Article Text

Abstract
Introduction Healthcare professionals (HCPs) experience difficulties in timely recognising and directing palliative care (PC) needs of their patients with chronic heart failure (CHF). The aim of this study was to develop a comprehensive tool to enable HCPs in timely recognising and directing PC needs in CHF.
Methods A four-stage mixed-method study was performed. Stage 1: identification of needs and questions of patients and families; stage 2: prioritisation and refinement of the needs and questions; stage 3a: testing and online feedback on V.1; stage 3b: selecting and refining care recommendations; stage 4: testing and review of V.2. Iterative reviews followed each step in the development process to ensure a wide range of stakeholder input. In total, 16 patients, 12 family members and 54 HCPs participated.
Results A comprehensive set of 13 PC needs was identified, redefined and tested. The resulting tool, called Identification of patients with HeARt failure with PC needs (I-HARP), contains an introduction prompt with open questions to start the conversation, 13 closed screening questions with additional in-depth questions, and recommendations on actions for identified needs.
Conclusion I-HARP contains an evidence-based set of questions and palliative CHF care suggestions for HCPs in the Netherlands. The resulting tool, approved by HCPs, patients and family members, is a promising guidance for HCP to timely recognise and direct PC needs in CHF.
- heart failure
- communication
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
People with chronic heart failure (CHF) experience disabling physical symptoms such as breathlessness, fatigue, tiredness and poor appetite, frequently combined with high psychological and social distress throughout the whole progressive disease trajectory.1–3 Research shows that people with advanced CHF have the same level of palliative care (PC) needs compared with patients with cancer.4 PC in the context of CHF has positive effects on patient-centred outcomes, quality of life, documentation of care preferences and resource use.5–7
The need to deliver holistic, supportive, needs-led, person-centred care to patients with advanced CHF is internationally recognised.8 However, high levels of unmet support needs and variability in person-centred care remain. Reasons for not providing timely PC in CHF contain the unpredictable disease trajectory,9 10 the limited value of prognostication to determine PC,8 the many different disciplines which are involved in the delivery of CHF care10 11 and the lack of skills in and time for PC conversations and to determine what should be done.11–14 Moreover, patients tend to accept their symptoms and limitations instead of seeking actively help. Thereby needs remain invisible, often leading to PC not being initiated until the last days of life.15
A tool that addresses these problems could help healthcare professionals (HCPs) from different disciplines and working in different settings, in recognising and directing PC needs. Desired characteristics of such a tool were explored to recognise and direct PC needs in CHF in the Netherlands.16 Important requirements of the tool included the following aspects: usability during a real-life conversation, comprehensive and generally applicable; CHF-specific (eg, with respect to medication and treatment regimens), inclusion of PC needs of the family caregiver, inclusion of some open questions to identify unique needs and applicability in early and in late CHF disease stage.17
A recent review showed that the available international tools were not fully appropriate for the Dutch setting based on the identified desired characteristics of a tool in this country.16 18 The tools were developed for a specific discipline or revealed to be too complex to apply, were focused on case finding instead of identification of PC needs or were not CHF-specific. The aim of this study was to develop the content of the new tool ‘Identification of patients with HeARt failure with PC needs (I-HARP)’ for HCPs working in primary care, secondary care and nursing homes. This paper outlines the results of a theory and practice-based development process for this tool.
