Article Text

Abstract
Objectives To evaluate the impact of provision and timing of palliative care (PC) on potentially inappropriate end-of-life care to patients with cancer in a mixed generalist—specialist PC model.
Method A retrospective population-based observational study using a national administrative health insurance database. All 43 067 adults in the Netherlands, who were diagnosed with or treated for cancer during the year preceding their death in 2017, were included. Main exposure was either generalist or specialist PC initiated >30 days before death (n=16 967). Outcomes were measured over the last 30 days of life, using quality indicators for potentially inappropriate end-of-life care.
Results In total, 14 504 patients (34%) experienced potentially inappropriate end-of-life care; 2732 were provided with PC >30 days before death (exposure group) and 11 772 received no PC or ≤30 days before death (non-exposure group) (16% vs 45%, p<0.001). Most patients received generalist PC (88%). Patients provided with PC >30 days before death were 5 times less likely to experience potentially inappropriate end-of-life care (adjusted OR (AOR) 0.20; (95% CI 0.15 to 0.26)) than those with no PC or PC in the last 30 days. Both early (>90 days) and late (>30 and≤90 days) PC initiation had lower odds for potentially inappropriate end-of-life care (AOR 0.23 and 0.19, respectively).
Conclusion Timely access to PC in a mixed generalist—specialist PC model significantly decreases the likelihood of potentially inappropriate end-of-life care for patients with cancer. Generalist PC can play a substantial role.
- end of life care
- cancer
- quality of life
- supportive care
- clinical decisions
Data availability statement
Data are available upon reasonable request. The data set from this study is held securely in coded form at Vektis Business Intelligence Center for Healthcare. While data sharing agreements prohibit Vektis from making data sets publicly available, access may be granted to those who meet prespecified criteria for confidential access. The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the program may rely upon coding templates and macros that are unique to Vektis.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
In high-income countries, over the past decade, there has been a growing concern for patients with life-threatening illnesses such as cancer, that life-prolonging medical treatments often prevail over comfort-oriented care near the end of life.1 2 Thus, medical treatments which are justifiable for patients with a similar diagnosis and good prognosis can turn into unwanted or inappropriate interventions near the end of life, where benefits of treatment no longer outweigh the possible negative effects of continuing treatment.3 Potentially inappropriate end-of-life care not only has a negative impact on a patient’s quality of care at the end of life,4 5 but also raises economic and ethical concerns, since resources are spent on interventions providing little benefit and even possible harm, rather than on care which could be more appropriate for the patient at that stage, such as comfort care or palliative care.6 Palliative care aims to improve the quality of life of patients with a life-threatening illness or frailty through early identification, careful assessment and treatment of symptoms of a physical, psychosocial and spiritual nature, effective patient–clinician communication, facilitation of complex decision making and advance care planning.7 8 Over recent years, a growing body of evidence has accumulated supporting that integration of standard oncology care with specialist palliative care is associated with improved quality of life, symptom burden, patient and caregiver satisfaction, healthcare utilisation and possibly survival for patients with advanced cancer.9–11
One of the challenges for quality improvement concerning care for patients with a life-threatening condition is to measure quality of care quickly and efficiently with as little burden to patients and their caregivers as possible. To address this concern, Earle et al previously identified a set of indicators, that can be obtained from administrative data sources, regarding potential overuse of chemotherapy, underuse of hospice services and frequency of emergency room (ER) visits, hospitalisations and intensive care unit admissions near the end of life.12 13 Applying these indicators of potentially inappropriate end-of-life care to administrative data has demonstrated a positive impact of specialist palliative care on potentially aggressive interventions in the last month of life for patients with advanced cancer.14–16 In the Netherlands however, all healthcare professionals provide generalist palliative care as part of their basic medical skills and competencies. To that end national standards and guidelines are available, although palliative care training is neither integrated nor required in healthcare education yet. There is a community structure of family practitioners and nurses who provide home care, and most primary home care teams and nursing homes provide end-of-life care. If needed, palliative care specialists are asked to provide extra support and share their expertise. As such, a multidisciplinary specialist palliative care team is available in every hospital that provides cancer care. Standards for referral or recommendations for the ratio of specialist—generalist palliative care workforce or for continuity in the delivery of palliative care have not been developed yet.17 18 The aim of this study is to investigate the association between palliative care and potentially inappropriate end-of-life care for patients with cancer in a healthcare system with a mixed generalist and specialist palliative care model.18 19
Methods
Study design
We conducted a retrospective nationwide population-based observational study using administrative data for healthcare utilisation.
