children remembered them. Parents created memory boxes, and shared memories and stories of the deceased, bringing them into everyday life.32 34 36 Parents noticed that they chose to remember the good memories.32 However, not all parents were sure how or if they should continue a relationship with the deceased.34 When talking about the deceased, many waited for the children to initiate conversations and then seized the opportunity to ask how they were feeling.32 Some parents noticed that their children stopped talking or asking questions about the deceased when they saw it upset them.36 Others believed children avoided the conversations as it made them sad.32 Some forced themselves to talk and show emotions so their children knew it was OK to remember.36
Parents in many studies suppressed their emotions and grief to protect their children,33 36 37 which made them feel lonely.36 If parents were advised to be open with their children’s emotions, they saw the benefits for the family and how doing so could bring the family closer.36 Parents also noticed their children modified their behaviours and took on more responsibilities to protect them, and some were reliant on their children’s support.32 36 Parents in one study noticed their children worried for them, and for some, a role reversal could be seen.36 Children were worried about losing the surviving parent, which sometimes led to 'clingy' behaviour, worry, anxiety and distress.36
Discussion
This review is the first (to the best of our knowledge) to synthesise published studies on the support experiences of parentally bereaved children and surviving parents, highlighting the limited research available. The synthesis provides good insight into what is known about experiences and perspectives on support. The findings show that experience can vary according to cultural and country context.
This review highlights many benefits for families of open and honest communication, no matter how difficult that may be. Parents often avoid communication to protect their children because of fears and anxieties about how to talk about death. Avoidance techniques and beliefs that children are too young to understand death lead to limited, complex and variable exposure of children to death.38 A seminal study on coping behaviours39 describes this as 'protective buffering', which involves withholding information from others in order to protect them from distress. Protective buffering is widely used as a coping strategy among people with chronic illness40 41 and often associated with increased psychological distress for the protector and protected.39 Adults are often gatekeepers of information.42 Although well intentioned, a desire to protect children from death can result in unhelpful language, euphemisms or delays in preparing children for, or informing children of, parental deaths; this avoidance can create further problems for children.42 Differences were seen in how children continued relationships with the deceased; many talked about them and shared memories they had with their surviving parent.23–25 29–32 However, children from Taiwan hid their continued relationships with their deceased parent to protect their surviving parent.23 This culture prohibits talk around death. Death at a younger age is seen as taboo, and symbolically widowed mothers may be regarded as failures.43 Some parents thought their children avoided talking about the deceased because it was difficult or sad, so waited for the children to initiate conversations.32 Children verified they avoided these conversations as they did not know how to initiate them or feared causing upset.23 25 30 Reciprocal protection was seen throughout the review, with children and parents acting in ways to protect each other and those around them.
Despite this, evidence suggests that caregivers underestimate children’s ability to understand.44 An awareness and understanding of death can reduce fear or confusion around death and improve communication with children,45 who recognise the importance of talking about their loss,24 28 31 32 but do not know how to talk about it or feel they require permission to discuss death.31 32 Not talking about it affects how children cope with death, leading to difficulty regulating their emotions and a lack of skills to cope with death effectively.46 In addition, lack of open and honest communication leads to misunderstandings, with some children blaming themselves for the death.29 This lack of communication affects children into adulthood, affecting trust, relationships, self-esteem, the ability to express emotions and feelings of self-worth, loneliness and isolation.47 Children need an environment where they feel safe to ask questions about death and show their emotions,46 allowing children and parents to experience their suffering and survival together.45 Parents may require specific support from health and social care professionals and those around them to create an environment to foster open communication.48 49
Parents must recognise that children have agency and need to be informed and involved in what is happening to them and their families to help them adjust and cope. Allowing children to be involved in death rituals allows children to acknowledge and accept the reality of the death, honour their deceased parent, and receive support and comfort from others.50 The evidence shows that children are not simply reactive but have agency as family members.51 Children’s desire for agency was seen when a parent has a terminal illness; however, parents often do not recognise this need and their child’s capabilities and fail to give them agency over matters affecting them.52 53
