Article Text

Abstract
Objectives To describe multinational prescribing practices by palliative care services for symptom management in patients dying with COVID-19 and the perceived effectiveness of medicines.
Methods We surveyed specialist palliative care services, contacted via relevant organisations between April and July 2020. Descriptive statistics for categorical variables were expressed as counts and percentages. Content analysis explored free text responses about symptom management in COVID-19. Medicines were classified using British National Formulary categories. Perceptions on effectiveness of medicines were grouped into five categories; effective, some, limited or unclear effectiveness, no effect.
Results 458 services responded; 277 UK, 85 rest of Europe, 95 rest of the world, 1 missing country. 358 services had managed patients with confirmed or suspected COVID-19. 289 services had protocols for symptom management in COVID-19. Services tended to prescribe medicines for symptom control comparable to medicines used in people without COVID-19; mainly opioids and benzodiazepines for breathlessness, benzodiazepines and antipsychotics for agitation, opioids and cough linctus for cough, paracetamol and non-steroidal anti-inflammatory drugs for fever, and opioids and paracetamol for pain. Medicines were considered to be mostly effective but varied by patient’s condition, route of administration and dose.
Conclusions Services were largely consistent in prescribing for symptom management in people dying with COVID-19. Medicines used prior to COVID-19 were mostly considered effective in controlling common symptoms.
- COVID-19
- Hospice care
- Symptoms and symptom management
- End of life care
- Terminal care
Data availability statement
Data are available on reasonable request. Applications for use of the survey data can be made for up to 10 years, and will be considered on a case-by-case basis on receipt of a methodological sound proposal to achieve aims in line with the original protocol. The study protocol is available on request. All requests for data access should be addressed to the chief investigator via the details on the CovPall website (https://www.kcl.ac.uk/cicelysaunders/research/evaluating/covpall-study and palliativecare@kcl.ac.uk) and will be reviewed by the Study Steering Group.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Multinational data on medicines prescribed for symptom control in people dying with COVID-19 are lacking.
WHAT THIS STUDY ADDS
Multinational specialist palliative care services prescribed similar medicines to those used in other conditions for people dying with COVID-19.
Medicines were perceived to be effective in symptom management.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Medicines used for symptom control in non-COVID-19 conditions were considered effective in COVID-19.
Introduction
Specialist palliative care services have been critical in managing people dying with COVID-19 and ensuring symptom control towards the end of life.1 2 Frequent symptoms in severe COVID-19 include breathlessness and agitation.3 4 Cough, fever, fatigue, pain and respiratory secretions are also common.3 5
A recent rapid review on the pharmacological strategies used for symptom management in patients dying of COVID-19 found seven studies (n=493 patients), and concluded that modest doses of morphine and midazolam are required for symptom control.6 There is very limited evidence on international practice and service-level perspectives regarding pharmacological management of symptoms and the perceived effectiveness of medicines in patients dying with COVID-19.
Opioids and benzodiazepines are recommended in guidelines for breathlessness in severe COVID-19.2 7 Opioids are generally used in palliative care and are the first line treatment for refractory breathlessness.8 9 Benzodiazepines have been recommended in patients dying from severe COVID-19, but there is mixed evidence in other advanced illnesses on benefits and harms,10 and no evidence in COVID-19.
Before the COVID-19 pandemic, benzodiazepine prescribing had been reported to differ between the UK and European countries. Huerta et al11 reported higher benzodiazepine prescribing in UK and Spanish electronic healthcare databases, but lower prescribing in Dutch, German and Danish databases. Possible reasons for differences included variation in help-seeking habits of patients and the diseases for which benzodiazepines are indicated by country as well as prescribing habits. Despite the adverse effects associated with benzodiazepines, the majority of hospice clinicians view them as beneficial treatments for breathlessness and agitation.12
While pain, agitation, fever and cough are severe symptoms in COVID-19,3 5 there have been limited information about their clinical management.4 Given the lack of clarity on benzodiazepine benefit for breathlessness, concerns around safety and variation in its prescribing by country,11 and the dearth of information around prescribing for pain, agitation, fever and cough in COVID-19, it is important to understand what is being prescribed for symptom control in patients dying with COVID-19 and whether prescribed medicines are considered to be effective by specialist palliative care services. We therefore aimed to describe multinational prescribing practices of specialist palliative care services for symptom management in patients dying with COVID-19 and the perceived effectiveness of medicines.