Data source
Data were derived from a population-level administrative database held by Vektis.20 Due to the legal obligation for all people living or working in the Netherlands to have health insurance, this database represents around 99% of approximately 17 million medically insured people in the Netherlands in 2017. Within Vektis, encrypted health card numbers were used to combine patient-level information across several health administrative databases that contain routinely collected full health insurance data from primary, secondary and tertiary care settings.
Study setting and participants
The study was conducted for all decedents who were registered with a Dutch health insurance provider at time of death in 2017. We included all those who were >18 years old and whose record showed specific national Diagnosis-Treatment Combination codes indicating diagnosis or treatment for solid tumours in the year preceding death (online supplemental table 1).
Supplemental material
Data on provision, timing, continuity and level of palliative care were collected over a period of 1 year preceding the date of death. Data collection on potentially inappropriate end-of-life care was limited to the last 30 days of life. Overall data collection covered a period between 1 January 2016 and 31 December 2017.
Patient and public involvement
We collected data on an aggregated level with quality indicators that have been accepted as benchmarks to assess the quality of end-of-life care.21 The patient’s perspective was incorporated in the definition of these quality indicators. In our study, as we used the predefined quality indicators, patients were not involved in defining the research question or the outcome measures, nor were they involved in developing plans for design or implementation of the study. No patients were asked to advise on interpretation or writing up of results. The results of this study will be broadly disseminated, that is, through patient organisations and digital patient communities.
Exposure group
The main exposure was provision of palliative care. This could be either generalist or specialist palliative care. First initiation of palliative care was assessed across all care settings by use of specific national healthcare codes required for reimbursement of palliative care. Healthcare codes were considered to represent initiation of palliative care when they contained the words ‘palliative’, ‘palliative/supportive’, ‘hospice’, when they referred to advance care planning or when a life expectancy of less than 3 months was an explicit requirement for reimbursement of a specific healthcare code (online supplemental table 2). This was done for hospital-based, home-based, hospice-based and nursing home-based care settings and resulted in 200 specified codes and 11 grouped codes. Healthcare codes for disease directed treatments (eg, palliative chemotherapy or radiotherapy in oncology setting) were considered part of usual care for the majority of patients, where the other dimensions of palliative care (ie, psychological, social and existential) are not necessarily addressed. Therefore, healthcare codes referring to these treatments were excluded from the palliative care exposure group.
To compose the exposure group, we distinguished between palliative care initiated >30 days before death, palliative care initiated ≤30 days before death and no palliative care at all. Patients scoring at least one healthcare code for palliative care initiated >30 days before death, were assigned to the exposure group.
Non-exposure group
Patients not scoring healthcare codes for palliative care or for whom palliative care was initiated ≤30 days before death were assigned to the non-exposure group.
Timing and continuity of palliative care
To evaluate the influence of timing of palliative care on potentially inappropriate end-of-life care, we stratified first initiation of palliative care by early, late and very late palliative care. In accordance with previous studies, we defined early palliative care as initiated >90 days before death,14 15 late palliative care as initiated ≤90 and>30 days before death and very late palliative care as initiated ≤30 days before death. To evaluate continuity of palliative care after initiation, we assessed the number of palliative care registrations per patient for each timeframe. We focused on assessing impact of early and late palliative care on potentially inappropriate end-of-life care and excluded very late palliative care from the exposure group. This was done to avoid confounding issues due to overlap with the outcome period (ie, it would be unclear if palliative care was started prior to or after use of potentially inappropriate care within the last 30 days of life).
