Article Text

Abstract
Objectives Despite the escalating public health emergency related to opioid-related deaths in Canada and the USA, opioids are essential for palliative care (PC) symptom management.
Opioid safety is the prevention, identification and management of opioid-related harms. The Delphi technique was used to develop expert consensus recommendations about how to promote opioid safety in adults receiving PC in Canada and the USA.
Methods Through a Delphi process comprised of two rounds, USA and Canadian panellists in PC, addiction and pain medicine developed expert consensus recommendations. Elected Canadian Society of Palliative Care Physicians (CSPCP) board members then rated how important it is for PC physicians to be aware of each consensus recommendation.
They also identified high-priority research areas from the topics that did not achieve consensus in Round 2.
Results The panellists (Round 1, n=23; Round 2, n=22) developed a total of 130 recommendations from the two rounds about the following six opioid-safety related domains: (1) General principles; (2) Measures for healthcare institution and PC training and clinical programmes; (3) Patient and caregiver assessments; (4) Prescribing practices; (5) Monitoring; and (6) Patients and caregiver education. Fifty-nine topics did not achieve consensus and were deemed potential areas of research. From these results, CSPCP identified 43 high-priority recommendations and 8 high-priority research areas.
Conclusions Urgent guidance about opioid safety is needed to address the opioid crisis. These consensus recommendations can promote safer opioid use, while recognising the importance of these medications for PC symptom management.
- cancer
- chronic conditions
- clinical decisions
- education and training
- pain
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What was already known?
The opioid crisis has had an effect on all aspects of society, particularly in the USA and Canada.
Guidelines on management of opioid safety have focused on chronic non-cancer pain populations to the exclusion of palliative care.
What are the new findings?
Our Delphi Study developed 130 expert consensus recommendations to promote opioid safety in adults receiving palliative care.
The resulting recommendations provide a necessary paradigm shift from the long-held view that opioid use disorder is rare among patients receiving palliative care.
What is their significance?
Clinical
Healthcare providers, administrators, educators and policy makers should be aware of the 43 high-priority recommendations.
Improved care plans are suggested that include identification of patient and caregiver risks related to opioid use.
Research
Eight high-priority topics have been identified.
Key areas include adaptation of urine drug screening and validation studies to better identify screening tools for opioid use disorder in palliative care.
Introduction
Globally, approximately 115 000 people died in 2017 from opioid-related overdoses, with nearly half of these deaths occurring in the USA and Canada.1–5 The opioid crises in these countries have accelerated since the onset of the COVID-19 pandemic, with opioid-related deaths in the USA increasing by 38% during May 2019–2020 compared with June 2018–2019.6 Multiple factors are contributing to the worsening of the opioid crisis, including increase in substance use as a coping mechanism, and restricted access to mental health and addiction services.7 Though most opioid-related hospitalisations and deaths are caused by fentanyl and its analogues, 27%–38% of deaths are from prescription opioids used by patients or diverted to others.1 8 Problematic use of prescription opioids is highly associated with the development of opioid use disorders (OUDs) and opioid-related overdoses.9 10 Nevertheless, prescription opioids are essential for symptom management, especially in palliative care (PC).11
PC improves the quality of life for people with life-limiting illnesses through symptom management and psychosocial support.12 Opioids are mainstay medications in PC, with strong evidence for their effectiveness in managing pain, dyspnoea and cough.13 14 Current PC guidelines focus primarily on how to prescribe opioids for symptom management, rather than prevention, detection and management of opioid-related harms.15–17 Most existing knowledge about opioid safety is from chronic non-cancer pain and addiction medicine but this evidence cannot be directly applied to all patients receiving PC. In the absence of a strong evidence base for opioid risk mitigation strategies in PC, knowledge synthesis and expert opinion are necessary to inform practice and research.18–20 Therefore, the Delphi Study objectives were to develop expert consensus recommendations that can be used by healthcare providers, administrators, educators and researchers to promote opioid safety in adult patients receiving PC. In doing so, we were mindful of the dual obligations of delivering effective symptom relief for people receiving PC, and managing opioid safety for patients, their families and society.