Methods
Study design and participants
This paper reports results from the CovPall study that aimed to understand the multinational specialist palliative care response to COVID-19.1 A survey was a fundamental part of the first work package for this study. The survey opened on 23 April 2020 and closed on 31 July 2020.
Services providing hospice and specialist palliative care were eligible for participation and were recruited through palliative care and hospice organisations (Hospice UK, Marie Curie, Sue Ryder, Together for Short Lives, European Association of Palliative Care, palliativedrugs.com and the www.pos-pal.org network). They were provided with a link to the online survey, and service leads (medical or nurse directors/clinicians) or their selected nominees were invited to complete the survey. The CovPall protocol is registered (ISRCTN16561225) and these results are reported according to Strengthening the Reporting of Observational Studies in Epidemiology,13 CHERRIES14 and MORECARE15 statements.
Survey and data collection
The questionnaire was developed building on an earlier survey of Italian hospices and has been reported in the main CovPall paper.1 The Research Electronic Data Capture16 was used to build a secure, web-based survey which had 72 closed text and 94 free text responses.
This paper focuses on prescribing practices for symptom management and how effective services found prescribed medicines (eg, time to give relief and how well it worked) (see online supplemental appendix 1). For the quantitative data items, we analysed the following variables by world region: protocols and protocol sources for symptom management, prescribing for breathlessness, agitation, cough, fever and pain. From the free text comments, we analysed 10 open-ended questions (see online supplemental appendix 1). Open free text comments were summarised and explored to understand how service leads (or their nominees) perceived the effectiveness of medicines prescribed for symptom management in patients dying with COVID-19.
Supplemental material
Data analysis
For the quantitative data items, descriptive statistics for categorical variables were expressed as counts and percentages. We used contingency tables, χ2 tests and Fisher’s exact test to explore relationships between variables (using SPSS V.26). Free text comments describing the types of medicines prescribed were summarised in Excel using content analysis; the British National Formulary17 categories were used. Responses to questions on the effectiveness of prescribed medicines were categorised into ‘effective’, ‘some effectiveness’, ‘limited effectiveness’, ‘unclear effectiveness’ and ‘no effect’ based on comments provided by respondents. For example, if medicines were described as generally effective within 10–20 min by respondents, this was classified as ‘effective’. Time to effect was also grouped based on respondents’ comments into effect within 30 min, effect over 31 min and varied effect.
Results
In the original CovPall survey,1 489 questionnaires were commenced and 477 completed (completion rate 97.5%). Nineteen were invalid because they were duplicates, triplicates or were from researchers without a palliative care service, leaving 458 valid responses: 277 UK, 85 rest of Europe, 95 rest of the world, 1 missing country.
In total, 358 services had managed patients with confirmed or suspected COVID-19: 248 UK, 60 rest of Europe, 49 rest of the world and 1 missing country. Of these, services were usually publicly (165, 47%), or charity managed (150, 42.7%); 15 (4.3%) were privately managed, 21 (6%) other; 7 missing. In total, 203 services provided inpatient palliative care units, 204 home care teams, 182 hospital palliative care teams and 94 home nursing teams. Over half of services (56.4%) provided care in more than one setting.
Two hundred and eighty-nine services had protocols for symptom management in COVID-19. Protocols for symptom management were available for 216 of 231 (93.5%) UK services, 44 of 52 (84.6%) services in the rest of Europe and 29 of 41 (70.7%) services in the rest of the world. Of 289 services with symptom management protocols, 238 (82.4%) services reported using locally developed guidelines: 181 UK, 34 rest of Europe and 23 rest of the world. Locally developed guidelines were used by 181 of 216 (83.8%) UK services, 34 of 44 (77.3%) services in the rest of Europe and 23 of 29 (79.3%) services in the rest of the world.