Level of palliative care
To assess the proportion of generalist and specialist palliative care, we stratified the specific national healthcare codes required for reimbursement of palliative care by generalist palliative care codes and specialist palliative care codes (online supplemental table 2). Generalist palliative care reimbursement can be claimed for palliative care provided by (healthcare organisations employing) healthcare professionals with basic training in palliative care, including but not limited to family physicians, general practitioners, medical specialists (eg, oncologists, internists, geriatricians, anesthesiologists, etc), nurse practitioners and nurses across all care settings.17 18 Stratification for generalist palliative care resulted in seven grouped healthcare codes.
Specialist palliative care reimbursement can only be claimed for care provided by individual healthcare professionals with specialty training in palliative care and by healthcare organisations employing a multidisciplinary team of palliative care specialists. For specialist palliative care four grouped healthcare codes were used (online supplemental table 2).17 18
Patients who were provided with only generalist palliative care were allocated to the generalist palliative care group. Patients provided with at least specialist palliative care were allocated to the specialist palliative care group. Specialist palliative care prevailed over generalist palliative care for the allocation to the groups. Therefore, patients in the specialist palliative care group were provided either with specialist palliative care alone, or with both generalist and specialist palliative care.
Outcomes
We selected population-based quality indicators for end-of-life care based on a body of literature concerning development, validation and benchmarking of these indicators.12 13 22 23 Six population-based quality indicators measuring potentially inappropriate or aggressive end-of-life care were used to evaluate quality of care in the last 30 days of life: provision of chemotherapy, frequency of ER visits (≥2) and hospital admissions (≥2), length of hospitalisations (>14 days), intensive care unit admissions (≥1) and hospital death. Patients scoring any one of these items were defined as receiving potentially inappropriate end-of-life care.12 14 24 As each patient could score multiple indicators, we calculated the mean composite score by adding up the numbers of patients scored per quality indicator and dividing this sum by the number of patients receiving potentially inappropriateend-of-life care.24 This reflects the mean number of indicators per patient.
Statistical analysis
Descriptive statistics were used to assess provision, timing and continuity of palliative care by itself and in relation to receiving potentially inappropriate end-of-life care. Summary statistics are presented, differences were tested using χ2 test. Multivariable logistic regression was used and adjusted ORs and corresponding 95% CIs were computed to assess the impact of palliative care as well as the impact of early and late palliative care on the likelihood of receiving potentially inappropriate end-of-life care. In the model, we adjusted for age, sex and cancer diagnosis (type and number of (ie, multiple) diagnoses). A two-tailed p value less than 0.05 was considered statistically significant. All analyses were conducted in R (V.3.4.4).25
Results
Overall, 43 067 adults were diagnosed with or treated for cancer in the year preceding their death in 2017 and palliative care was initiated for 32 768 (76%). For 16 967 patients (39%) palliative care was provided >30 days before death (exposure group). This was initiated early for 8882 patients (20%) and late for 8085 patients (19%). For 15 801 patients (37%) palliative care was provided ≤30 days before death and 10 299 patients (24%) did not receive palliative care at all (non-exposure group). Characteristics regarding age, sex and cancer diagnosis were similar for both groups (table 1).
Cohort characteristics
During the last 30 days of life, 14 504 patients (34%) experienced potentially inappropriate end-of-life care; 2732 patients in the exposure group and 11 772 patients in the non-exposure group (16% vs 45%, p<0.001). All quality indicators rated lower for patients in the exposure group; ≥2 ER visits (6% vs 16%, p<0.001), ≥2 hospital admissions (4% vs 12%, p<0.001), >14 hospital days (3% vs 11%, p<0.001), chemotherapy (3% vs 6%, p<0.001), intensive care unit (ICU) admission (1% vs 9%, p<0.001) and hospital death (8% vs 28%, p<0.001). However, the average number of indicators scored per patient, that is, the mean composite score was similar (1.6 vs 1.8) for both groups (table 2).
Indicators of potentially inappropriate end-of-life (EoL) care*
Timing and continuity of palliative care
On average, early palliative care was started 6.8 months before death and late palliative care 2.1 months before death. We found a small but statistically significant difference in potentially inappropriate end-of-life care between early and late start of palliative care in favour of the latter (18% vs 14%, p<0.001). More specifically in the indicators for ER visits, hospital days, ICU admission and hospital death (table 3). The median number of palliative care registrations for patients provided with early palliative care was 3 (IQR 1–6) from initiation to 3 months before death, 4 (IQR 2–9) between 3 and 1 months and 7 (IQR 4–11) in the last 30 days. For patients provided with late palliative care, the median number of palliative care registrations was 2 (IQR 1–5) between 3 and 1 months before death and 8 (IQR 5–12) in the last 30 days (table 3).