Methods
Study design
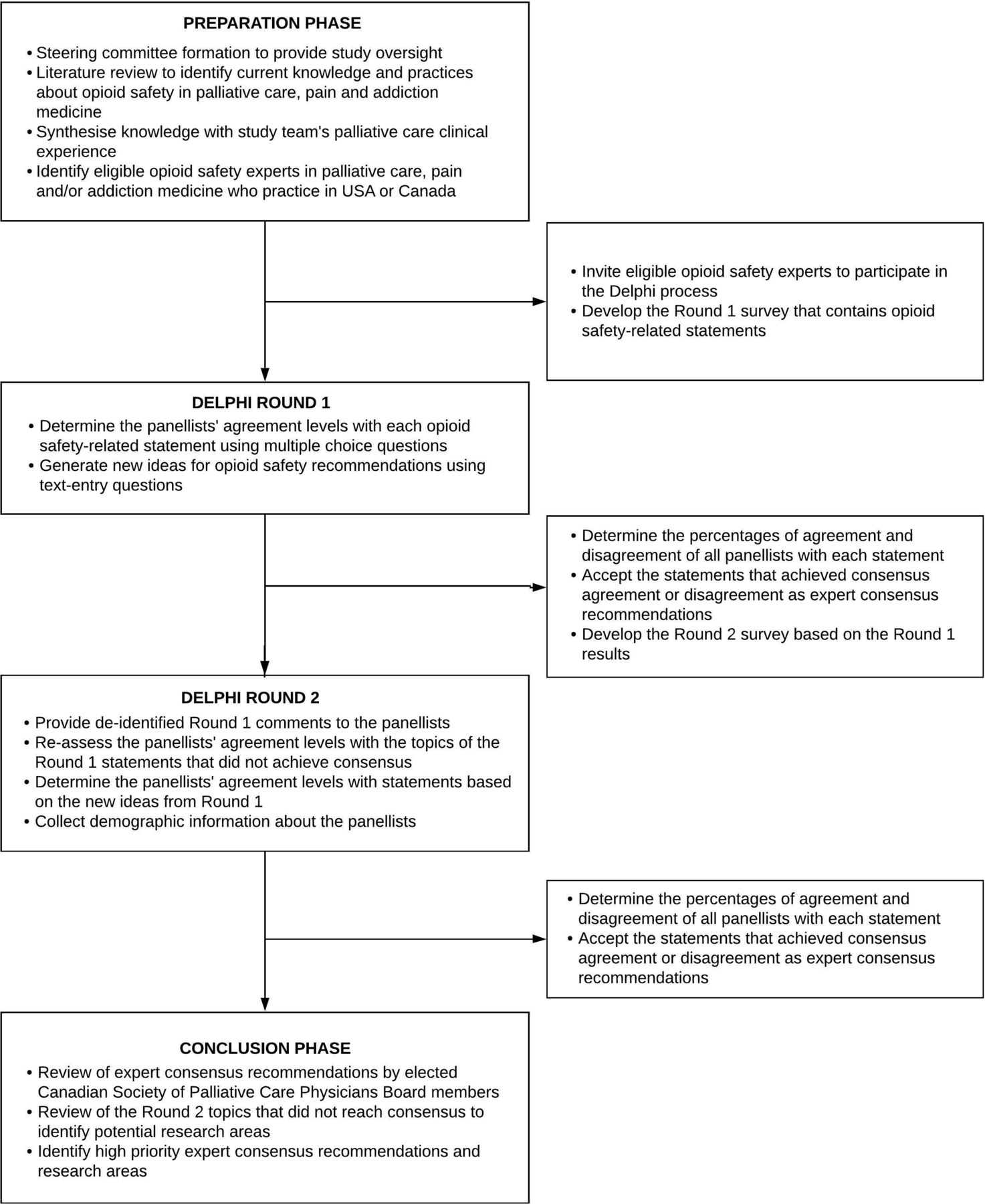
The Delphi technique was used to develop expert consensus recommendations about opioid safety for adult patients receiving PC. This technique has been employed in medical and nursing research ‘to form consensus or explore a field beyond existing knowledge and the current conceptual world’.21 22 We used the Conducting and Reporting of Delphi Studies in Palliative Care recommendations to design, conduct and report our study.21 Our Delphi process involved four phases: (1) Preparation phase, (2) Round 1, (3) Round 2 and (4) Conclusion phase (figure 1). A steering committee of eight leaders in addiction medicine (n=2), pain medicine (n=2) and PC (n=4), from the USA (n=2) and Canada (n=6), provided study oversight from design to knowledge dissemination.

