Article Text

Abstract
Objective P-cadherin can act both as a tumour suppressor and an oncogene. The clinical prognostic value of P-cadherin overexpression in breast cancer (BC) remains unclear. We conducted a study-level meta-analysis to determine whether P-cadherin expression can help predict prognosis in BC.
Methods A systematic literature search was performed to review eligible studies and clarify the relationship between P-cadherin overexpression and overall survival (OS), disease-free survival (DFS), pathological features, molecular subtypes and molecular phenotypes in BC.
Results Thirty-one studies including 12 332 patients were included. P-cadherin overexpression was correlated with significantly worse OS (HR=1.77, p<0.00001) and DFS (HR=1.96, p<0.00001) than P-cadherin-negative. P-cadherin overexpression could lead to high histological grade (OR=3.33, p<0.00001) and lymph node metastasis (OR=1.62, p<0.00001). Moreover, P-cadherin overexpression was associated with low odds of the luminal A subtype and high odds of the human epidermal growth factor receptor-2 (HER2)-positive and triple-negative subtypes. P-cadherin expression led to low expression of oestrogen and progesterone receptor (OR=0.37 and OR=0.36, respectively, both p<0.00001) and high expression of HER2 (OR=2.31, p<0.00001), Ki-67 (OR=2.79, p<0.00001), epidermal growth factor receptor (OR=5.85, p<0.00001) and cytokeratin 5/6 (OR=6.79, p<0.00001).
Conclusions P-cadherin was found to be associated with invasiveness and metastasis. P-cadherin expression can probably be a useful biomarker for predicting poor survival and may act as an independent prognostic predictor.
- cancer
- breast
- prognosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Breast cancer (BC) is a heterogeneous disease with high morbidity and mortality.1 2 Different disease stages, molecular subtyping and histological features underlie different biological characteristics and prognoses. BC is classified into hormone receptor-positive (oestrogen receptor (ER)+/progesterone receptor (PR)+), human epidermal growth factor receptor-2-overexpressing (HER2(+)) and triple-negative breast cancer (TNBC).3 Many prognostic indicators such as pathological grade, histological type, and HER2, ER, PR and Ki-67 status have been examined.4 5 However, these markers cannot accurately and reliably predict the prognosis of BC alone. Furthermore, there are no adequate molecular markers for predicting TNBC or inflammatory BC (IBC). Superior prognostic factors that can be evaluated in the primary tumour are necessary, and such biomarkers may also be novel therapeutic targets.
Recent studies have found that P-cadherin is differentially expressed in hormone receptor-positive BC, basal-like BC and HER2(+) BC. It can be regarded as an additional immunohistochemical marker of BC.6 The cadherin family includes epithelial (E), neural (N), retinal (R) and placental (P) cadherins,7 which mediate calcium-dependent cell–cell adhesion. However, their expressions have different implications. E-cadherin and P-cadherin play important roles in maintaining the structural integrity of epithelial tissues.8 However, the expression of P-cadherin is different from that of E-cadherin, although they share 67% homology and are both extremely important for the maintenance of cell shape and polarity.9 P-cadherin is expressed in the placental tissue, and in adults it is present only in the basal layers of stratified epithelia and is confined to the myoepithelial layer of the human mammary gland.10 It has not been fully examined at the molecular level.11
P-cadherin can act as a tumour suppressor or an oncogene.12 In BC, P-cadherin overexpression was reported to be correlated with increased tumour cell motility and invasiveness.13 There is a direct link between P-cadherin expression and the lack of ER-alpha signalling in BC cells, suggesting a role of P-cadherin in invasion.14 However, P-cadherin expression is crucial for the maintenance of normal breast epithelial architecture.15 Furthermore, the migration of mammary myoepithelial cells is compromised in the absence of P-cadherin.16 Recently, the expression of P-cadherin was found to be lower in normal breast tissue than in ductal carcinoma in situ and IBC, and the expression of P-cadherin was found to be higher in ER-positive and node-negative cancer and lower in node-positive cancer.17 18 Therefore, P-cadherin is an important biomarker of BC. However, its prognostic significance in relation to clinicopathological characteristics of BC has not been clearly established. Here, we conducted a systematic review and meta-analysis to determine whether P-cadherin expression can predict BC prognosis. For this study-level meta-analysis, the sample variance information was collected to analyse the correlation between P-cadherin expression and overall survival (OS), disease-free survival (DFS), histological grade, lymph node metastasis, tumour-node-metastasis (TNM) stage, molecular subtype and molecular phenotype, and was used to compute the variance of the estimated effect.
Methods
Identification of eligible studies
The PubMed, EMBASE and Chinese National Knowledge Infrastructure (CNKI) databases were searched without language limitations. We included studies published from January 1997 to August 2019. The protocol for this study has been published in Medicine and has been registered in the PROSPERO network (International Prospective Register of Systematic Reviews; registration number: CRD42019119880).19 The search terms are described in the protocol. The strategy used both MeSH terms and free-text words to increase sensitivity.