Prescribing for symptoms
Breathlessness
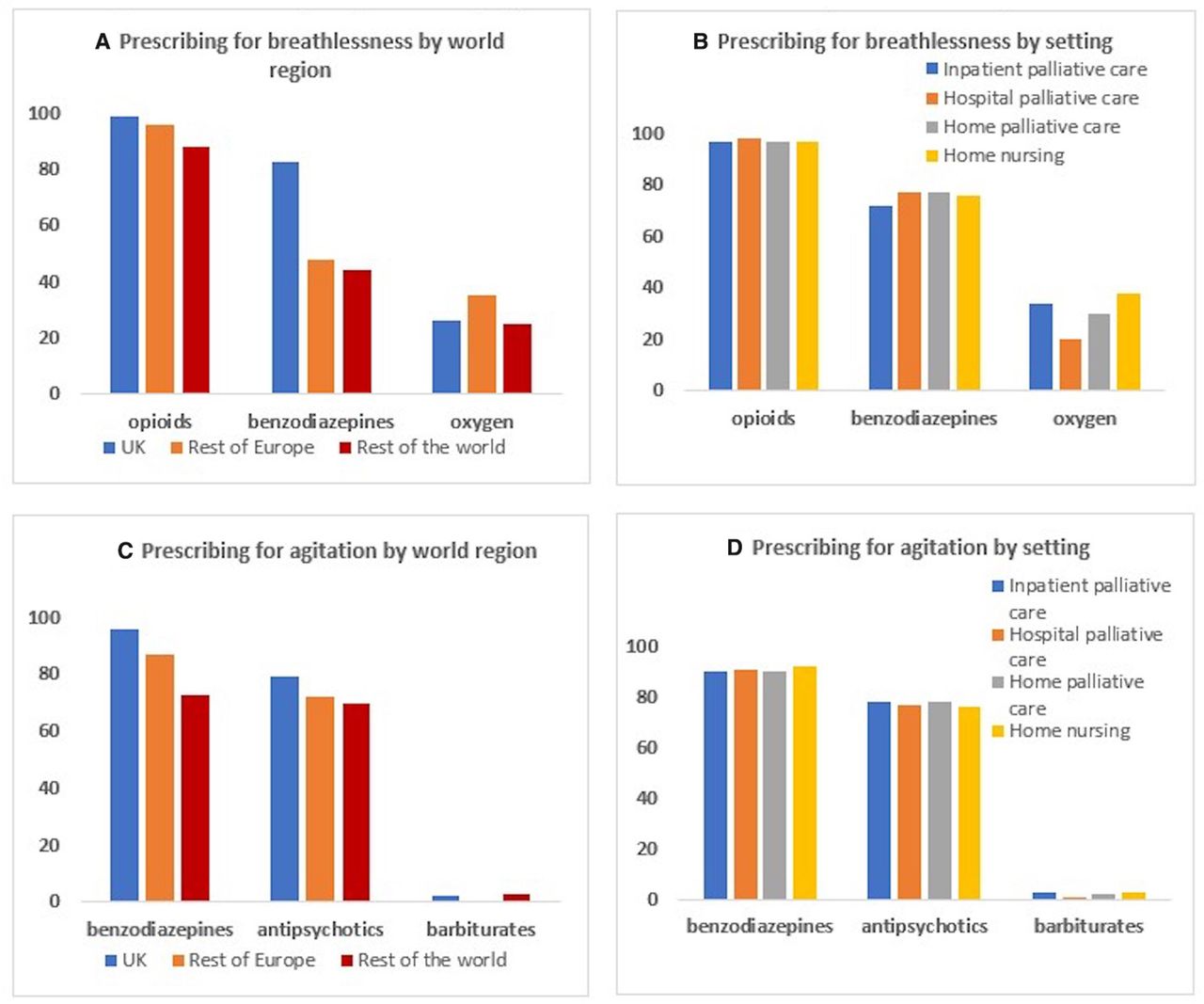
The three most common prescribed medicines for breathlessness were opioids (n=273 of 282 (96.8%) services), benzodiazepines (n=205 of 282 (72.7%) services) and oxygen (n=76 of 282 (27%) services) (table 1, online supplemental appendix 2a).
Characteristics of palliative care and hospice services that managed patients with suspected or confirmed COVID-19 by region
The level of opioid prescribing by services in different world regions and palliative care settings were similar (figure 1A and B, online supplemental appendix 2a, 2b). Morphine was the most prescribed opioid, representing 172 (54.1%) of the 318 prescribed opioids. Others included oxycodone (n=26 (8.2%)), fentanyl (n=9 (2.8%)), hydromorphone (n=4 (1.3%)), diamorphine (n=3 (0.9%)), alfentanil (n=3 (0.9%)), buprenorphine (n=3 (0.9%)) and sufentanil (n=1 (0.3%)) (online supplemental appendix 2c). Some services reported prescribing opioids but did not state the type of opioid (n=97 (30.5%)).