Indicators of potentially inappropriate end-of-life (EoL) care* stratified by timing of palliative care (PC)
Level of palliative care
We found the proportion of specialist palliative care in relation to generalist palliative care to be 12%, regardless of whether palliative care was provided early, late or very late (table 4). In the exposure group (n=16 967) specialist palliative care (n=2024) consisted of specialist palliative care alone in 1% of patients (n=141) and of both generalist and specialist palliative care in 11% (n=1883). The majority of patients (88%) was provided with generalist palliative care alone.
Level of palliative care (PC) stratified by timing of PC (n=32 768)
Impact of provision and timing of palliative care on the likelihood of receiving potentially inappropriate end-of-life care
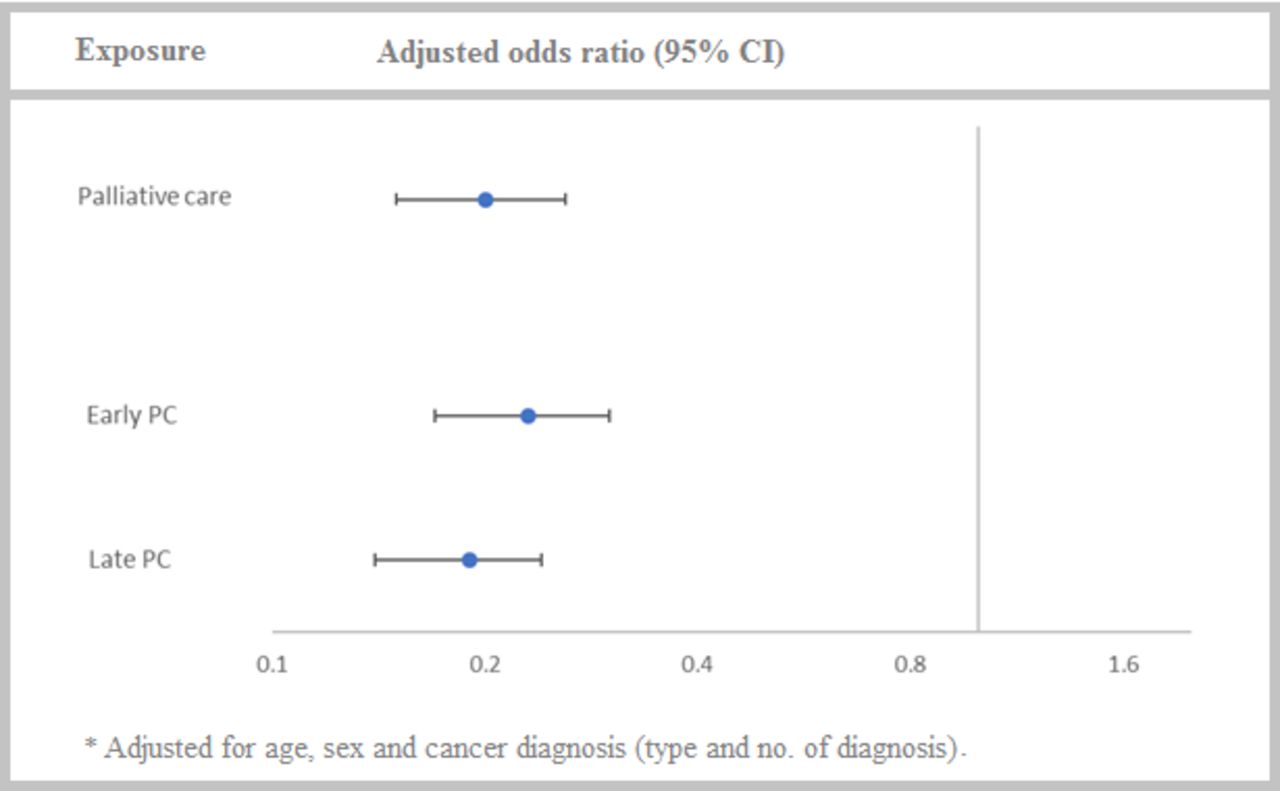
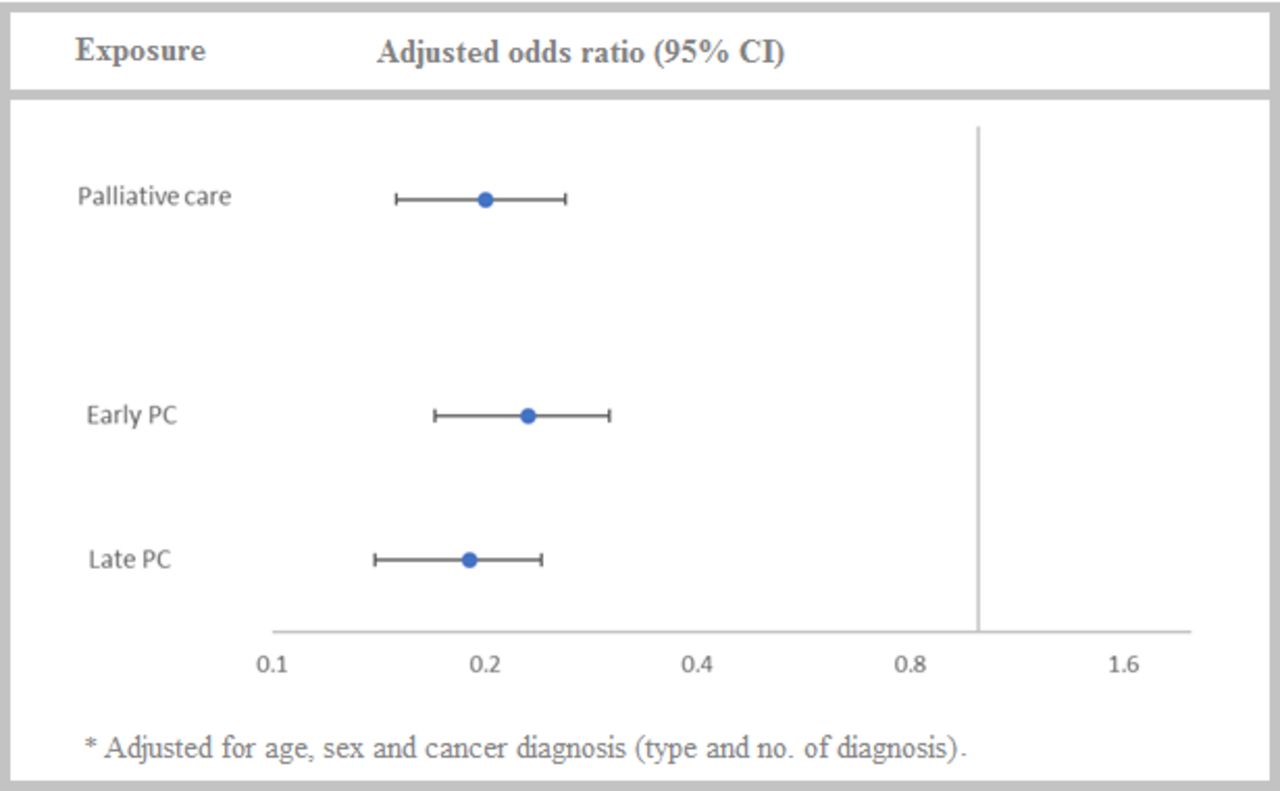
Adjusted for age, sex and type and number of cancer diagnoses, patients receiving palliative care more than 30 days before their death (exposure group) were five times less likely to experience potentially inappropriate end-of-life care (adjusted OR 0.20; 95% CI 0.15 to 0.26) than patients who received palliative care less than 30 days before their death or not at all (non-exposure group). Subanalysis of the exposure group showed lower odds for potentially inappropriate end-of-life care with late initiation of palliative care (≤90 and>30 days before death; adjusted OR 0.19; 95% CI 0.14 to 0.24) than with early initiation of palliative care (>90 days before death; adjusted OR 0.23; 95% CI 0.17 to 0.30; figure 1).