Additionally, printed journals and relevant textbooks were manually searched in the libraries of the Beijing University of Chinese Medicine, Peking Union Medical College and Guang’anmen Hospital, and specialised experts in particular fields were consulted for the necessary supplements.
Inclusion criteria were as follows: (1) female patients with a histological diagnosis of BC; (2) P-cadherin protein in the primary tumour tissues was assessed immunohistochemically; and (3) at least one of the following was reported: OS, molecular subtype, TNM clinical stage, lymph node metastasis, bad pathology grade, haematogenous metastasis or depth of tumour invasion.
Exclusion criteria were as follows: (1) reviews and single case reports; (2) studies referring to P-cadherin but not to human cancer; and (3) lack of outcome variables and clinicopathological features between P-cadherin and human cancer.
Data extraction and management
Three independent reviewers (RQ, SC and JJ) extracted data from eligible studies using a standardised collection form. We recorded the details of eligible studies, including first author, patient characteristics, publication year, pathology, P-cadherin assay methods, total cases, clinicopathological features and outcomes. If there were discrepancies between the reviewers, a final consensus was reached after a discussion with XZ. The HR was extracted directly if it was reported in the article or it was estimated using Kaplan-Meier survival curves and 5-year survival outcome events.20
Methodological assessment
Methodological assessment of eligible studies was conducted using a quality scale for biological prognostic factors (online supplementary file 1).21 Two specialists (QG and BH) who are experienced in clinical and basic experiments rated the studies. Disagreements between the two reviewers were discussed with JL, and a final consensus was reached.
Supplemental material
Statistical analysis
Statistical analyses were performed using Review Manager (RevMan) V.5.3.5 software (Cochrane Community, London, UK) and STATA V.14 software. Dichotomous data of the clinical pathological features were pooled using OR with 95% CI. HR was pooled as inverse variance data with 95% CI. P<0.05 was considered statistically significant. An observed HR or OR >1 implied worse prognosis for the group that was P-cadherin-positive and was considered statistically significant if the 95% CI did not overlap 1. The heterogeneity of the included studies was evaluated using the χ2 and I2 tests, and p<0.10 or I2 >50% was defined to indicate heterogeneity. The fixed effect model was used for pooling homogeneous data, and the random effect model was used for heterogeneous data. Publication bias and meta-regression were evaluated using the Egger’s test (STATA V.14), with p<0.05 indicating significant bias and a contribution of heterogeneity. Sensitivity analysis was performed by reanalysing the data using different statistical approaches.
Results
Included studies and characteristics
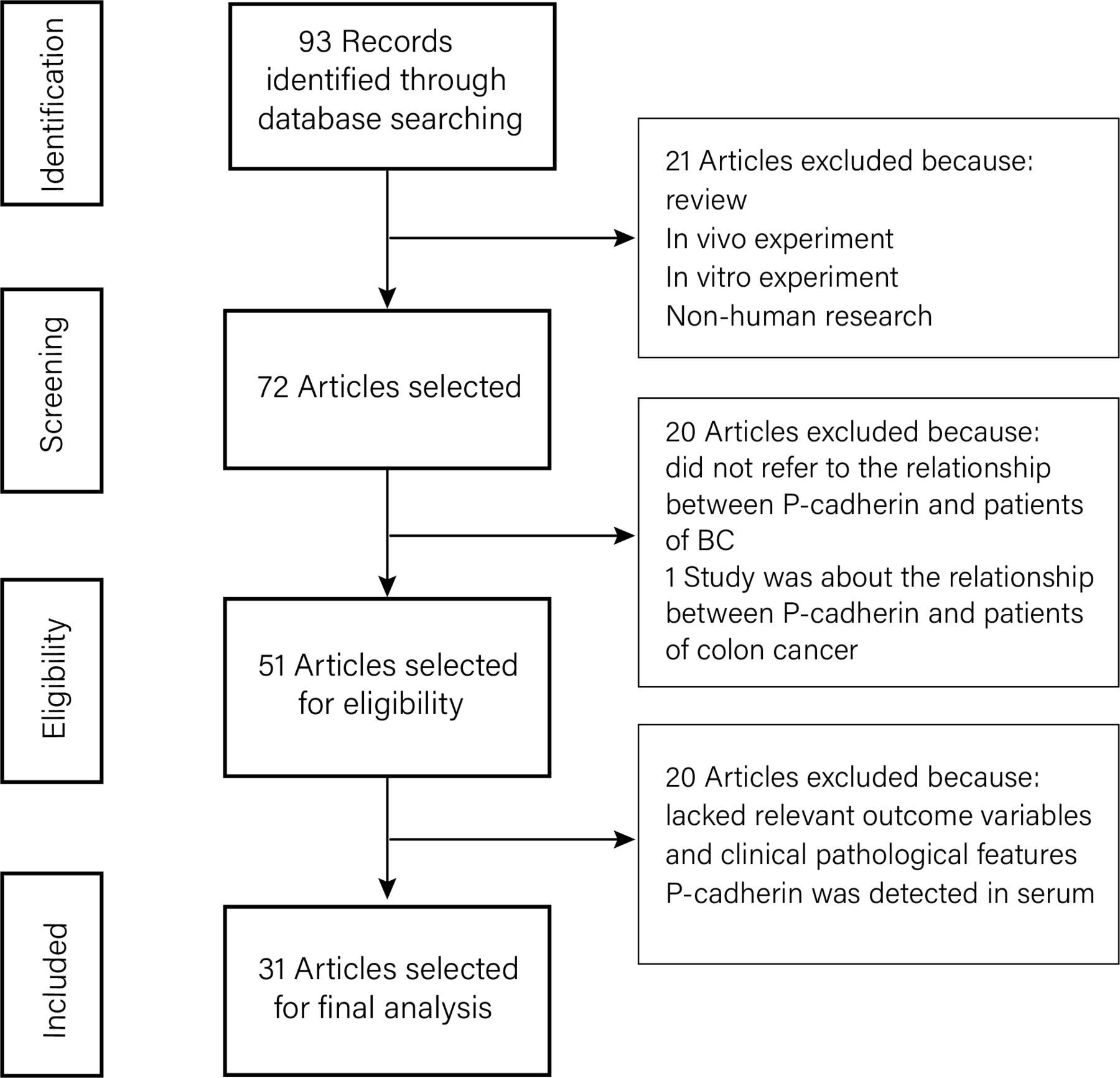
