Article Text

Abstract
Objectives Febrile neutropenia (FN) commonly occurs during cancer chemotherapy. Prophylaxis with granulocyte colony-stimulating factors (G-CSFs) is known to reduce the severity and incidence of FN and infections in patients with cancer. Despite the proven efficacy, G-CSFs are not always prescribed as recommended. We performed a discrete-choice experiment (DCE) to determine what factors drive the physician preference for FN prophylaxis in patients with cancer undergoing chemotherapy.
Methods Attributes for the DCE were selected based on literature search and on expert focus group discussions and comprised pain at the injection site, presence of bone pain, associated fever/influenza syndrome, efficacy of prophylaxis, biosimilar availability, number of injections per chemotherapy cycle and cost. Oncologists, in a national database, were solicited to participate in an online DCE. The study collected the responses to the choice scenarios, the oncologist characteristics and their usual prescriptions of G-CSFs in the context of breast, lungs and gastrointestinal cancers.
Results Overall, the responses from 205 physicians were analysed. The physicians were mainly male (61%), with ≤20 years of experience (76%) and working only in public hospitals (73%). The physicians prescribe G-CSF primary prophylaxis for 32% of patients: filgrastim in 46% and pegfilgrastim in 54%. The choice of G-CSF for primary and secondary prophylaxis was driven by cost and number of injections. Biosimilars were well accepted.
Conclusion Cost and convenience of G-CSF drive the physician decision to prescribe or not G-CSF for primary and secondary FN prophylaxes. It is important that these results be incorporated in the optimisation of G-CSF prescription in the clinical setting.
- cancer
- hospital care
- supportive care
- symptoms and symptom management
Data availability statement
No data are available. PrefmeG.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What was already known?
Granulocyte colony-stimulating factors (G-CSFs) are not always prescribed as recommended.
In clinical practice, the use of G-CSFs is driven by various factors including the convenience and cost of G-CSFs, availability of biosimilars and the clinical evidence for the benefit of G-CSFs.
What are the new findings?
In France, the choice of G-CSF for primary and secondary prophylaxes was driven by cost and number of injections.
Biosimilar G-CSFs are well accepted by French physicians.
What is their significance?
Clinical: The factors that influence the choice of G-CSF will allow optimisation of G-CSF use in clinical practice and consequently improve febrile neutropenia management in patients with cancer.
Research: The acceptability of biosimilars in France and the lower costs associated with biosimilars may increase the use of G-CSFs as prophylaxis in routine practice.
Introduction
Febrile neutropenia (FN) occurs when severe neutropenia, with an absolute neutrophil count below 500/mm3, is associated with a fever higher than 38°C.1 2 A common cause of FN is cancer chemotherapy.1 Patients with chemotherapy-induced neutropenia are at high risk of developing life-threatening infections.1 In addition, FN causes treatment delays, dose reductions and even early termination of chemotherapy.3–6 These management modifications can negatively affect tumour response and other outcomes, including survival.7 Indeed, the risk of death for patients with FN is estimated to be about 10%.3 5 8 In cases of FN, patients are often hospitalised and administered intravenous broad-spectrum antibiotics.1 Also, FN induces significant burden.