{kind=link}
Percentage of prescribing by services in different settings and world regions.
Prescribing of benzodiazepines for breathlessness was significantly higher in the UK (83%) than the rest of Europe (48%) and the world (44%) (figure 1A, online supplemental appendix 2a) (χ2=38.42, p=<0.001). Among benzodiazepines, midazolam (n=126 (48.6%) of 259) was the most prescribed. Others included lorazepam (n=58 (22.4%)), diazepam (n=3 (1.2%)), oxazepam (n=2 (0.8%)), clonazepam (n=1 (0.4%)). The type of benzodiazepines prescribed was not stated in 69 (26.6%) cases (online supplemental appendix 2c).
Palliative care services that prescribed oxygen were less likely to have hospital palliative care teams (χ2=9.16, p=0.002).
Fifty seven services indicated how quickly medicines worked, with 43 (75.4%) responding that they worked within 30 min and 13 (22.8%) over 31 min (table 1).
All respondents on the perceived effectiveness of these medicines considered them to be either effective or as having some effect. Perceived effectiveness depended on the patient’s condition and route of drug administration (online supplemental appendix 2d).
In context of COVID-19 we found opioids to be very effective in relieving distressing dyspnoea, particularly when given SC if severe symptoms. In some instances with severe symptoms multiple SC doses were needed to gain symptom control. MR Morphine (MST, Zomorph) preparations were helpful for patients to better tolerate CPAP/Venturi masks etc. Addition of benzodiazepines was helpful where anxiety component. In most instances good relief within 30mins—1hr if given Midazolam SC or Lorazepam SL (hospital palliative care team, UK).
Although medicines tended to be effective, this was challenging to predict with an acknowledgement that patients sometimes required high doses.
Benzos and opioids tend to work in 10-20 minutes. Most people need small doses, but some need bigger doses (inpatient palliative care unit/hospital palliative care team/home palliative care team, UK).
Further, services reported reluctance to prescribe opioids.
…Not quite effective in some cases, it’s difficult due to some senior physicians afraid of opioids. (hospital palliative care team/home palliative care team, rest of the world).
Agitation
The most common prescribed medicines for agitation were benzodiazepines (n=255 of 277 (92.1%) services) and antipsychotics (n=213 of 277 (76.9%) services) (figure 1c; online supplemental appendix 3a). Prescribing of benzodiazepines was higher in the UK (96%) than the rest of Europe (87%) and the world (73.3%) (Fisher’s exact test=16.82, p≤0.001), but did not differ by setting (figure 1D; online supplemental appendix 3b).
Midazolam was the most prescribed benzodiazepine for agitation, making up 215 of 317 (67.8%) prescribed benzodiazepines. Other benzodiazepines prescribed included lorazepam (n=52 (16.4%)), diazepam (n=7 (2.2%)), clonazepam (n=2 (0.6%)), oxazepam (n=3 (0.9%)), alprazolam (n=1 (0.3%)) and lormetazepam (n=1 (0.3%)) (online supplemental appendix 3c). Some services did not state the type of benzodiazepine prescribed (n=36 (11.4%)).
Among antipsychotics, levomepromazine was most commonly prescribed for agitation: 157 of 315 (49.8%) prescribed antipsychotics. Haloperidol (n=132 (41.9%)), olanzapine (n=4 (1.3%)), chlorpromazine (n=3 (1%)), quetiapine (n=3 (1%)), risperidone (n=2 (0.6%)), cyamemazine (n=1 (0.3%)), droperidol (n=1 (0.3%)) and promazine (n=1 (0.3%)) were also prescribed (online supplemental appendix 3c). In 11 (3.5%) cases, the type of antipsychotic prescribed was not stated.
Out of 234, 189 (80.3%) respondents considered prescribed medicines to be effective, while 42 (17.9%) and 4 (1.7%) reported some effect and limited effect respectively (online supplemental appendix 3d). Forty-two services indicated how quickly medicines worked, and 28 (66.7%) responded that they worked within 30 min (table 1). Medicines tended to be effective depending on symptom severity, type of medicine, route of administration and dosage. One service highlighted that
Midazolam SC effective within 30mins-2hrs. If severe symptoms often needed to give multiple doses before symptom controlled. Levomepromazine was found to be more effective if there was a delirium component to agitation (hospital palliative care team, UK).