The Delphi process.
Preparatory phase
Guiding definitions
The following definitions were used to guide the Delphi process: (1) PC: ‘an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual’,12 (2) Opioid safety: prevention, identification and management of aberrant medication taking behaviours (AMTBs), OUD and opioid-related overdoses, (3) AMTB: ‘any use of prescription opioids in a manner other than intended by the prescribing physician and pharmaceutical manufacturer’23–25 and (4) OUD: problematic patterns of opioid use, which result in clinically significant impairment or distress.26
Expert panel and recruitment
The Delphi technique uses a structured, consensus process to engage expert panellists with diverse backgrounds.21 Previous studies suggest that there is no added benefit for more than 30 panellists.27 Therefore, we aimed to involve a total of 30 panellists in Canada (n=15) and the USA (n=15), who practised in PC (n=10), pain medicine (n=10) and addiction medicine (n=10). We recruited panellists from these disciplines and countries because of their opioid safety experience within the context of the USA and Canadian opioid crisis. Potential panellists were identified through literature review, professional organisation memberships and steering committee recommendations. Further snowball sampling was used to attain our target sample size.
Experts were eligible if they were fluent in English, had at least 5 years of clinical practice in PC, pain or addiction medicine, and completed at least one of the following opioid safety-related work within the last 7 years: healthcare professional or public education, research, quality improvement, policy development and/or advocacy. All panellists were asked to declare their real, potential or perceived conflicts of interest. We provided each participant with a small incentive ($15.00 coffee gift card).
Delphi rounds
Our Delphi process contained two Delphi rounds; each round involved online survey distribution using the survey software, Qualtrics. Data were collected between 1 August 2018 and 30 April 2019, with each round lasting 4–6 weeks. Email reminders were sent 2 weeks after the initial distribution of each survey. Both surveys were in English and included information about the study, guiding definitions and ethics. The panellists were informed that they were providing consent to participate in the study by completing the surveys.
The two surveys used three multiple-choice question formats to evaluate the panellists’ levels of agreement with opioid safety-related statements and items. The first format instructed the panellists to select their agreement level to a statement or item using a five-point Likert Scale (strongly disagree, disagree, neutral, agree, strongly agree). The second format allowed the panellists to choose multiple options from a list of items. The third format allowed them to choose only one option from a list of possible answers. Based on the panellists’ percentages of agreement (or disagreement), we determined whether to accept a statement or item as an expert consensus recommendation.
Delphi Round 1
We conducted a scoping review28 that identified limited evidence regarding opioid safety in PC, pain and addiction medicine; therefore, the study team and steering committee used their clinical experience in PC, pain and addiction medicine to create the Round 1 survey, which contained six domains (figure 2). Domain 1 focused on general principles about opioid prescribing for patients with life-limiting illnesses. The remaining domains focused on key stakeholders who should be engaged to promote and ensure opioid safety: healthcare organisations, PC training programmes and PC clinical programmes (Domain 2); healthcare providers (Domains 3, 4, 5), and patients and caregivers (Domain 6). The result was a survey that was used to generate comprehensive recommendations about opioid safety in PC.

Opioid safety domains and key stakeholders.
The purpose of Round 1 was to determine the panellists’ agreement level with statements and items related to each of the six domains and to generate new ideas. Before distribution to the panellists, the survey was reviewed by the steering committee and piloted by five clinicians (PC n=4, addiction medicine n=1). In total, the Round 1 survey contained 122 multiple-choice questions. Open-ended feedback was collected using seven text-entry questions. The online supplemental appendix 1 presents seven tables that contain all the multiple-choice question stems and text-entry questions included in the Delphi surveys.
Supplemental material
Delphi Round 2
The purpose of Round 2 was to evaluate topics that did not reach consensus or that were newly suggested in the Round 1 comments, and to collect demographic information about the panellists. De-identified verbatim comments from Round 1 were collated and shared with the experts to examine whether group-level feedback would enable them to form consensus. In total, the Round 2 survey contained 86 multiple-choice and 8 text-entry questions (online supplemental appendix 1). Three of the multiple-choice questions evaluated the panellists’ agreement (‘yes’ or ‘no’) with summaries derived from Round 1 recommendations. The topics of these summaries were: items that should be used to identify patients with life-limiting illnesses who are at high-risk of AMTB (n=20) and opioid-related overdose (n=17); and methods to deliver opioid safety education (n=4).