Methods
Design and setting
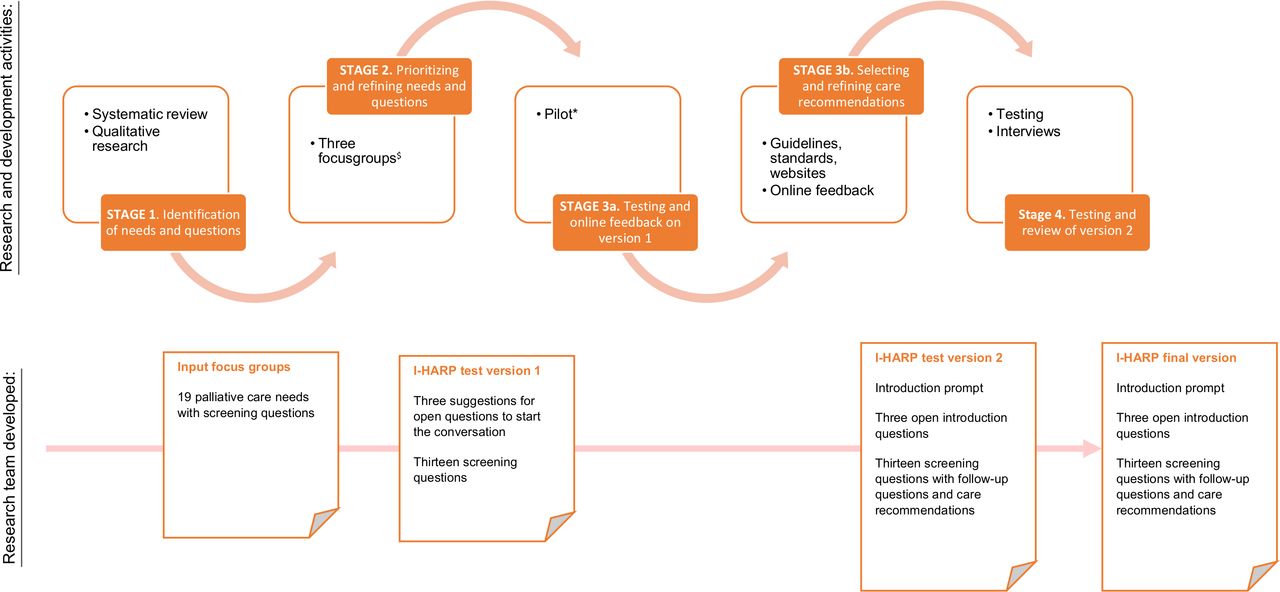
An iterative mixed-method and participatory research design was used for the content development of I-HARP (November 2018–March 2020).19–21 The development stages of the research process are presented in figure 1.
{kind=link}
Development process of the content of the Identification of patients with HeARt failure with PC needs (I-HARP). Research and development activities were performed in four stages. The research team developed the input for the focus groups, the I-HARP test versions 1 and 2 and the I-HARP final version. Research team: implementation scientist (SA), a specialist in elderly care medicine and PC (DJAJ), a specialist in PC (MvdB-E) and a specialised heart failure nurse (JB). $=Three focus groups: to prioritise needs with respect to relevance regarding advanced heart failure and palliative care, and to refine the tool’s content with respect to the comprehensiveness (whether all key items were included) and comprehensibility (whether the content was clear and appropriately worded).26 *To help healthcare professionals with finding patients with palliative care needs, we extended the recruitment period and we adapted our communication to healthcare professionals by adding explanations about PC in the context of advanced chronic heart failure using the palliative care approach in CHF as defined by the European Association for Palliative Care (EAPC).8 CHF, chronic heart failure; PC, palliative care.
The methods involved four different stages:
1. Defining the needs of patients and family members and questions based on existing tools and qualitative research.
2. Prioritisation and refinement of the needs and questions.
3a. Testing and online feedback on V.1.
3b. Selecting and refining care recommendations.
4. Testing and review of V.2.
Stage 1: identification of needs and questions
The first stage of the development process was to identify, categorise and define PC needs in CHF and to extract related questions from existing tools and qualitative research.