Another service highlighted limited effectiveness
…no(t) so well. Especially for ventilated patients with agitation/delirium (inpatient palliative care team, rest of Europe).
Cough
The three most prescribed medicines for cough were opioids (n=238 of 251 (94.8%) services), cough linctus (n=76 of 251 (30.3%) services) and nebulised saline (n=10 of 251 (4%) services) (table 1; online supplemental appendix 4a).
Opioids prescribed were morphine, representing 123 of 299 (41.1%) prescribed opioids; codeine (n=75 (25.1%)); methadone (n=7 (2.3%)); oxycodone (n=6 (2%)); paracodeine (n=4 (1.3%); dihydrocodeine (n=3 (1%)); hydrocodone (n=1 (0.3%)); fentanyl (n=1 (0.3%)); sufentanil (n=1 (0.3%)); hydromorphone (n=1 (0.3%)); diamorphine (n=1 (0.3%)) (online supplemental appendix 4b). In 79 (26%) cases, the type of opioid prescribed was not stated.
Across settings, opioids were prescribed by 89% to 96% of services; cough linctus by 25% to 50% of services; nebulised saline by 2%–11% of services (online supplemental appendix 4c). Cough linctus prescribing was higher in the UK (41%) than Europe (5%) and the rest of the world (3%) (χ2=31.85, p<0.001); opioid prescribing differed across world regions (83%–98%) (online supplemental appendix 4a) (Fisher’s exact test=6.92, p=0.026).
Twenty-one services indicated how quickly medicines worked; 13 (61.9%) stated that they worked within 30 min and 7 (33.3%) highlighted effect over 31 min (table 1). The remaining service indicated that the onset of effect varied.
Out of 177, 151 (85.3%) respondents considered prescribed medicines to be effective or somewhat effective, while the remaining reported limited (13.6%) or unclear effects (1.1%) (online supplemental appendix 4d).
not that good, though not a common Sx (symptoms) in the elderly (home palliative care team, UK).
There was an indication that cough was sometimes challenging to treat.
in combination with other medications to support end of life care then I would say that cough can be reduced within a short period of time. Difficult to achieve no cough (hospital palliative care team, UK).
Fever
The most prescribed medicines for fever were paracetamol (n=267 of 272 (98.2%) services), non-steroidal anti-inflammatory drugs (NSAIDs) (n=46 of 272 (16.9%) services) and metamizole (n=15 of 272 (5.5%) services) (table 1). NSAIDs prescribed were ibuprofen, representing 11 of 48 (22.9%) prescribed NSAIDs, diclofenac (n=7 (14.6%)) and ketorolac (n=1 (2.1%)). In 29 (60.4%) cases, the type of NSAID prescribed was not stated (online supplemental appendix 5a).
Prescribing for fever tended to be similar across world regions except for metamizole. Metamizole was not prescribed in the UK, while 32% and 3.4% of services in the rest of Europe and the world respectively prescribed it (online supplemental appendix 5b). Prescribing for fever was similar across settings (online supplemental appendix 5c).
Thirty-seven services indicated how quickly medicines worked; 17 (45.9%) responded that they worked within 30 min and 19 (51.4%) within over 31 min. One (2.7%) service said this varied.
Out of f 201, 188 (93.5%) respondents on the effectiveness of these medicines considered them to be effective or to have some effect, while the remaining reported limited effect (10, 5%), no effect (1, 0.5%) or unclear effect (2, 1%) (online supplemental appendix 5d). There was an indication of variation in recommendations across countries regarding what to prescribe for fever.
[paracetamol] quite effective but NSAIDS might have been more effective - in the French COVID context, they were not recommended because allegedly causing more severe cases (inpatient palliative care unit/hospital palliative care team, rest of Europe).
Services also described limited effect.
Temperatures in COVID-19 +ve patients have not always settled with paracetamol and needed NSAID 2nd line (inpatient palliative care unit/home palliative care team/home nursing services, UK).