In humans, granulocyte colony-stimulating factor (G-CSF) is a naturally occurring glycoprotein, a haematopoietic colony-stimulating factor that stimulates neutrophil precursors in the bone marrow to proliferate and differentiate, as well as activating mature neutrophils.6 9
In the early 1990s, the recombinant human G-CSF, filgrastim, was approved as primary prophylaxis for preventing FN, after it was shown to reduce the risk of FN and infections in patients with cancer treated with chemotherapies.6 A disadvantage of filgrastim is its relatively short half-life.10 Indeed filgrastim, a short-acting G-CSF, requires daily injections to stimulate neutrophil production and maturation. In 2002, pegfilgrastim, with a longer half-life than filgrastim, was approved in the European Union.6 10 Pegfilgrastim is more convenient since it only requires a single injection for each chemotherapy cycle to stimulate neutrophil production. However, pegfilgrastim has a significantly higher cost per injection compared with filgrastim.11 Overall, the efficacy of pegfilgrastim and filgrastim to reduce the incidence of FN and infections has been found to be comparable.12 13 However, in everyday clinical practice, filgrastim is frequently underdosed, resulting in a reduced effectiveness compared with pegfilgrastim.12 13 Since the approval of filgrastim and pegfilgrastim, numerous biosimilars have been developed and commercialised.4 14 15 Biosimilars, compared with reference biologics, have comparable efficacy but are cheaper and therefore more cost effective.12
The European Organisation for Research and Treatment of Cancer guidelines (2010) recommend primary prophylaxis with G-CSF in patients with cancer prescribed chemotherapies with a >20% risk of FN and in those prescribed chemotherapies with a risk between 10% and 20% if the patients have other FN risk factors.16
Nevertheless, in everyday clinical practice, G-CSF prescription is not always consistent with the guidelines. In fact, various studies have shown that G-CSFs tend to be overused in patients administered low-risk chemotherapies (risk of FN <10% or 10%–20%) and underused in those on high-risk regimens (risk of FN >20%).17–19 Indeed, the use of G-CSFs in clinical practice, as primary and secondary prophylaxes, is driven by various factors including the convenience and cost of G-CSFs, availability of biosimilars and the clinical evidence for the benefit of G-CSFs.14 A better understanding of the factors that influence the choice of G-CSF will allow optimisation of G-CSF use in clinical practice and consequently improve FN management in patients with cancer .
Our primary objective was to determine the physician preference for G-CSF, as primary prophylaxis, for patients with cancer initiating chemotherapy. The physician preference for G-CSF, as secondary prophylaxis, was also assessed. We also assessed whether physician characteristics (medical specialty, healthcare sector and type of healthcare institution) impacted the G-CSF preferences, for both primary and secondary prophylaxes.
Methods
Development of the discrete-choice experiment (DCE) content
A DCE was used to assess the characteristics/attributes associated with the physician’s preferred use of G-CSF.
Discrete-choice experiment
The DCE is a choice-based method that compares treatment options pairwise. The attributes chosen for the DCE, including G-CSF characteristics (efficacy, tolerance and injection frequency), were selected based on the literature and on discussion by an expert focus group. The following attributes were selected for the DCE: pain at the injection site, presence of bone pain, associated fever or influenza syndrome, efficacy of prophylaxis (risk of FN with prophylaxis), availability of biosimilar, number of planned G-CSF injections per chemotherapy cycle and cost of each G-CSF injection (included the associated nurse’s cost).
Construction of DCE questionnaire
The DCE questionnaire was composed of eight scenarios. Each scenario had two G-CSF treatment options, each with seven attributes. The eight scenarios with details concerning the attributes are shown in online supplemental table S1. In addition, the overall cost of the G-CSF options for a chemotherapy cycle was indicated, calculated from the number injections required per chemotherapy cycle and the cost per injection. The participating physician selected one of the two treatment options for each scenario in the primary and secondary prophylactic settings.
Supplemental material
Participants and data collection
This study was performed in physicians that use G-CSF prophylaxis (primary and secondary) during the treatment of patients with cancer with chemotherapy. Oncologists, throughout France, in both private and public healthcare institutions, were solicited to participate in this study.
Statistical analysis
The baseline characteristics of participants are described using descriptive statistics. Categorical data are reported as frequency with percentages. Continuous data are reported as mean with SD or as median with the associated range. The numbers of missing data are reported, when applicable.
The relative importance of each attribute for the choice of treatment, in the DCE experiment, was estimated using a mixed logit model combining fixed effects on treatment attributes and random effects on respondents. Random effects were necessary to estimate the impact of the treatment attributes on the participants’ choice independently of personal preference. The equation used to model the physician choices is shown in online supplemental figure S1. For the model, the choices for each attribute were given a numerical value between 0 and 3; for example, for the attribute risk of FN, low risk of FN was assigned 0 and moderate risk 1, and for the number of injections per cycle, one injection was assigned 1, two injections were assigned 5, and three injections were assigned 10. The complete list is shown in online supplemental table S2.