Stage 1a: systematic review
The methodology for the identification of the tools was described elsewhere.18 Besides existing tools related to CHF, the Support Needs Approach for Patients needs assessment tool to identify palliative support needs in advanced chronic obstructive pulmonary disease (COPD) was used to identify promising questions.22
Stage 1b: qualitative research
Qualitative research was performed to identify desired characteristics of a tool to assess PC needs in CHF16 and to identify descriptions of PC needs in CHF. The suggested questions were used in the current study. As previously reported,16 this dataset contained focus group and individual interviews with HCPs caring for patients with CHF and individual interviews with patients with CHF, family members and bereaved family members. Patients, family members and bereaved family members were recruited in one general practice, two academic hospitals and two nursing homes. HCPs were recruited in two hospitals, six general practices and two nursing homes. In brief, included patients were diagnosed with advanced CHF (New York Heart Association (NYHA) class III or IV). Family members of patients with CHF NYHA class III or IV were eligible. Bereaved family members were included between six and 12 months after decease of the patient. Respondents were recruited until data saturation level was reached.23 Qualitative data were analysed using Nvivo V.12 PRO.
The research team (implementation scientist (SA), a specialist in elderly care medicine and PC (DJAJ), a specialist in PC (MvdB-E) and a specialised heart failure nurse (JB)) categorised the identified PC domains, needs and questions from the tools and the qualitative research in the palliative domains.24 25 An inductive approach was used to categorise other and possible heart failure-specific PC domains, needs and questions. Similar items were merged and renamed into a single item.
Stage 2: prioritisation and refinement of the needs and questions
The second stage of the development process was to prioritise the content with respect to relevance, and to refine the tool’s content with respect to the comprehensiveness (whether all key items were included) and comprehensibility (whether the content was clear and appropriately worded).26 Three parallel focus groups with HCPs, patients and family caregivers were organised during a 3-hour meeting.
Recruitment of focus group participants. HCPs were recruited by members of the research team, using purposive sampling to achieve diversity in terms of disciplines, setting and cultural background in three groups with a maximum of six HCPs per group. HCPs were recruited in four hospitals, four general practices and two nursing homes. HCPs were eligible if they were HCPs caring for patients with CHF. HCPs who participated in stage 1a were approached as well. Patients and family members were recruited via staff of two hospitals and two general practices using the same inclusion criteria as in stage 1b. Patients and family members were informed about the study by their HCP and if they agreed, they were contacted by a member of the research team and they received written information.
Data collection: The session started with an introduction providing background information about PC in CHF, the current project and the aims of the session (DJAJ). Thereafter, respondents were divided in three focus groups. For sake of the acceptability of I-HARP, we opted for a short set of relevant screening items. The aim of the focus groups was to discuss the 19 PC needs and to select the ten most relevant ones, to discuss suggestions for additional relevant PC needs (comprehensiveness) and to select or redefine questions (comprehensibility) per focus group.26 Three project members of the research team (YE, JB and LB) joined the three focus groups to observe the research process and to take field notes. One researcher (SA) applied topical steering and took field notes.27
Data analysis: Items were included in I-HARP test V.1 if they were at least twice selected in the focus groups. Also, based on the desired tool characteristics (that the tool had to increase the awareness of and knowledge about PC needs), all four PC domains and attention for the caregiver needed to be included.16
Stage 3a: testing and online feedback on V.1
The third stage of the development process was to evaluate the content and acceptability of I-HARP test V.1 during a regular face-to-face consultation.26 28
Recruitment of participants: HCPs were asked via the research team, among them the HCPs who were involved in stage 1a and stage 2. Purposeful sampling was used to include two registered nurses, two cardiologists, two general practitioners, two general practice-based nurse specialists, two elderly care physicians and two heart failure nurse specialists. HCPs were recruited in four hospitals, twelve general practices and eight nursing homes.
Data collection: The HCPs were asked to use all I-HARP screening questions (PDF-file) during a regular face-to-face consultation. After having tested the I-HARP screening questions in practice, the respondents filled in a web-based questionnaire (Qualtrics XM) to share their experiences and to make suggestions for I-HARP improvements. The respondents were invited to rate and to provide comments with respect to the relevance, comprehensiveness (whether all key items were included) and comprehensibility (whether the content was clear and appropriately worded).26 Value definition consisted of statements, all with five answering categories (totally disagree, disagree, neutral, agree and totally agree). To increase the chance for successful implementation of the tool in the Netherlands, the acceptability of I-HARP was evaluated. Acceptability was defined as the perception among I-HARP’s future users that an innovation is agreeable or satisfactory.29 With respect to acceptability of I-HARP, the respondents were asked to report the time needed to complete the I-HARP screening questions, to rate the level of approval of the content and of the intention to use I-HARP in practice using the same five answering categories as described above. A shorter feedback questionnaire was sent to the same HCPs who could not test I-HARP in practice to make suggestions for I-HARP improvements. This questionnaire was shared by the research team via purposeful sampling to other HCPs.