Some children experienced a taboo surrounding death,28 often further enforced by those around them, who refused to have open discussions.29 Death is a taboo subject, causing social awkwardness, creating uncomfortable social reactions or ambivalence which can prevent individuals from supporting a bereaved person for fear of causing harm or being unprepared.54–57 This lack of understanding and awareness surrounding death means the bereaved do not always get a supportive response. However, children do not want death to be taboo; they want to discuss death and are open and curious to learn more.42 Yet, both personally and socially, children cannot access information about death, with avoidance of death seen in both their family and school lives.42 This highlights the benefits of normalising death conversations with children.42 Children desire information and opportunities to discuss death, including advice on how to grieve adaptively and receive timely communication about the death.46
Children found that peers often struggle to understand; unless they had similar experiences, they did not know how to behave or react, leaving children feeling isolated. The stigma surrounding parental death exists6 with social comparison, teasing or taunting by peers, highlighting a lack of understanding.58 This stigma may cause children to hide themselves and how they feel, not talking about it or withdrawing from social circles as an avoidance method.29 Some children believed their loss was too much for their peers to handle, causing further isolation, which parents added to by avoiding or waiting for the children to initiate conversations. Lower bereavement morbidity is seen when emotions are addressed and acknowledged within a family.59 Avoidance can be an adaptive response to loss and is a common reaction associated with anxiety and fear.59 However, reliance on avoidance as a coping strategy can contribute to complicated grief and poor long-term adjustment.59 60
Hiding and suppressing emotions and avoiding bereavement interactions were forms of coping and reciprocal protection which could be accounted for with Goffman’s theory of dramaturgy which likens social interaction to a theoretical performance.61 Presentation of self is a performance used to create an impression to provoke the desired response—consisting of the front stage, visible to the audience and backstage, which is not visible, allowing a safe place for people to vent feelings.61 Participants in this review often displayed front stage and backstage performances by avoiding bereavement interactions and suppressing emotions to prevent themselves or others from becoming upset, protecting others, and for children to prevent them from being perceived as different. Worryingly for some children, their parents and peers only saw their front stage performance, meaning backstage performances were enacted entirely alone. Supporting previous research, finding children had not spoken to anyone about their feelings following their parental loss,62 63 children feared the reaction of family members, finding it too difficult to talk or not knowing where to get help.62 63 Society influences grief reactions by implying that intense sadness should not be seen publicly.64 For many children, this was their first experience of death, and they would look to their parents to learn how to mourn; where parents hid their grief or suppressed emotions, their children could learn this is how they should mourn.65 This review supports recent recommendations to tackle the taboos surrounding death and dying and a greater need for a public health approach that encourages conversations surrounding dying, death and bereavement,66 67 coupled with a better understanding and response to the needs of the bereaved from their social networks and communities.1
Parents cope by committing to their children, putting their children’s needs first.33 35–37 Child-centred parenting has been shown to help children adapt better to their loss.68 Furthermore, having a purpose when bereaved has been shown to improve life satisfaction, provide a solid reason to live, increase social support and lessen the impact of loss.69 Parents found themselves in a challenging situation and often lacked advice or support to cope. Becoming a single parent through bereavement and taking on the other parent’s role can make parents question their parenting abilities, especially parenting a grieving child.70
Children and parents can struggle to accept support.23 27 32 35–37 Some parents experienced difficulties finding support appropriate to their family needs.30 33 36 37 Children were unsure who could support them or misinterpreted the supportive gestures they received.23 27 Healthcare professionals, although well placed to signpost families to appropriate support, are often unaware of available and appropriate support. Some families felt an expectation to seek professional support even though they felt it was unnecessary.33 There is a belief by some that professional support is essential, however, evidence suggests most bereaved people are well supported by their existing networks.11 This review supports the evidence that most families are initially well supported by their networks, but highlights a need for ongoing and sustained support.