Supplemental material
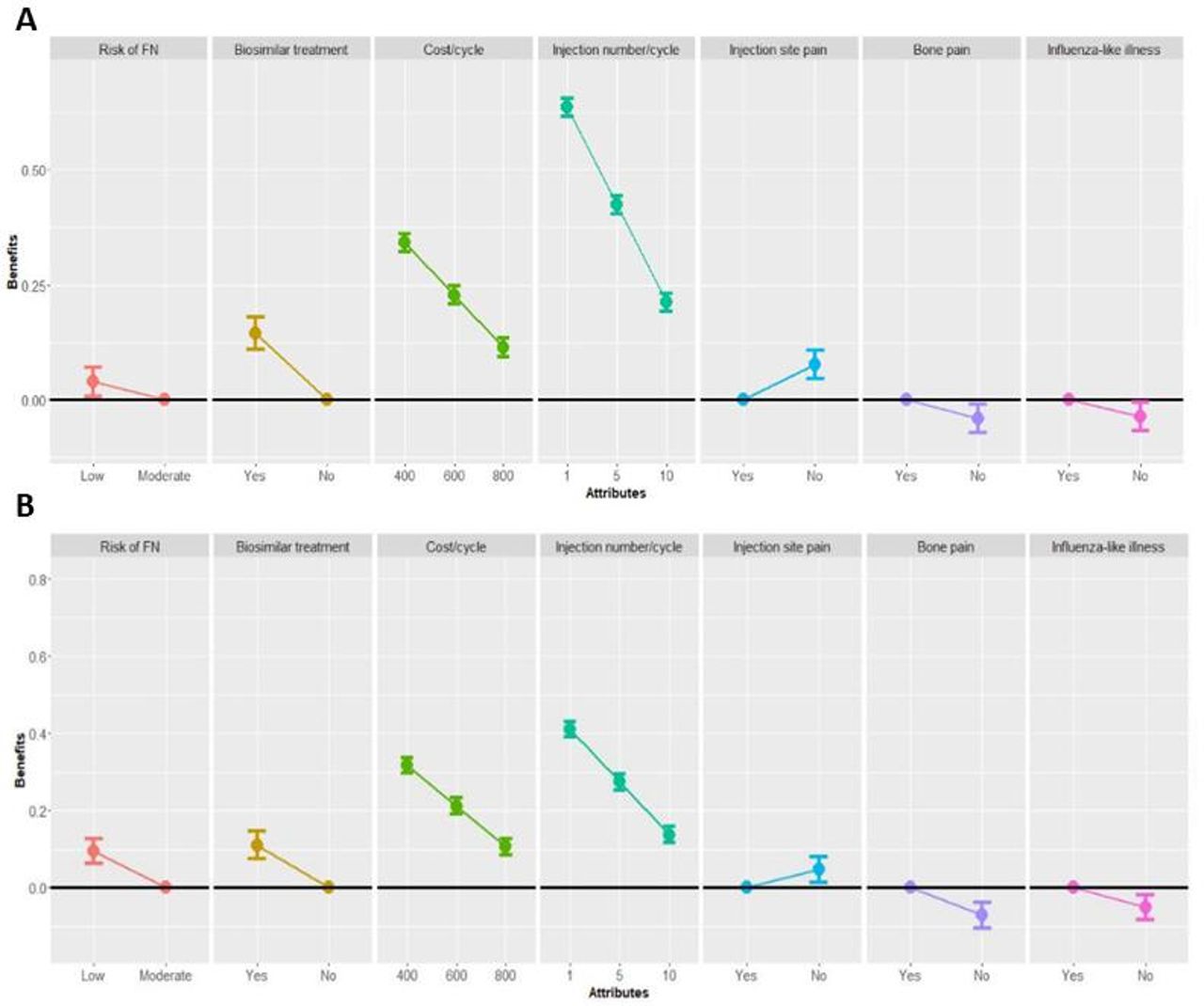
Analysis of the physicians’ preferences for G-CSF as primary (A) and secondary (B) prophylaxes. (A) Analysis of G-CSF preference for primary prophylaxis. (B) Analysis of G-CSF preference for secondary prophylaxis. FN, febrile neutropenia; G-CSF, granulocyte colony-stimulating factor.