Data analysis: Quantitative data were analysed through descriptive analyses via Qualtrics XM. Qualitative and quantitative data were summarised and clustered (SA) based on relevance, comprehensiveness, comprehensibility and acceptability using Excel 2016 Pro Plus. The research team discussed the results and developed I-HARP test V.2. An expert of the Dutch Centre of Expertise on Health Disparities (Pharos) checked the comprehensibility of the language used in I-HARP test V.2.
Stage 3b: selecting and refining care recommendations
Data collection: Based on the desired tool characteristics to guide proactively addressing PC needs and when to consult other HCPs,16 the research team developed recommendations on actions for HCP on item level. The content was developed using clinical PC guidelines and national standards and references. This concept was shared by email with all HCPs who had been involved in a previous development step (including step 3a) of I-HARP and with experts of the I-HARP project team (YE, LB, H-PB-LR, JMGAS, JMCM and JB). Respondents were asked to evaluate and comment on the comprehensiveness and relevance of the recommendations on item level.
Data analysis: The research team discussed the comments from the respondents and refined the care recommendations on item level. The care recommendations were integrated in I-HARP test V.2.
Stage 4: testing and review of V.2
The fourth stage of the development process was to test the content and acceptability of I-HARP test V.2.
Data collection: The same recruitment goals as in stage 3a were used and the same HCPs as in stage 3a were approached to take part in the pilot of I-HARP test V.2. After having tested the I-HARP screening questions in practice, the respondents filled in a web-based questionnaire to share their experiences and to make suggestions for I-HARP improvements (see stage 3a). All patients and family members who participated in stage 2 were asked to review this version, in particular its comprehensiveness and comprehensibility. The content was reviewed using a think-aloud method by telephone while field notes were taken (LB) or via email.30 A member check was performed by submitting an interview summary to each respondent for approval. The concept of the final I-HARP version was shared with experts of the I-HARP project team (YE, LB, H-PB-LR, JMGAS, JMCM and JB) to review.
Data analysis: Quantitative and qualitative data were summarised and clustered based on relevance, comprehensiveness and comprehensibility of the content and acceptability of using I-HARP. These data were discussed by the research team.
Results
Respondent characteristics of all four research stages are presented in table 1. Respectively, 22% (n=12) of the HCPs and 37% (n=10) of the patients and family members was male. Mean age of the patients was 73 (51–89) years and mean age of the family members was 67 (43–86) years. From the HCPs, 17.5% were in the age group of 21–30 years, 15.8% were in the age group of 31–40 years, 24.6% were in the age group of 41–50 years, 28.1% were in the age group of 51–60 years and 14.0% were in the age group of 61–70 years.
Characteristics of respondents participating in individual interviews, focus groups, testing and evaluation round
Stage 1: identification of needs and questions
As previously reported,16 three focus group interviews with HCPs caring for patients with CHF, eight individual qualitative interviews with HCPs caring for patients with CHF and 23 individual interviews with patients with CHF, family members and bereaved family members were done.
Online supplemental file 1 shows the 15 domains and 50 PC needs and how they were identified. After categorisation, 13 domains and nineteen PC needs with screening questions were developed.