Conclusion phase
The Canadian Society of Palliative Care Physicians (CSPCP) is a national organisation composed of physicians with special interest in PC (eg, regional programme leads, educators).29 In December 2020, we invited CSPCP to identify high-priority recommendations and areas of research that can be most helpful and impactful for CSPCP members. Five current and formerly elected CSPCP Board Members were asked to rate how important it is for PC physicians to be aware of each consensus recommendation using a 5-point Likert Scale, where 0 was ‘not at all important’ and four was ‘extremely important’. Using the same scale, they also reviewed the topics that did not reach consensus in Round 2 and rated how important it is for research to be conducted about them.
Data analysis
The data were de-identified before analysis. We used descriptive statistics (IBM SPSS Statistics V.27) to analyse the quantitative data from the multiple-choice questions. The percentages of agreement and disagreement to each statement and item was calculated based on all the panellists’ responses after each round. A priori, consensus agreement was defined for the 5-point Likert Scale questions as ≥80% of the panellists agreeing (‘agree’ and ‘strongly agree’) with a statement.21 30 31 For the remaining questions, we defined agreement as ≥80% of the panellists selecting ‘yes’ or a multiple-choice option. Consensus disagreement was defined similarly but with ≥80% disagreement (‘disagree’ and ‘strongly disagree’) with a statement or item. If a statement or item reached consensus agreement or disagreement, it was accepted as a consensus recommendation. Based on the CSPCP ratings of importance, recommendations were deemed as high priority if they had average ratings of ≥3, where 3 was ‘very important’. Descriptive analysis was also conducted for the panellists’ demographic data, whereas content analysis was used to examine the text-entry question responses.
Results
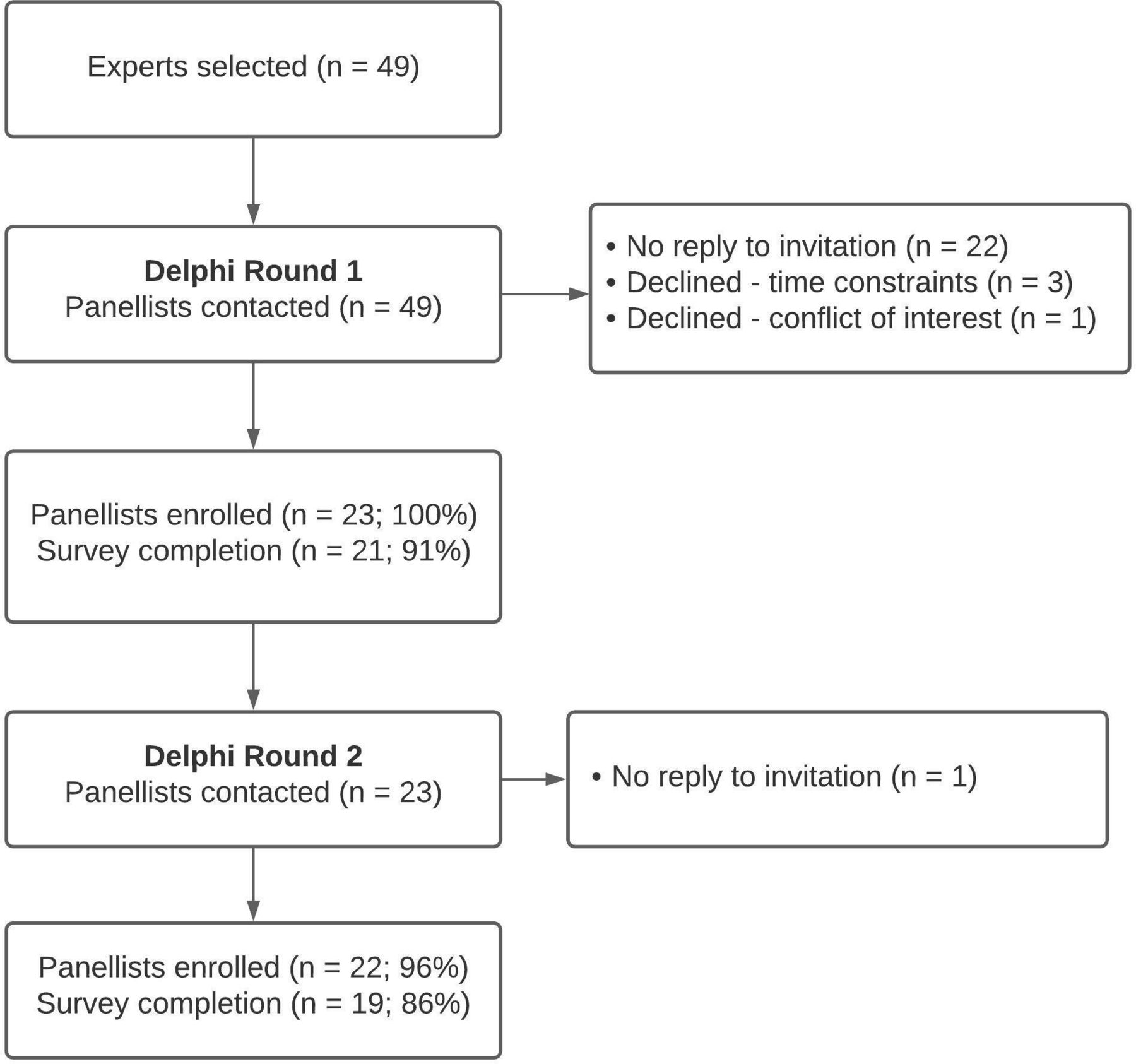
Out of 49 experts who were invited, 23 (47%) were enrolled as panellists (figure 3). One enrolled expert was recommended by another expert. The 23 panellists were primarily from Canada (n=14, 61%) and specialised in PC (n=10, 43%). Additional demographic data were provided by 22 (96%) of the panellists: the majority were from urban settings (n=21, 95%), and were employed as clinicians (n=22, 100%) and educators (n=18, 82%) in academic workplaces (n=16, 73%). They were involved in all types of opioid-safety related work, with the most common being education of healthcare professionals (n=20, 91%) and patients (n=18, 82%) (table 1).

{kind=link}
{kind=link}
{kind=link}
Flow chart of the panelists in the Delphi Study.
Characteristics of panelists