Preferences were initially estimated for primary and secondary prophylaxes in the study population, and then in the subpopulations according to physician characteristics. For each analysis, an initial model was estimated that included all attributes. Subsequently, if certain coefficients were not significant, the associated attributes were discarded to estimate a more precise model. For all coefficients, the significance level was set at 5%. Modelling was performed using R V.3.6.3 and nlme package V.3.1.
Results
Study population
Between September 2018 and July 2019, of the 1684 physician solicited, 210 completed the DCE questionnaire via an electronic case report form. Of these, five were considered non-evaluable: one pulmonologist since the physician did not prescribe primary prophylaxis and four haematologists because they did not treat patients with solid tumours. Thus, finally the questionnaires completed by 205 physicians were analysed. The participants were predominantly male (61%), with ≤20 years of experience (76%), and working only in public hospitals (73%) (table 1).
Characteristics of participating physicians
The proportion of patients with breast, lung and digestive cancers treated by the participating physicians by medical specialty are shown in online supplemental table S3. Medical oncologists treated 42% (SD: 31%) of patients with breast cancer, 22% (SD: 25%) with digestive cancer and 14% (SD: 18%) with lung cancer. In contrast, oncology-certified pulmonologists treated almost exclusively patients with lung cancer (100%, SD: 0.2%). Similarly, oncology-certified gastroenterologists treated mainly patients with digestive cancers (95%, SD: 19%).
The participating physicians prescribe primary prophylaxis with G-CSF in 32% (SD: 20%) of patients, on average, treated with chemotherapy (table 2). The G-CSF prescribed was filgrastim in 46% (SD: 27%) of these patients and pegfilgrastim in 54% (SD: 27%). G-CSFs were more frequently prescribed by medical oncologists in 35% (SD: 21%) of their patients undergoing chemotherapy.
Primary prophylaxis with G-CSF used by physician: overall and according to medical specialty
Analysis of physician preference of G-CSF as primary prophylaxis (primary outcome)
For primary prophylaxis, all attributes selected were statistically significant table 3 and figure 1A. The number of G-CSF injections per chemotherapy cycle (coefficient: 0.212) and the cost per injection (coefficient: 0.114) were more important than efficacy and tolerance attributes in the choice of G-CSF. In addition, the use of a biosimilar did not hinder the use of G-CSF for primary prophylaxis (coefficient: 0.145).
Results from the analysis of the physician preferences for G-CSF as primary and secondary prophylaxes
Analysis of physician preference of G-CSF as secondary prophylaxis
For secondary prophylaxis (table 3 and figure 1B), all attributes were also statistically significant, and again the number of G-CSF injections per chemotherapy cycle (coefficient: 0.137) and the cost per injection (coefficient: 0.106) drove the decision. However, in the secondary prophylaxis setting, the efficacy of prophylaxis (coefficient: 0.094) had an increased importance. The use of biosimilars, as secondary prophylaxis, was well accepted (coefficient: 0.110).
The analysis of the G-CSF preference, for primary and secondary prophylaxes, according to medical specialty (online supplemental table S4 and figure S2), showed that the number of injections and convenience of treatment tended to be more important with oncology-certified pulmonologists and gastroenterologists compared with medical oncologists (coefficients per chemotherapy cycle 0.246 with oncology-certified pulmonologist, 0.255 with oncology-certified gastroenterologist vs 0.186 with medical oncologists). Interestingly, oncology-certified gastroenterologists (coefficient: 0.223) were more accepting of biosimilars than oncology-certified pulmonologists (coefficient 0.099) and medical oncologists (coefficient: 0.126).