Supplemental material
Stage 2: prioritisation and refinement of the needs and questions
Out of the 19 PC items identified in stage 1, 13 PC needs in CHF were selected based on relevance and comprehensiveness (online supplemental file 2). Respondents of focus group three mentioned that open questions such as ‘What is this patient most concerned about?’ or ‘What does the patient still enjoy?’ were considered key questions and may reveal a lot of information. As a result, open introduction questions were added to I-HARP test V.1 (online supplemental file 3). Respondents in all groups mentioned that PC was associated with terminal care. To facilitate the HCPs in recognising needs earlier in the course of CHF, the research team decided not to use the word ‘palliative’ in the screening questions and all screening questions were reformulated into closed questions. With respect to acceptability, one cardiologist mentioned that asking the I-HARP questions may take more time than ten minutes. Further questioning is often necessary.
Supplemental material
Supplemental material
Stage 3a: testing and online feedback on V.1
Eight and 10 of the 14 respondents perceived the items about financial and cultural issues, respectively, as relevant (online supplemental file 4). The research team decided not to exclude financial and cultural issues from I-HARP as1 these items were selected as relevant content for I-HARP in stage 2 and as2 patients and family caregivers mentioned these elements to be relevant in previous research.16 Respondents made suggestions for textual improvements on item level and identified two areas for improvement1: more specific attention for ACP in the context of advanced CHF and2 the order of the items.
Supplemental material
The mean time needed to complete the I-HARP screening questions was 34 min (range: 10 min by the general practice-based nurse specialist and family physician; and 60 min by the elderly care physician). Eleven HCPs (79%) approved the content (agree and completely agree). Nine HCPs (64%) were intended to use I-HARP test V.1 in practice (agree and completely agree) and four HCPs (29%) provided a neutral answer. One HCP, an elderly care physician, was not intended to use I-HARP test V.1. Reasons for not using the introduction and screening questions was the perception of already knowing the patient’s answers or the perception of already asking these questions in practice.
Stage 3b: Selecting and refining care recommendations
Respondents reviewed the care recommendations and mentioned that they needed more concrete questions and guidance on item level to make I-HARP more usable during a consultation.
In some of the questions I miss concrete examples that can be discussed with the patient and caregiver. (Cardiologist)
I think example prompts are highly desirable. This is because formulating the questions is sometimes very difficult (Heart failure nurse specialist)
As a result of stage 3a and 3b, the order of the items was changed, and follow-up questions and care recommendations were added to I-HARP test V.2 (online supplemental file 5).
Supplemental material
Stage 4: testing and review of V.2
Seventy-seven HCPs were asked to test I-HARP V.2 and 14 agreed to participate. Due to the impact of the COVID-19 pandemic,31 testing in practice became impossible and the test phase was terminated on 20 March. One week before, HCPs received a request and last call to participate if possible and the announcement of the termination of the pilot 1 week later. HCPs had the option to fill in a short online evaluation or to participate in a telephone interview with the researcher (SA) to think-aloud about I-HARP test V.2.
Experts, HCPs, patients and family members gave some suggestions for textual improvements, additional in-depth questions and care recommendations. HCPs agreed to the content and all were intended to use I-HARP in practice. All HCPs mentioned that I-HARP may be too extensive for one face-to-face consultation. Reasons they mentioned were the limited consultation time, the possible limited energy of the patient and it may have too many items to reflect on as a patient. HCPs recommended to spread the questions over multiple consultations or moments.
The patients and family members mentioned that the open questions to start the conversation, the screening question per I-HARP item and the follow-up question per I-HARP item were clear and non-confronting formulated. One patient suggested to add the term ‘togetherness’ to the introduction prompt for HCPs to emphasise the participatory role of the patient during the conversation. Another patient mentioned the importance to inform and stimulate the patient to bring a family caregiver to the consultation.
Based on this feedback, the final I-HARP version was developed by the research team (online supplemental file 6).
Supplemental material
Discussion
This paper reports the development process of I-HARP, a tool for HCPs to facilitate in timely recognising and directing PC needs of patients with advanced CHF for use in the hospital setting, general practice and nursing homes in the Netherlands. The findings show that I-HARP has content validity for patients within this population.