In Round 1, 21 (91%) panellists completed the entire survey, and reached consensus for 103/122 (84%) statements and items. From the 23 panellists in Round 1, 22 (96%) agreed to participate in Round 2 and, of these, 19 (86%) completed the Round 2 survey. Consensus was achieved for an additional 27/86 (31%) statements and items. In total, the Delphi process resulted in 130 expert consensus recommendations (127 individual statements, 3 summaries) about opioid safety for adult patients receiving PC (online supplemental table and table 2), of which 43 were rated as high priority by the CSPCP. From the 59 statements and items that did not achieve consensus in Round 2, CSPCP identified 8 high-priority research topics (table 3).
Supplemental material
Summaries of recommended items used to identify patients with life-threatening illnesses who are at high risk of aberrant opioid medication-taking behaviours and opioid overdose
High-priority palliative care opioid safety research topics
Domain 1: General principles
Domain 1 focused on general principles to guide opioid prescribing and identification, and management of OUD in PC. The panellists developed a total of 12 recommendations, and 6 were deemed high priority by CSPCP (online supplemental table , #1–#12). The high-priority recommendations were as follows: Opioids should not only be prescribed by PC specialists to patients with life-limiting illnesses. Opioid prescribing should be part of the practices of all clinicians caring for patients with life-limiting illnesses, such as family physicians and oncologists. If needed, PC physicians should mentor non-PC physicians on opioid use for individuals with life-limiting illnesses. Further, the importance of identifying whether a patient has OUD does not depend on a patient’s diagnosis or prognosis. Management of a patient’s OUD does not depend on their diagnosis. The importance of identifying a caregiver’s OUD also does not depend on the patient’s prognosis.
Domain 2: Healthcare institutions, PC training and clinical programs
Domain 2 focused on measures that healthcare institutions, PC training programmes and PC clinical programmes can implement to promote opioid safety. The panellists developed a total of 23 recommendations, and 6 were deemed high priority by CSPCP (online supplemental table , #13–#35). The high-priority recommendations were as follows: Healthcare institutions should collect data about opioid-related overdoses of patients receiving PC, and provide access to pharmacological OUD treatments (eg, methadone, buprenorphine-naloxone). PC training programmes should provide mandatory education about specific opioid safety topics—the most important being urine drug tests (UDTs). Further, PC clinical programmes are highly recommended to have access to addiction medicine, psychiatry and pain medicine for joint management of patients at high risk of AMTB, OUD and opioid-related overdose.