{kind=link}
Association between palliative care (PC) and potentially inappropriate end-of-life care*.
Discussion
Among 43 067 patients with cancer who died in the Netherlands in 2017, we found that more than one-third of patients experienced potentially inappropriate care in the last month of their life. Patients who received palliative care prior to the last month of their lives were five times less likely to experience potentially inappropriate care in the last month of their life than patients provided with palliative care in the last month of life or not at all. Both early and late palliative care exposure were similarly associated with lower odds for potentially inappropriate care. For most patients, palliative care consisted of generalist palliative care, regardless whether it was provided early, late or very late.
Strengths and limitations of this study
To our knowledge, this is the first nationwide population-based observational study evaluating the impact of a mixed generalist and specialist palliative care model on quality of end-of-life care for patients with cancer, provided across all care settings. Another strength of this study lies in the use of a population-level administrative database covering nearly all Dutch residents. This minimises selection bias and renders our findings generalisable for comparison to other populations of patients with cancer. However, several limitations need mentioning. First, population-based quality indicators are used on an aggregated level and cannot be used as indicators of inappropriate care for individual patients; clinical factors may justify an acute care intervention and personal preferences may differ. Hence, our strict use of the term ‘potentially inappropriate end-of-life care’ throughout the article. Second, as administrative data are not primarily captured for the purpose of quality assessment, a general limitation results from a lack of clinical information about the content of care provided. Third, our findings are based on a retrospective study design. Therefore, we could not determine whether healthcare professionals were aware of their patients being in their last months of life nor whether care took place in that context.
Comparisons with other studies
When we compare our results to previous national and international studies in high-income countries with a similar healthcare system, it shows a higher percentage of potentially inappropriate end-of-life care for patients with cancer in the Netherlands compared with Canada (34% vs 22.4%)24 and a consistently low percentage of hospital death (20% vs 29%) as well as a low percentage of chemotherapy use (5% vs 17%) in the Netherlands compared with Belgium.26 27 In contrast, we find only 12% of patients received specialist palliative care vs 47% in Belgium and 25.8% in Canada.19 27 In 2017, reimbursement for specialist palliative care in Dutch hospitals was difficult to obtain as a result of complicated administrative financial regulations. Therefore, the actual proportion of specialist palliative care provided is likely to be larger than our data suggest. However, a previous study showed a limited number of referrals to specialist palliative care teams in Dutch hospitals in 2014 (median 77 consultations per year, range 2–680).28 In relation to other countries actual underutilization of specialist palliative care services, complex registration of specialist palliative care provided, and a lack of standards for referral or the ratio of specialist—generalist palliative care workforce may contribute to the low proportion of patients receiving specialist palliative care in the Netherlands. This is currently subject of further research.
Considering that most palliative care provided in this study was generalist palliative care, this comparison of studies seems to suggest that generalist palliative care improves end-of-life care through preventing hospital death and use of chemotherapy in the last month before death. Improving access to specialist palliative care for patients with complex palliative care needs may assist in lowering the overall percentage of patients experiencing potentially inappropriate end-of-life care.
A recent systematic review of population-based quality indicators found only one previous study that established a benchmark for healthcare systems not providing overly aggressive end-of-life care.13 29 In this preferred healthcare system less than 10% of patients receive chemotherapy in the last 14 days of life, less than 4% have multiple hospitalisations or ER visits or are admitted to the ICU in the last month of life and less than 17% die in an acute care institution. Applying this benchmark to our results for the patients receiving palliative care very late or not at all leaves room for improvement for nearly all quality indicators. However, for patients who were provided with palliative care prior to their last month of life, nearly all benchmark requirements were met. These results strongly suggest a need to focus local and national policy on increasing the number of people with cancer receiving palliative care early in their disease trajectory.
Contrary to what other studies have shown,14 15 30 in this study early initiation of palliative care has a weaker association with less potentially inappropriate end-of-life care than late initiation of palliative care. In their studies, while using similar definitions for early and late palliative care, both Hui et al and Scibetta et al did not exclude palliative care provided during the outcome period (ie, last 30 days before death) from their late palliative care group. This may have reflected on the outcomes for potentially inappropriate end-of-life care in this group, thereby confounding comparison with our results. As Qureshi et al used different timeframes for the early and late exposure group in their large population-based study, we could not compare our results.