The initial search strategy identified 93 studies, of which 21 were excluded for the following reasons: review, in vivo experiment, in vitro experiment and non-human research. Another 20 studies were excluded because they did not refer to the relationship between P-cadherin and BC, and 20 studies were excluded because they lacked relevant outcome variables and clinical pathological features associating P-cadherin and human BC (figure 1).

Flow diagram of the literature search process. BC, breast cancer.
Finally, 31 studies with 12 332 patients were included (online supplementary table 1 in online supplementary file 2). Methodological assessment of eligible studies was conducted, as described in online supplementary table 2 in online supplementary file 2.
Supplemental material
Supplemental material
P-cadherin expression is associated with adverse prognosis
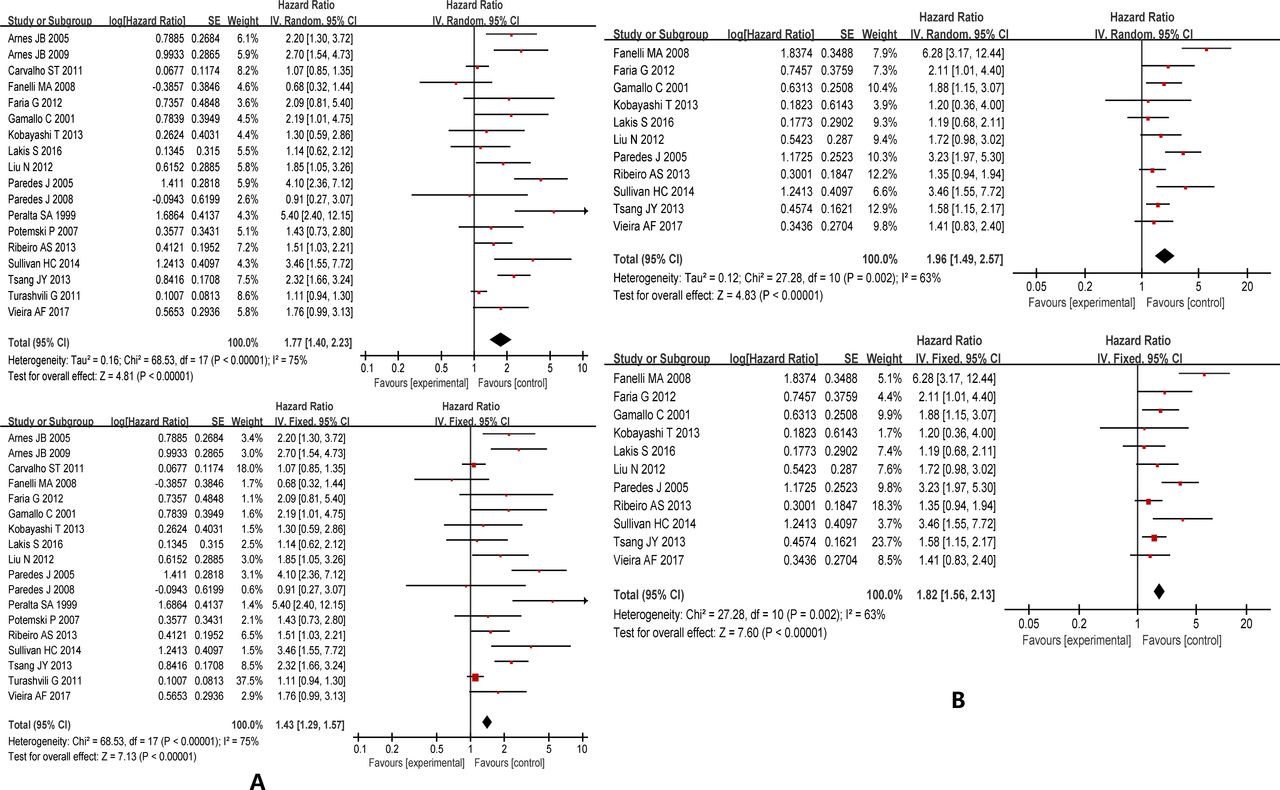
Eighteen studies reported the relationship between OS and P-cadherin expression. High P-cadherin expression was associated with worse OS (HR=1.77, 95% CI 1.40 to 2.23, random); however, significant heterogeneity was detected (I2=75%, p<0.00001). The same result was achieved in the sensitivity analysis using a fixed effect model (HR=1.43, 95% CI 1.29 to 1.57) (figure 2).
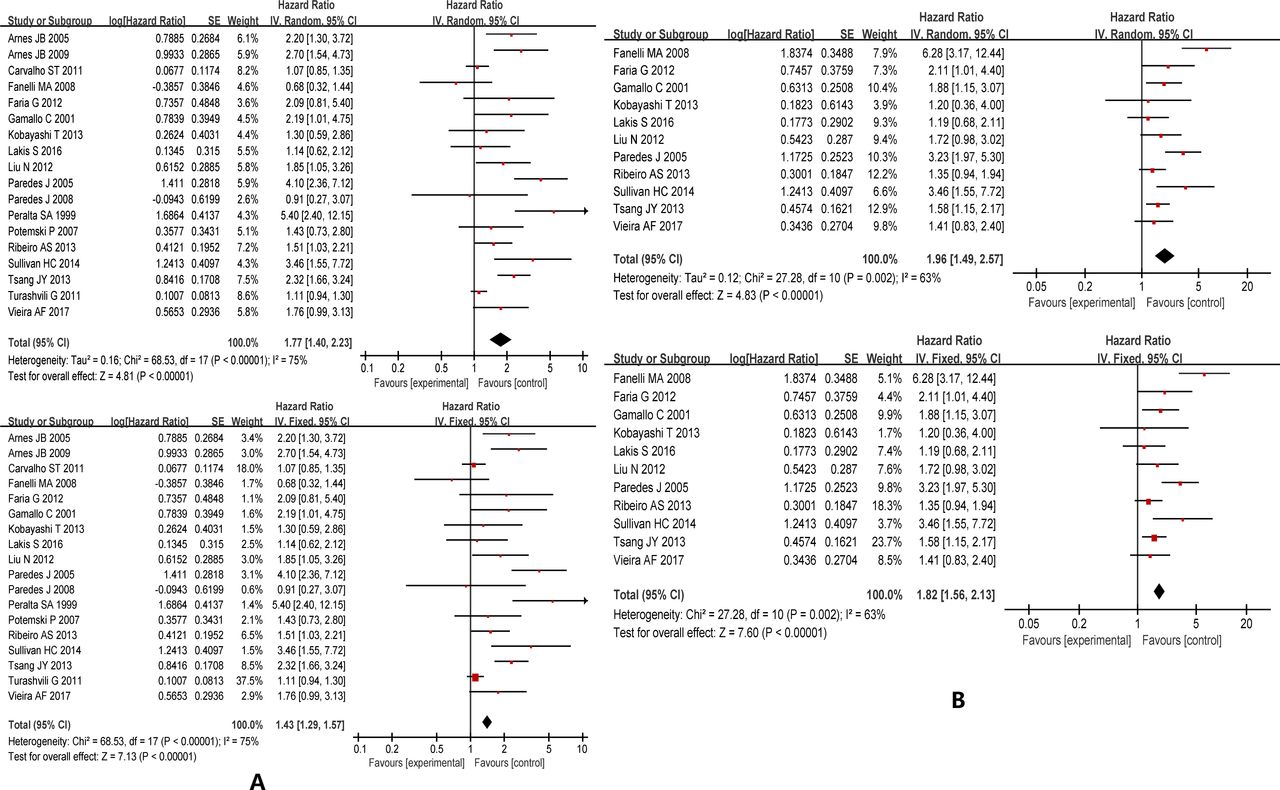
Forest plot of HR of overall survival (A) and disease-free survival (B) in random and fixed effect models. High P-cadherin expression was associated with poor overall survival and disease-free survival in the random model. Some heterogeneity was detected. The same result was reached in the sensitivity analysis using a fixed effect model.