Domain 3: Patient and caregiver assessments
Domain 3 focused on patients and caregiver assessments for opioid-related harms. The panellists developed a total of 54 recommendations, and 7 were deemed high priority by CSPCP (online supplemental table #36–#89). The high-priority recommendations focused on the patient assessments (not caregivers) and were as follows: Before receiving opioid prescriptions, every patient with a life-limiting illness should receive assessments that include asking about their caregiver’s substance use history. Ten actions were identified by the panellists as AMTB in individuals with life-limiting illnesses: theft or borrowing of opioids, and route altercation of prescribed opioid are the most important AMTBs that PC clinicians should be aware of. Additionally, PC physicians should know that histories of post-traumatic stress and sexual abuse are two of the identified risk factors for AMTB (table 2). The CAGE questionnaire, Opioid Risk Tool and UDT are recommended tools that can be used to identify patients with life-limiting illnesses who are at high risk of AMTB or OUD. Research to determine which PC patients should have UDT and at what frequency are high priority.
The panellists recommend using clinical assessments, rather than specific tools or tests, to identify patients with life-limiting illnesses who have OUD. Approximately half of the panellists (n=12, 52%) reported using the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) OUD criteria. However, evaluation of use of the DSM-5 OUD criteria and screening tools (eg, ORT) to identify people with life-threatening illnesses who have OUD and/or are at high risk of opioid-related overdose are high-priority research areas. In the interim, the panellists identified a summary of items that can be used to identify patients with life-limiting illnesses who are at high risk of opioid-related overdose (table 2). Notably, PC physicians should be aware that one of the risk factors for opioid-related overdose is when a patient receives opioid prescriptions from two or more physicians.
Domain 4: Clinician opioid prescribing practices
Domain 4 focused on PC clinician prescribing practices that can prevent and manage opioid-related harms. The panellists developed a total of eight recommendations, and five were deemed high priority by CSPCP (online supplemental table #90–#97). The high-priority recommendations were as follows: Physicians should have access to regional prescription monitoring programmes to track previously dispensed prescriptions. If a patient’s primary prescriber for their opioids will be away, covering clinicians should have access to detailed pain management plans and documentation. Patients who are at high risk of AMTB, OUD and/or opioid-related overdose should receive daily to weekly dispensing of their opioids; and, for patients with active AMTB, OUD and/or history of opioid-related overdose, joint management with addiction medicine specialists should be considered. All healthcare facilities that provide PC services are recommended to have access to addiction medicine.
Domain 5: Clinician opioid monitoring practices
Domain 5 focused on practices that can be implemented by PC clinicians to monitor for opioid-related harms. The panellists developed a total of 10 recommendations, and 3 were deemed as high priority by CSPCP (online supplemental table #98–#107). The high-priority recommendations were as follows: Patients receiving PC who are at high risk or have active AMTB, OUD and opioid-related overdose are strongly recommended to be assessed more frequently than low-risk individuals. A high-priority research area is determining how often these high-risk individuals should be monitored. Regarding assessments, PC physicians are recommended to assess for and document the 4 As of universal precautions after initiating or adjusting opioids (Analgesia, Activity level, Adverse effects, AMTB)32 and adherence to instructions. Patients’ support networks should be involved to ensure adherence to the opioid prescriptions. Pill counts by nurses were recommended for patients at home and clinics; and determining which patients should receive pill counts was deemed to be a high-priority research topic.
Domain 6: Patient and caregiver education
Domain 6 focused on the content and delivery of opioid safety-related education to patients with life-limiting illnesses and their caregivers. The panellists developed a total of 23 recommendations, and 16 were deemed high priority by CSPCP (online supplemental table #108–#130). The high-priority recommendations were as follows: All patients with life-limiting illnesses who receive prescription opioids should receive education about seven topics: differentiating between physical dependence and OUD, chemical coping with opioids, opioid-related overdose signs and symptoms, safe disposal of opioids, opioid withdrawal symptoms, and driving/operating machinery. It was highly recommended that patients receive this opioid safety education through discussions with their prescriber but formal education sessions and consultations with pharmacists could be considered.