{kind=link}
{kind=link}
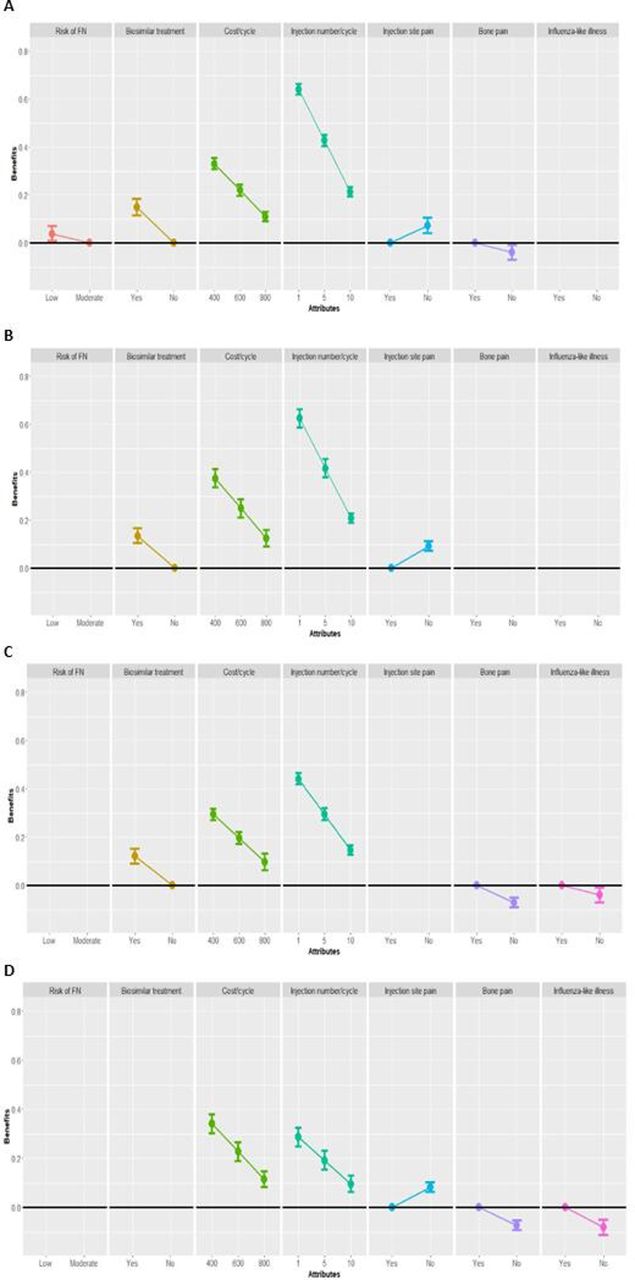
Analysis of the G-CSF preference, as primary and secondary prophylaxes, according to the healthcare sector in which the physicians work. (A) Physicians working in the public sectors: primary prophylaxis preference; (B) physicians working in the private sector (combined or not with the public sector): primary prophylaxis preference; (C) physicians working in the public sectors: secondary prophylaxis preference; (D) physicians working in the private sector (combined or not with the public sector): secondary prophylaxis preference. FN, febrile neutropenia; G-CSF, granulocyte colony-stimulating factor.
There are no significant differences for physician G-CSF preferences for primary or secondary prophylaxis according to the healthcare sector, either public sector only vs private sector (combined or not with the public sector), in which the physicians work (table 4 and figure 2A–D).
Analysis of the G-CSF preference for primary and secondary prophylaxis according to healthcare sector in which the physicians work
Discussion
In our study of a representative sample of French physicians prescribing G-CSFs, the attributes most significantly associated with the choice of G-CSF for primary prophylaxis were based more on cost and number of injections than on efficacy and tolerance attributes. In contrast, in addition to cost and number of injections, efficacy played a more important role in the choice of a G-CSF as secondary prophylaxis.
The participating physicians indicated that they prescribed G-CSFs as primary prophylaxis in 32% of their patients with cancer. The physicians prescribe G-CSF primary prophylaxis for 32% of patients: filgrastim in 46% and pegfilgrastim in 54%. However, oncology-certified pulmonologists tended to prescribe more pegfilgrastim.