The HRs of P-cadherin expression for OS were compared. Each individual study is represented by a red square, and the pooled data sets are indicated by a diamond, representing the 95% CI of each study. An HR >1 implies worse survival. The size of each study represents the weighting factor (1/SE) assigned to it.
P-cadherin expression indicates poor DFS
Eleven studies were found on the DFS of patients with cancer with P-cadherin expression. P-cadherin expression was associated with shorter DFS (HR=1.96, 95% CI 1.49 to 2.57, p<0.00001, I2=63%, random), but some heterogeneity was detected (I2=63%, p=0.002). The same result was reached in the sensitivity analysis using a fixed effect model (HR=1.82, 95% CI 1.56 to 2.13) (figure 2).
The HRs of P-cadherin expression for DFS were compared. Each individual study is represented by a red square, and the pooled data sets are indicated by a diamond, representing the 95% CI of each study. An HR >1 implies worse DFS. The size of each study represents the weighting factor (1/SE) assigned to it.
P-cadherin expression leads to high histological grade and lymph node metastasis
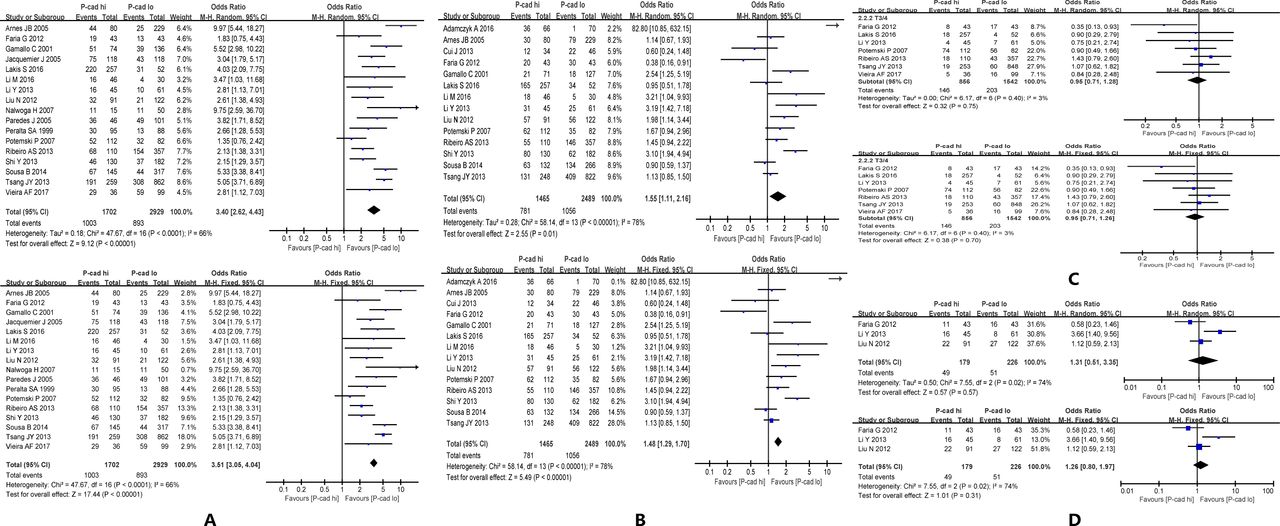
The prognostic significance of P-cadherin expression in histological grade 3 tumours was evaluated in 13 studies with 1896 patients. P-cadherin expression was associated with lower pathological differentiation in patients with BC (OR=3.40, 95% CI 2.62 to 4.43, p<0.00001, I2=66%, random). In 14 studies with 1837 patients, P-cadherin expression was significantly associated with lymph node metastasis (OR=1.55, 95% CI 1.11 to 2.16, p<0.00001, I2=78%, random). Significant heterogeneity was detected in these analyses, but the sensitivity analysis showed that the OR was not influenced by using different statistical approaches (OR=3.51, 95% CI 3.05 to 4.04, fixed; OR=1.48, 95% CI 1.29 to 1.70, fixed, respectively). There were no significant differences in P-cadherin expression based on tumour size or TNM clinical stage in both fixed and random effect models (table 1 and figure 3).
Meta-analysis of the clinical and pathological features of patients with breast cancer

Forest plot of the clinical and pathological features of patients with breast cancer in random and fixed effect models. (A) P-cadherin expression was associated with poor pathological differentiation in patients with breast cancer. (B) P-cadherin expression was significantly associated with lymph node metastasis. (C,D) There were no significant differences in P-cadherin expression based on tumour size or tumour-node-metastasis clinical stage in both fixed and random effect models.