Support quickly dwindled, with an unwritten 'timeline for grief' imposed by those around them.28 34 36 37 Others move on quickly, with an expectation that the bereaved should too, highlighting a lack of understanding about how grief affects individuals. Sustained support was appreciated, but few experienced this.31 33 36 37 This supports previous research findings that bereaved children wanted more sustained support.63 Some parents found those they expected would have given them good support did not,34 37 possibly through fear of not knowing what to say. Insecurity and fear have been described as factors that prevent social networks from providing support.71 Social networks of the bereaved may need advice and guidance on how to provide support.
Both children and parents experience similar challenges and changes following their loss, with a gap in the family that needs filling by changing roles and relationships.72 In line with family systems theory, how families behave and function are interdependent, meaning a change in one family member’s functioning will lead to changes in the other.73
Children and parents show examples of the Dual Process Model of coping with their bereavement.74 They adapted coping strategies and processes in their everyday lives, which oscillated between loss-orientated activities and restoration-orientated activities.74 However, despite the similarities in experience, there was little evidence to suggest children and parents were aware of or spoke of each other’s shared challenges. Instead, they managed their experiences alone, contributing to their feelings of isolation and, at times, suffering in silence. Sharing their experiences could open an avenue of support from each other in which they can both relate and feel less isolated in their experience.
Strengths and limitations
This is the first review (to the best of our knowledge) focusing on children and surviving parents' support experiences following parental death. A strength of the review is the combination of perspectives from both parents and children, especially the synthesis of fathers' perspectives, adding to the limited literature surrounding widowed men.
Not all included studies reported on the parental presence during the interview, which could either help or hinder children’s voices from being heard by influencing what and how things are discussed.75–77 Most studies recruited via bereavement support groups and services; therefore, participants may have received formal support. Included studies are also limited to two-parent families and do not consider blended families' experiences. The children included in the review were predominantly adolescents; therefore, these findings are not necessarily transferable to all parentally bereaved children.
Recommendations for research
This review highlights the lack of research in this field and the importance of involving children in such research. Further research needs to explore: families' differing relationships and perspectives of support and how they can support one another; support provided by existing networks; what a supportive response is; and the benefits of sustained support. Research needs to examine the experiences of blended and lone families and families who have not accessed formal support to understand how they cope and why they have not received formal support.
Conclusion
This review explored support experiences for children and parents following parental death. Open and honest communication and involving children are central to improving how families cope and adapt to life following parental death. A lack of support often resulted from a death 'taboo' within society, meaning some of those around a bereaved family did not understand or know how to respond to their needs. Parents are anxious to engage with open communication; however, death is more familiar to children than often expected. If parents were supported to realise the benefits of sharing their grief and engaging in open communication with their children, this would lead them to offer each other better support. Findings add to the discourse that childhood bereavement is a public health issue. As such, society, professionals and communities need to understand better and respond to the needs of bereaved families.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JasonWBoland
Contributors AW, JWB and SG developed the search strategy for the review. AW, SG, BP-S and OB reviewed search output. AW and SG contributed to the quality assessment of papers and data extraction. AW, BP-S, SP, BW, FM and JWB contributed to the thematic synthesis. AW prepared the manuscript, with support from JWB and FM, all authors read and agreed to the published version of the manuscript. AW is responsible for the overall content as the guarantor.
Funding This work was funded by Yorkshire Cancer Research as part of the TRANSFORM programme (award reference number HEND405PhD). FM is a National Institute for Health and Care Research (NIHR) Senior Investigator. The views expressed in this article are those of the author(s) and not necessarily those of the NIHR, or the Department of Health and Social Care. SG is funded by Yorkshire Cancer Research as part of the TRANSFORM programme. OB is funded by Yorkshire Cancer Research as part of the TRANSFROM programme (award reference number HEND405SPT).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.