Several studies have assessed G-CSF prescription in patients with cancer. A retrospective study assessed pegfilgrastim use in four outpatient sites of the Lifespan Comprehensive Cancer Centre (USA).17 The study found that pegfilgrastim, predominantly as primary prophylaxis, was prescribed when the chemotherapy used had a risk of FN of ≥20%. Interestingly, filgrastim was rarely used. The study found that pegfilgrastim prescription depended on cancer type. Among solid cancers, 35% of patients with breast cancer, 22% of patients with lung cancers, and 9% of patients with colorectal cancer received pegfilgrastim. A Dutch study assessed G-CSF use in 221 patients with breast cancer treated with neoadjuvant or adjuvant chemotherapy (either 5-fluorouracil, epirubicin or cyclophosphamide, then docetaxel or doxorubicin and cyclophosphamide then paclitaxel).8 FN occurred in 61 (28%) patients. However, G-CSF was administered only in 50 (23%) patients, mostly as secondary prophylaxis, with only 4 (8%) patients having primary prophylaxis due to their age and fragility. An Iranian prospective observational study assessed G-CSF prescription patterns during the first cycle of chemotherapy in patients with solid tumours.20 Of the 96 patients enrolled, 26 (27%) had primary prophylaxis as recommended (National Comprehensive Cancer Network (NCCN) guidelines).21 However, in the 70 patients for which G-CSF was not recommended, 60 (79%) patients received G-CSF. The G-CSF used was almost exclusively filgrastim (96% of the doses used).
There are several reasons for the inappropriate and inconsistent prescription of G-CSF.14 The cost-effectiveness of G-CSF used as primary and secondary prophylaxes remains controversial.
Our results clearly show that the choice of G-CSFs, in the primary and secondary settings, is driven by cost, in terms of the number of injections per cycle and cost per injection. The use of G-CSF biosimilars, although less costly, was not found to drive the decision but were well accepted as primary and secondary prophylaxes.
In our study, we observed that G-CSF efficacy played a more important role in the choice of secondary prophylaxis than for that of primary prophylaxis. This may be as expected since patients eligible for secondary prophylaxis are more likely to develop FN during subsequent cycles.
Considering the economic pressure on healthcare institutions, it is not surprising that the cost of prophylaxis, and not efficacy, impacts the physician decision to administer or not, both primary and secondary, G-CSF prophylaxis. Several European cost-effectiveness studies have assessed the benefit of G-CSF prophylaxis. A Belgian study assessed the benefit of prophylaxis in patients with stage II breast cancer treated with docetaxel and cyclophosphamide and patients with non-Hodgkin’s lymphoma treated with rituximab, cyclophosphamide, doxorubicin and vincristine, combined with prednisone from the Belgian payer perspective.22 The study found that primary prophylaxis with pegfilgrastim was more cost-effective than secondary prophylaxis with either pegfilgrastim, lipegfilgrastim, filgrastim or lenograstim in both cancers. Also, in Italy, primary prophylaxis with pegfilgrastim was reported to be more cost effective than filgrastim, despite a higher price per cycle for pegfilgrastim.23
In 2012, Aapro et al reported that in the European Union G5 countries (Germany, France, Italy, Spain, and the UK), the filgrastim biosimilar (Zarzio), compared with filgrastim (Neupogen) and pegfilgrastim (Neulasta), was the most cost-effective choice for prophylaxis or treatment of FN.11 A recent study accessing the economic impact of introducing a biosimilar pegfilgrastim in France24 concluded that biosimilar pegfilgrastim use would have a substantial financial benefit for the French Healthcare system. A similar financial benefit was obtained in a US pharmacoeconomic study assessing the benefit of using a biosimilar pegfilgrastim instead of the reference pegfilgrastim as prophylaxis for chemotherapy-induced FN.4
Despite its considerable cost and widespread use, the most effective duration of G-CSF as primary FN prophylaxis has remained unknown. A multicentre randomised trial has aimed to evaluate the optimal duration of filgrastim as primary FN prophylaxis in early breast cancer, which variates between 5 and 7 or 10 days. The study has demonstrated that 5 days was non-inferior to 7 or 10 days of filgrastim use with a difference in risk of either FN or treatment-related hospitalisation per cycle of 1.52% (95% CI 3.22% to 0.19%). Given the recognised toxicity and cost of this agent, as well as the impact on health economics and patient morbidity, this study suggested that the shorter duration should be considered standard of care.25
Interestingly, our results show the physician’s choice is driven by convenience, number of injections and cost. Indeed, the physicians reported that they prescribed both filgrastim and pegfilgrastim in about 50% of their patients. However, in the DCE, they indicated that G-CSF prophylaxis choice was driven by cost and number of injections. Indeed, pegfilgrastim requires only a single injection per cycle, while filgrastim requires multiple injections per cycle.