P-cadherin expression differs based on BC subtype
Seven studies with 3788 patients evaluated the association between P-cadherin expression and luminal A/B subtypes. P-cadherin expression was associated with lower odds of the luminal A subtype (OR=0.19, 95% CI 0.11 to 0.33, p<0.00001, I2=88%, random), with significant heterogeneity. There was a discrepancy between the fixed effect and random effect models in the evaluation between P-cadherin and the luminal B subtype. Because significant heterogeneity was detected, the random effect model was used, and results showed that P-cadherin expression was not significantly associated with luminal B subtype (OR=0.76, 95% CI 0.56 to 1.02, p=0.06, I2=42%, random) (table 2 and figure 4).
Meta-analysis of patients with breast cancer based on molecular subtype

Forest plot of patients with breast cancer based on molecular subtype in random and fixed effect models. (A) P-cadherin expression was associated with lower odds of the luminal A subtype. (B) P-cadherin expression was not significantly associated with the luminal B subtype. (C,D) High P-cadherin increased the odds of the HER2(+) and TNBC/basal-like subtypes in both fixed and random effect models. HER2, human epidermal growth factor receptor-2; TNBC, triple-negative breast cancer.
Nine studies with 529 patients evaluated the relationship between P-cadherin and the HER2(+) subtype. Furthermore, 10 studies with 1115 patients evaluated the association between P-cadherin and TNBC/basal-like BC (table 2). Although significant heterogeneity was detected, the results showed that high P-cadherin increased the odds of the HER2(+) and TNBC/basal-like subtypes in both fixed and random effect models (table 2 and figure 4).
Relationship of P-cadherin expression with the expression of other BC markers
As shown in table 3, P-cadherin expression was significantly associated with low expression of ER and PR (OR=0.33, 95% CI 0.21 to 0.52, p<0.0001, I2=92%, random; OR=0.33, 95% CI 0.22 to 0.49, p<0.00001, I2=87%, random, respectively) and high expression of HER2 (OR=2.47, 95% CI 1.93 to 3.16, p<0.00001, I2=51%, random), Ki-67 (OR=2.65, 95% CI 1.94 to 3.62, p<0.00001, I2=66%, random), epidermal growth factor receptor (EGFR) (OR=6.04, 95% CI 4.05 to 9.03, p<0.00001, I2=45%, random) and cytokeratin (CK) 5/6 (OR=6.79, 95% CI 6.53 to 10.20, p<0.00001, I2=68%, random). Because significant heterogeneity was detected in the ER, PR, HER2, Ki-67 and CK5/6 evaluations, the random effect results were adopted, and the same results were achieved using a fixed effect model (table 4 and figure 5).
GRADE summary of findings

Forest plot of P-cadherin expression to the expression of other tumour markers in patients with breast cancer in the random effect model. P-cadherin expression was significantly associated with low expression of (A) oestrogen receptor and (B) progesterone receptor. P-cadherin expression was significantly associated with high expression of (C) human epidermal growth factor receptor-2, (D) Ki-67, (E) epidermal growth factor receptor and (F) cytokeratin 5/6.
Relationship of P-cadherin expression to the expression of other tumour markers in patients with breast cancer
Subgroup analyses
Because heterogeneity was observed, subgroup analyses were performed based on publication date, region, sample size, cut-off value, survival analysis, follow-up time and quality score (table 5).
Subgroup meta-analysis for OS
We assessed the impact of P-cadherin expression on OS in four regions—Asia (HR=2.06, 95% CI 1.57 to 2.70, p<0.00001, I2=0%, fixed), Europe (HR=1.92, 95% CI 1.48 to 2.49, p<0.00001, I2=42%, random), North America (HR=2.60, 95% CI 0.86 to 7.84, p=0.09, I2=90%, random) and South America (HR=1.43, 95% CI 1.29 to 1.57, p<0.00001, I2=21%, fixed)—and detected significant heterogeneity in North American patients.
We observed a significant association between high expression of P-cadherin and good OS regardless of the publication date (before 2010: HR=1.87, 95% CI 1.20 to 2.92, p=0.006, I2=67%, random; after 2010: HR=1.53, 95% CI 1.21 to 1.94, p=0.0004, I2=68%, random), sample size (>300: HR=1.57, 95% CI 1.10 to 2.24, p=0.01, I2=80%, random; <300: HR=1.90, 95% CI 1.35 to 2.66, p=0.0002, I2=74%, random), cut-off value (HR=1.77, 95% CI 1.40 to 2.23, p<0.00001, I2=75%, random), survival analysis (univariate: HR=1.78, 95% CI 1.24 to 2.54, p=0.002, I2=73%, random; multivariate: HR=1.78, 95% CI 1.25 to 2.52, p=0.001, I2=78%, random), follow-up time (5 years: HR=2.33, 95% CI 1.14 to 4.75, p=0.02, I2=70%, random; 10 years: HR=1.69, 95% CI 1.32 to 2.16, p<0. 75%, random) and quality score (>72: HR=1.77, 95% CI 1.32 to 2.37, p=0.0002, I2=71%, random; <72: HR=1.80, 95% CI 1.15 to 2.81, p=0.01, I2=81%, random). Because significant heterogeneity was detected among these subgroups, we adopted the results of the random effect model (table 5 and figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of subgroup of overall survival in random and fixed effect models. A significant association was observed between high expression of P-cadherin and good overall survival regardless of publication date, sample size, cut-off value, survival analysis, follow-up time and quality score. Because significant heterogeneity was detected, the results of the random effect model were adopted.