Comparing the median number of palliative care registrations between early and late provision of palliative care as presented in table 3 sheds some light on our ambivalent results. Patients provided with early palliative care have more palliative care registrations between 3 and 1 month before death than patients provided with late palliative care. This might indicate that these patients have more complex palliative care needs that potentially require more healthcare utilisation at the end of life. Still, in both early and late palliative care groups care consisted of generalist palliative care with a similarly limited proportion of specialist palliative care (12%). Comparing specialist and generalist palliative care visits around critical timepoints, specialist palliative care visits emphasised coping and prognostic awareness, whereas oncologic care focused on cancer treatment and management of medical complications.31 Early referral of patients with complex palliative care needs to specialist palliative care may well improve quality of care for these patients.32
Recent literature shows that patients with life-threatening illness or frailty continue to receive non-beneficial treatments at the end of life, leading to poor quality, high cost care in high-income countries.33 34 Despite ample evidence that specialist palliative care improves quality of life, symptom burden and quality of end-of-life care for these patients and their families,10 11 16 35 and professional organisations recommend earlier and routine co-management by palliative care specialists,1 36 37 there appears to be little improvement over the past two decades.2 24 34 With the foreseen increase in patients with palliative care needs,38 39 comes a workforce shortage in palliative care specialists and a need for all healthcare professionals to deliver generalist palliative care.17 40 41 Our data confirm that generalist palliative care can play a substantial role.41 42 Moreover, as we established as yet a limited involvement of specialist palliative care services, standards or recommendations on use of internationally expert-based referral criteria may help optimise quality of end-of-life care through timely access to specialist palliative care for patients with complex palliative care needs.11 43
Conclusion and policy implications
This study shows that initiation of palliative care prior to the last month of life significantly decreases the likelihood of potentially inappropriate end-of-life care for patients with cancer. As generalist palliative care may play a substantial role, these results imply a strong need to focus local and national policy on improving access to generalist and specialist palliative care for every patient.
Sustained investment in training of all healthcare professionals can improve timely identification of palliative care needs in the individual patient, distress caused by the disease and its impact on the person as a whole. This will lead to a larger number of patients receiving generalist palliative care earlier in their disease trajectory. Also, improving early access to specialist palliative care for patients with complex palliative care needs will lead to more prognostic awareness and better quality of end-of-life care for these patients. Recommendations on use of standardised referral criteria for specialist palliative care and funding of integrated palliative care models are needed to support these improvements. As such, these improvements to end-of-life care may have major implications for health policy. Further prospective research is needed to substantiate the findings of this retrospective study.
Data availability statement
Data are available upon reasonable request. The data set from this study is held securely in coded form at Vektis Business Intelligence Center for Healthcare. While data sharing agreements prohibit Vektis from making data sets publicly available, access may be granted to those who meet prespecified criteria for confidential access. The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the program may rely upon coding templates and macros that are unique to Vektis.
Ethics statements
Patient consent for publication
Ethics approval
According to the Central Committee on Research involving Human Subjects (CCMO), this type of study is exempt from approval of an ethics committee. This study was approved by all health insurance companies contributing data to Vektis national administrative health insurance database.
Acknowledgments
The authors wish to thank Lyanne Bakker MSc and Bart Koetzier MSc, data scientists and statistical analysts at Vektis, Business Intelligence Center for Healthcare for their contribution to the acquisition, analysis and interpretation of data and Marijke Dermois PDEng, clinical informatician at Netherlands Comprehensive Cancer Organisation for her valuable contribution to the design of the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JA had full access to all data and MB, CP, NR and HF had access to most of the data in the study. MB, CP, JA, NR and HF take responsibility as guarantors for the integrity of the data and the accuracy of the data analysis. MB, CP, NR and HF conceived and designed the study. JA collected the data. MB, CP, YL, NR and HF interpreted the data. MB, JA and HF undertook the statistical analysis. MB drafted the manuscript. All authors provided critical input to the analyses, interpreted the data and critically revised the manuscript. YL, KV, NR and HF supervised the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.