In this DCE analysis, the use of biosimilar G-CSFs was well accepted by physicians as both primary and secondary prophylaxes of FN. Several studies have found that G-CSF biosimilars have similar efficacy compared with the reference biologic in terms of preventing FN but with a reduced cost.12 26–28 Thus, the acceptability of biosimilars in France and the lower costs associated with biosimilars may increase the use of G-CSFs as prophylaxis in routine practice.
Study limitations
There are several limitations linked to the use of the DCE methodology. The attributes were selected based on those reported in the literature and selected by physicians to be clinically relevant. We have tried to make the scenarios as realistic as possible, but they can never completely simulate the complexity of decision making in the real world. The analysis of physician preference is based on scenarios with a limited number of attributes; the attributes chosen were those related to G-CSF. However, the type of chemotherapy and patient characteristics may also impact the physician’s choice of G-CSF prophylaxis. Finally, the study was performed among French physicians within the French healthcare system, leading to a limited number of respondents. However, the sample was sufficient to obtain satisfactory precision in the analysis and guaranteed a reliable geographical and specialty representativeness of French practitioners. Considering the variations in the price of G-CSFs and financial situations of national healthcare systems worldwide, our results cannot easily be extrapolated to other countries.
Conclusion
In France, the choice of G-CSF for primary and secondary prophylaxes is predominantly based on the number of injections (convenience) and the cost. G-CSF efficacy plays a more important role in the decision in the choice of secondary prophylaxis. Overall, biosimilar G-CSFs are well accepted by French physicians.
Data availability statement
No data are available. PrefmeG.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Mathilde Pouriel and Pierre Foulquie for the statistical analysis, Raphael Germain for the logistical management, Trevor Stanbury (Pro-Pens) and Siham Bibi for medical writing assistance, and all the doctors who participated for their investment in this study and for completing the questionnaire.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been made open access since it was first published.
Contributors FS, HS, PL, E-CA, NT, KG and CC analysed the data; NT and CS wrote the paper; CC revised the manuscript; and all authors approved this article.
Funding Mundipharma participated in the study conception, conduct and analysis, as well as the preparation of the manuscript for publication.
Competing interests FS benefited from assistance from Amgen, Roche, Pierre Fabre, Léo Pharma, Pfizer, BMS, Mylan, Vifor Pharma, Helsinn Healthcare, Mundipharma and MSD. HS benefited from assistance from Lilly, Pfizer, Tesaro, Novartis, Lilly, Vifor Pharma, Pierre Fabre, Mundipharma, Mylan, Sandoz, Roche and AstraZeneca. PL was a board member for Servier, Roche, Sanofi, Janssen, Ipsen, Pierre Fabre, Pfizer, Lilly, Novartis, Bristol Myers Squibb and MSD; received funding for congresses from Pierre Fabre, Pfizer and Novartis; and received funding for his institution from Lilly, Amgen, Roche and Merck Serono. E-CA benefited from assistance from AstraZeneca, Novartis, Pfizer, MSD, Lilly, Eisai and Pierre Fabre. KG was employed by Mundipharma. CC received fees for attending scientific meetings, coordinating research or consulting from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Roche, Sanofi Aventis, Bristol Myers Squibb, MSD, Lilly, Novartis, Janssen, Bayer, Mundipharma and Amgen.
Provenance and peer review Not commissioned; externally peer reviewed.