Publication bias
The possibility of publication bias was evaluated using Egger’s test (online supplementary file 3). The Egger’s test suggested that publication bias may have had a significant influence on the results of the HR for OS (p=0.018) but not on DFS (p=0.254).
Supplemental material
The Egger’s test is based on a linear regression of the standard normal deviate against its precision. In our analysis, we used the inverse of the SE as an independent variable and the standardised estimate of the size effect (log HR on its SE) as a dependent variable. The estimate of the effect is considered biased if the intercept is significantly different from zero.
Discussion
P-cadherin is a transmembrane glycoprotein involved in calcium-dependent cell–cell adhesion and a potential therapeutic target in cancer.22 First, P-cadherin expression is crucial for the maintenance of normal breast epithelial architecture.23 Overexpression of P-cadherin may predict adverse effect on survival prognosis. The invasive nature of P-cadherin was confirmed in vitro, which makes P-cadherin a possible therapeutic target for BC.14 Actually, several highly selective human monoclonal antibodies against P-cadherin have shown significant antitumour and antimetastatic activities in distinct P-cadherin-overexpressing tumour model.24 Some explorations to select P-cadherin as a target are also underway. For example, a CD3-bispecific molecule targeting P-cadherin causes T cell-mediated regression of established solid tumours in vivo.25 It is generally believed that P-cadherin is important in the prognosis and treatment of BC. Many studies have assessed the relationship between P-cadherin levels and prognosis in BC; however, no consensus has been reached. We conducted a systematic and comprehensive meta-analysis to assess this relationship. This study also provided effective indicators for the clinical treatment of BC and useful information for clinical decision-making.
We performed this meta-analysis to assess whether P-cadherin expression affects prognosis in patients with BC. Overexpression of P-cadherin was observed in 38.18% of 12 332 patients. There was a significant correlation between P-cadherin expression and worse OS and DFS, indicating that P-cadherin overexpression is deleterious for patients with BC. This result is consistent with Peralta Soler et al’s26 finding, which showed that the expression of P-cadherin in breast carcinoma is associated with shorter survival of BC, so it was considered as a prognostic predictor. However, the results of different clinical studies are inconsistent. Carvalho et al27 found that P-cadherin was not associated with worse prognosis for stage IIA patients. Our results provide a conclusion as to whether P-cadherin can be used as a prognostic factor for BC and then guide clinical practice. A recently published systematic review which included 11 studies supports this finding.28 It was found that the overexpression of P-cadherin is linked with adverse prognosis of BC, even though the prognosis of survival was not affected by the subtype of BC. Different subtypes of BC are treated differently; thus, the prognosis of P-cadherin in various subtypes of BC may not be easy to evaluate. Therefore, the correlation between P-cadherin and histopathological information that can determine the degree of malignancy needs to be analysed.
The expression of P-cadherin could lead to bad pathological differentiation and lymph node metastasis in patients with BC. Several studies have described the relationship between P-cadherin and mortality risk in patients with BC. Rakha et al29 indicated that a high grade of BC was associated with P-cadherin expression. Besides, P-cadherin expression was correlated with various molecular subtypes in this review. Based on these results, correlation analysis of P-cadherin was carried out for molecular subtype markers such as ER, PR, HER2 and Ki-67. P-cadherin has been found to be a marker for different types of BC. Matos et al30 indicated that P-cadherin can be used as a marker for basal-like BC, and another study indicated that P-cadherin is probably one of the most useful adjunct markers to distinguish basal-like ductal carcinomas in situ.31 In the analysis of P-cadherin and molecular subtypes, high expression of P-cadherin was negatively associated with the luminal A subtype and positively associated with the HER2(+) and TNBC subtypes. The luminal A and B subtypes have the best prognosis among the molecular subtypes.32 However, P-cadherin expression was not significantly associated with the luminal B subtype. We analysed markers that affect molecular typing and reflect BC cell proliferation. We found that P-cadherin expression led to low expression of ER and PR and high expression of Ki-67. This also explains why there is no significant correlation between P-cadherin expression and the luminal B subtype. P-cadherin expression was also found to be associated with high expression of HER2, EGFR and CK5/6. Turashvili et al33 also demonstrated that P-cadherin expression was positively associated with Ki-67, EGFR and HER2 expression. Sousa et al34 found that P-cadherin expression has higher sensitivity for TNBC and is more reliable than the classic standard pair CK5/EGFR. Arnes et al35 also found that P-cadherin is a biomarker for basal-like BC or TNBC and has a significant association with BRCA1 mutation. Tsang et al36 demonstrated that P-cadherin was associated with basal features and did not show a significant negative association with the luminal B subtype; thus, it was not recognised as a good marker for identifying TNBC alone. The result of this systematic review proves that P-cadherin is an indicator of significantly worse survival and high invasiveness. In addition, P-cadherin is a favourable factor for the expression of HER2 and Ki-67, and it expressed lower when ER or PR positive. This also supports the adverse prognosis of P-cadherin.