Pain
Opioids (n=244 of 247 (98.8%) services), paracetamol (n=74 of 247 (30%) services) and neuropathic agents (n=33 of 247 (13.4%) services) were mostly prescribed for pain (table 1). Opioids prescribed included morphine, representing 119 of 364 (32.7%) prescribed opioids, oxycodone (n=50 (13.7%)), fentanyl (n=22 (6%)), alfentanil (n=12 (3.3%)), methadone (n=12 (3.3%)), hydromorphone (n=11 (3%)), buprenorphine (n=8 (2.2%)), codeine (n=3 (0.8%)), diamorphine (n=3 (0.8%)), tramadol (n=2 (0.6%)), sufentanil (n=2 (0.6%)), hydrocodone (n=1 (0.3%)) and pethidine (n=1 (0.3%)) (online supplemental appendix 6a). In 118 (32.4%) cases, the type of opioids was not described.
Neuropathic agents prescribed for pain included gabapentin (n=16 (40%)), pregabalin (n=8 (20%)) and anticonvulsants (n=2 (5%)) (online supplemental appendix 6a). The type of neuropathic agent prescribed was not stated in 14 (35%) cases. Prescribing of neuropathic agents was higher in the rest of the world (20%) compared with the UK (14%) and the rest of the Europe (5%). Other medicines in which there was variation in prescribing across world regions include antidepressants, anaesthetics, NSAIDs and other non-opioid analgesics (online supplemental appendix 6b). Prescribing across settings was broadly similar (online supplemental appendix 6c).
Thirty services indicated how quickly medicines worked; 17 (56.7%) responded that they worked within 30 min and 11 (36.7%) within over 31 min. Two (6.7%) services responded that how quickly medicines worked varied.
Out of 199, 198 (99.5%) respondents considered the medicines to be effective or somewhat effective, while the remaining service reported unclear effects (0.5%). Medicines tended to be effective depending on the route of administration, drug, dose and type of pain (online supplemental appendix 6d):
[Opioids] mostly well. Depends on dose and responsiveness of pain to opioids. Sometimes an NSAID is just better (inpatient hospice palliative care team, UK).
Discussion
We report a multinational service-level perspective on prescribing to manage the symptoms of patients dying with COVID-19. With the exception of benzodiazepines prescribed for breathlessness and agitation, services within world regions tended to prescribe similar medicines for symptom control. This included mainly opioids and benzodiazepines for breathlessness, benzodiazepines and antipsychotics for agitation, opioids and cough linctus for cough, paracetamol and NSAIDs for fever, and opioids and paracetamol for pain. Medicines were considered to be effective as 45.9%–75.4% of prescribed medicines were reported to work within 30 min.
Evidence suggests that breathlessness and agitation are common in severe COVID-19.3 18 A recent review6 suggests these symptoms in terminal COVID-19 can be alleviated with modest opioid and benzodiazepine doses (eg, 15 mg morphine CSCI and 10 mg midazolam CSCI). This is similar to our findings and is in line with national and international guidelines.2 7 19 It is however not clear when benzodiazepines are being used for agitation related to breathlessness or agitation from other causes. Prior evidence from a Cochrane review showed no evidence of effect when benzodiazepines are used for breathlessness in other advanced diseases.10 Medicines prescribed were typical for similar symptoms in people without COVID-19, implying that services consider them to be effective. However, it might also represent a dependence on clinical guideline recommendations prevalent at the time, with limited evidence and understanding of the disease.20
We found low levels of prescribing of oxygen and corticosteroids. This may be because this survey was carried out early in the pandemic when little was known about their benefits. In patients with COVID-19, there is scant evidence to support oxygen use in the absence of hypoxaemia. Also, patients may have been in the dying phase and prevented from dying with a mask on which could worsen agitation. There is evidence that corticosteroids are beneficial in reducing the risk of breathlessness, the cytokine storm and mortality in COVID-19 patients who require oxygen and ventilation21 22; the need for mechanical ventilation is also reduced.
Some of the variation by world regions may be due to medicines availability and regulations around prescribing. For instance, metamizole was prescribed for fever in the rest of Europe and the world, but not in the UK. Metamizole is banned in the UK due to the associated risk of agranulocytosis.23 Furthermore, services sometimes reported the use of medicines that are outside guideline recommendations. For instance, prescribing of antipsychotics for breathlessness. However, we did not explore the reasons for such prescribing in this study.