Regarding caregiver education, the high-priority topics are differentiating between physical dependence and OUDs, indications for opioid use, opioid adverse effects, opioid-related overdose signs and symptoms, and safe storage and disposal of opioids. Caregivers are strongly recommended to receive instructions (written and verbal) to return unused medications to pharmacies.
Discussion
Through a Delphi process, USA and Canadian PC, pain and addiction medicine experts tailored knowledge, strategies and tools originally developed in pain and addiction medicine to formulate 130 opioid safety recommendations for PC. In addition to reviewing these recommendations, the CSPCP reviewed 59 topics that did not achieve consensus in the study. In total, CSPCP identified 43 high-priority recommendations and 8 high-priority research topics.
These consensus recommendations are a necessary paradigm shift from the long-held views that OUD is rare among patients receiving PC.33 While PC originally focused on end-of-life care for patients with cancer, PC is now increasingly integrated early into the care of people with advanced cancers and life-threatening non-cancer illnesses.34–36 Consequently, some patients with life-limiting illnesses are being prescribed long-term, high-dose opioid therapy for symptom management, which likely increases risk of opioid-related harms.37 There is indisputable evidence in chronic non-cancer pain studies that the likelihood of OUD, opioid-related overdose and death increases as the durations and doses of prescription opioids increase.38 39 Additionally, as patients with life-limiting illnesses approach the end of their lives, they often require multiple different and increasing doses of opioids.40 Approximately 30% of patients with cancer receive more than one opioid prescription in the last 3 months of their lives41 and mean opioid doses at the end of life reportedly can be as high as 659 mg morphine equivalent daily dose in the last week of life.42 These large quantities of opioids can accumulate in households and be used for non-medical purposes, be diverted and/or can contribute to deaths.
Given the limited high-quality evidence about opioid safety in PC, CSPCP identified eight high-priority research topics. Two of the high-priority topics are about UDT, which are available as point-of-care immunoassays or laboratory-processed chromatography/mass spectroscopy tests.43 These non-invasive tests can be used to monitor prescription opioid therapy compliance and detect non-prescribed and illegal drug use. However, widespread adoption of UDT is likely limited by their availability and cost, clinician knowledge about UDT result interpretation, and negative association with use in criminal situations.44 45 Further research is highly recommended to determine which patients receiving PC should have UDT and at what frequency, especially in outpatient PC clinics. The other identified high-priority research areas are about use of pill counts and use of screening tools and DSM-5 OUD criteria to identify patients with life-limiting illnesses who have OUD and are at a high risk of opioid-related overdose. Currently there are no studies that have evaluated the efficacy and accuracy of these tools. Validation studies are urgently needed before these tools are adopted widely in PC practice.
Our study has several limitations. First, while we had a rigorous process for identifying qualified experts, only 23 of 49 invited experts agreed to participate, introducing the possibility of a biased sample. Second, there was significant heterogeneity in practice settings due to variable access and availability of resources, and uniform implementation of certain recommendations may not be possible. Finally, there are many recommendations, which introduces some cognitive burden on potential users. As this was the first study of its kind, our goal was to be as comprehensive as possible and to provide a foundation for further research and practice. The CSPCP review helped address this limitation by identifying high-priority recommendations and research topics.
These expert consensus recommendations, endorsed and reviewed by the CSPCP, provide guidance in an area of ambiguity, and inform clinical practice and future research to generate further evidence. As the COVID-19 pandemic accelerates the opioid crisis in the USA and Canada, many of these recommendations can be immediately adopted to reduce opioid-related harms.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information
Ethics statements
Patient consent for publication
Ethics approval
Research ethics approval was obtained from the University Health Network Coordinated Approval Process for Clinical Research (Study ID 18–5157).
Acknowledgments
The authors thank the experts who participated as panellists and steering committee members who helped develop these recommendations. As well, the authors thank the Canadian Society of Palliative Care Physicians for their review and endorsement of this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JelauPC, @drhaclarke, @adfurlan
Contributors All authors contributed to the conception or design of the work. JL and PM drafted the work, and all authors revised it critically for important intellectual content. All authors approved the final version and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This research was funded by the Global Institute of Psychosocial Palliative and End-of-life Care (GIPPEC) Research Collaboration Grant and Temmy Latner Centre for Palliative Care.
Competing interests AF developed the Opioid Manager app that is available for sale on iTunes. This app is owned by University Health Network. AF does not receive any profits from the sales of this app.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.