Considering the various quality and heterogeneity of included studies, we also considered the influence of different regions, research age and follow-up time on the analysis of each study. A meta-regression analysis found that the cut-off value had a significant association with the interstudy heterogeneity, indicating that the cut-off value might account for part of the interstudy heterogeneity. Subgroup analysis could not be performed to explore this as a source of heterogeneity because the studies used the same antibody. The molecular mechanism might also contribute to the heterogeneity. P-cadherin expression is affected by p120ctn, a cell adhesion protein belonging to the cadherin/catenin family.37 Several reports have indicated that p120ctn can associate with all the classic cadherin subtypes and is involved in the regulation of cell migration and adhesion.38 An in vitro experiment showed that cell motility induced by increased P-cadherin expression was due to the activation of Rac1 and Cdc42 through the accumulation of p120ctn in the cytoplasm.13 39 This mechanism might also be applicable to BC; however, few studies have assessed p120ctn in BC. In addition, regional differences may also cause interstudy heterogeneity. In the subgroup analysis of the OS, significant heterogeneity among North American patients was observed. One possible reason may be the different cut-off values of P-cadherin staining in tumour cells. For two studies, P-cadherin staining of 10% of the tumour cells was considered to be positive expression. However, for one study, P-cadherin staining of 50% or more of the tumour cells was considered to be positive expression; this study included 1000 people, the largest weighting. Besides, P-cadherin expression of BC in different races may contribute to significant heterogeneity. Studies have shown that African–American women are more likely to have triple-negative or basal-like breast BC.40 Finally, 31 studies met all the inclusion criteria.41 42 ,43 ,44 ,45 ,46 ,47 ,48 ,49 The characteristics of nine of these studies are only shown in online supplemental file 2-Table 1. For our study, P-cadherin expression increased the odds of the triple-negative/basal-like type in both fixed and random effect models. Thus, race might be one of the reasons for the heterogeneity in North American patients.
There are some limitations to this study. First, bias was unavoidable for the clinical evidence because the relevant data were extracted from non-randomised controlled trials. Second, there were no uniform scoring criteria to define high P-cadherin expression. Third, because not all databases were searched, some publication/language bias may be present. Finally, differences in clinical characteristics such as age, weight, height and treatment in each study will obviously lead to bias. Further investigations should determine whether these factors influence the results of the meta-analysis.
In conclusion, our meta-analysis suggests that overexpression of P-cadherin is not only significantly associated with worse OS and DFS in BC but also with clinicopathological features, including high histological grade, lymph node metastasis, molecular subtype and molecular phenotype. Overexpression of P-cadherin can probably act as a useful biomarker for predicting adverse effect on survival and P-cadherin can be an independent prognostic predictor. Hopefully, this finding may provide effective indicators for the clinical treatment of BC.
The PRISMA checklist for systematic reviews and meta-analyses has been provided in online supplementary file 4.
Supplemental material
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
RQ, JL, SC, JJ and XZ contributed equally.
BH and QG contributed equally.
Contributors QG and RQ contributed to study concepts. BH, JL, QG, RQ, SC, JJ and XZ contributed to study design. RQ, SC, JJ, BY and XZ contributed to data acquisition. BH, RQ, JL and QG contributed to quality control of data and algorithms. RQ, JL, BY, YY, QG, SC and ZJ contributed to data analysis and interpretation. RQ, SC, JJ and BY contributed to statistical analysis. RQ, JJ, SC, BY, QG, BH and XZ contributed to manuscript preparation. RQ, JJ, SC, ZJ, QG, YY, BH and XZ contributed to manuscript editing. YY, BH and ZJ contributed to manuscript review. All authors gave final approval for submission of the manuscript.
Funding This study was funded by Specialized Training for Outstanding Young Scientific and Technological Talents (Innovation) of the China Academy of Chinese Medical Sciences.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.