Over 80% of services with symptom management protocols used locally developed guidelines. While it is unclear whether the locally developed guidelines are adaptations of national guidelines, it does imply duplication of effort by services. For an effective and coordinated response, processes are needed for better translation of learnings from the pandemic into policies and guidelines that are easily accessible and usable.
Limitations
This study is limited by its cross-sectional design. Given that services sometimes did not state the type of medicine they prescribed in a particular class, we could not make comparisons between different types of medicines (eg, comparing use of different types of benzodiazepines). Assessment of treatment benefit by service leads was a subjective impression of effectiveness, including reports from team members. These responses were then categorised into different levels of effectiveness by our team.
As randomised controlled trials may be impractical, further research, involving observational studies are needed to understand from patient level data whether these medicines, including doses, duration and route, are effective in improving patient outcomes.
Furthermore, there may be non-response, sample and other biases. We cannot tell if the prescribing practices of services that did not respond are different to those of respondents. The survey was distributed through organisations that were mainly based in the UK and Europe, and most respondents were UK services. The survey was offered only in English and some countries were not represented. When we carried out the survey, countries were at varying stages in the pandemic, which may have affected responses. These limit the interpretation of our international comparisons.
Conclusion
Overall, similar medicines to those used in symptom management in other conditions were prescribed for people dying with COVID-19. Our data suggest that medicines used in non-COVID-19 conditions appear to be effective for symptom control. Prescribing was largely consistent across countries and palliative care settings. Further research is needed to clarify which medicines are most effective in improving patient outcomes.
Data availability statement
Data are available on reasonable request. Applications for use of the survey data can be made for up to 10 years, and will be considered on a case-by-case basis on receipt of a methodological sound proposal to achieve aims in line with the original protocol. The study protocol is available on request. All requests for data access should be addressed to the chief investigator via the details on the CovPall website (https://www.kcl.ac.uk/cicelysaunders/research/evaluating/covpall-study and palliativecare@kcl.ac.uk) and will be reviewed by the Study Steering Group.
Ethics statements
Patient consent for publication
Ethics approval
The survey received ethical approval from King’s College London Research Ethics committee (LRS-19/20-18541). Completion of the survey by participants indicated consent.
Acknowledgments
We thank all collaborators and advisors. We thank all participants, partners, PPI members and our Study Steering Group. We gratefully acknowledge technical assistance from the Precision Health Informatics Data Lab group (https://phidatalab.org) at National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London for the use of REDCap for data capture.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @SBajwah, @kesleeman, @cewalshe, @nancypreston16, @MevHocaoglu
Contributors IJH is the grant holder and chief investigator; KES, MM, FM, CW, NP, LF, SB, MH and AOO are coapplicants for funding. IJH and CW with critical input from all authors wrote the protocol for the CovPall study. MH, AOO and RLC coordinated data collection and liaised with centres, with input from IJH. AOO analysed the data. All authors had access to all study data, discussed the interpretation of findings and take responsibility for data integrity and analysis. AOO drafted the manuscript. All authors contributed to the analysis plan and provided critical revision of the manuscript for important intellectual content. IJH is the guarantor.
Funding This study was part of CovPall, a multinational study. This research was primarily supported by Medical Research Council grant number MR/V012908/1. Additional support was from the National Institute for Health Research (NIHR), Applied Research Collaboration, South London, hosted at King’s College Hospital NHS Foundation Trust, and Cicely Saunders International (Registered Charity No. 1087195). IJH is a National Institute for Health Research (NIHR) Emeritus Senior Investigator and is supported by the NIHR Applied Research Collaboration (ARC) South London (SL) at King’s College Hospital National Health Service Foundation Trust. IJH leads the Palliative and End of Life Care theme of the NIHR ARC SL and co-leads the national theme in this. MM is funded by a National Institute for Health Research (NIHR) Career Development Fellowship (CDF-2017-10-009) and NIHR ARC SL. LF is funded by a NIHR Career Development Fellowship (award CDF-2018-11-ST2-002). KES is the Laing Galazka Chair in palliative care, funded by an endowment from Cicely Saunders International and Kirby Laing. RC is funded by Cicely Saunders International and Marie Curie. FM is an NIHR senior investigator. MH is supported by the NIHR ARC SL.
Disclaimer The views expressed in this article are those of the authors and not necessarily those of the NIHR, or the Department of Health and Social Care.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.