Strengths of I-HARP
I-HARP is the first CHF specific tool which is generally applicable and accessible to facilitate HCPs from different disciplines. I-HARP is developed based on a needs assessment of desired characteristics of an implementable tool and iterative development stages with patients with advanced CHF, family members and all relevant HCPs.19 This needs-based and user-centred development may increase the chance for adoption in practice.29 The use of multiple data sources and iterative feedback loops provided data on the content and refinements of the tool. The content of the tool elaborates on existing content and criterion validation research of tools in the context of PC and advanced CHF and on the lessons learnt from practice.18 Moreover, the care recommendations are partly based on the Dutch multidisciplinary guideline ‘PC for patients with heart failure’.32
Challenges expected regarding implementation of I-HARP
During the development process it became clear that the acceptability of I-HARP may be hindered due to time limitations. More guidance and education for HCPs about how to use I-HARP may facilitate effective and efficient application.18 The time needed to complete I-HARP may vary due to the different roles of the HCPs and the different organisational processes and regional collaboration. Patients with CHF and family members prefer recognition of PC needs during a conversation instead of self-completing a questionnaire.16 Spreading the questions over multiple consultations or recognising PC needs before consultation may be preferred to overcome time limitations. Asking some I-HARP questions before consultation may facilitate patient empowerment and the participatory role of the patients with advanced CHF while maintaining the comprehensiveness of the items.33 Patients may have more time to reflect on issues which supports the patient and HCP dialogue.34 E-health is rapidly evolving in CHF care and care is increasingly delivered close to the patients home.35 However, these methods may not be totally appropriate for all patients living with advanced CHF.
Limitations
Several limitations of the current project need to be considered. First, I-HARP was developed within the Dutch context. International and cultural differences in providing care to patients with advanced CHF may affect the applicability in other countries. Further, we tried to ensure that male and female respondents and the different disciplines relevant to PC in advanced CHF were represented. Though, male respondents, elderly care physicians and general practitioners were under-represented in this study. The aim of I-HARP is to recognise and direct PC needs and the application of I-HARP takes time. Nurses, heart failure nurse specialists and general practice-based nurse specialists have a screening and referring role in the Dutch healthcare system and they may have more time to talk with the patient than doctors have. Therefore, I-HARP may be more applicable for this target group which was sufficiently represented. In addition, HCPs may have selected patients they already knew very well and feel save to test I-HARP. Some HCPs perceived difficulties in finding appropriate patients. Comparable issues of recruiting patients with CHF in the context of PC research were described by Kane et al.36 Finally, a second testing phase of I-HARP was not possible due to the impact of the COVID-19 pandemic. As a consequence practice-based insights related to the acceptability may be missed.
Future research
More validation and feasibility research is needed of using I-HARP in the hospital setting, general practice and nursing homes in the Netherlands.37 38 Future research is needed to test the criterion validity and reliability of I-HARP. This feasibility research needs to include the roles related to I-HARP in the interdisciplinary context. Also, the participatory role of the patient and the possibilities of using e-health needs to be explored. As more evidence becomes available, we may find arguments to adapt the format and design of I-HARP to make it more usable and feasible for different disciplines. Additionally, more research is needed to determine the effectiveness of I-HARP, to explore the experiences from a patient perspective and to evaluate the implications on resource use.
The open questions to start the conversation and the screening questions to recognise PC needs in CHF seem generally applicable for patients with other life-limiting chronic diseases, with comparable PC needs like COPD and chronic renal failure.39 Further research should explore the content validity of the PC needs and related screening questions to other patient groups and other countries.
Conclusion
I-HARP is a general and accessible tool for HCPs and is promising to facilitate timely recognition and directing of personal PC needs in CHF during a conversation. This study presents the development of I-HARP. The tool is developed specifically for advanced CHF and is appropriate for different HCPs and different settings.
Accessing I-HARP
I-HARP is available in Dutch via the website of the Centre of Expertise for PC of MUMC. I-HARP can be accessed free of charge.
Acknowledgments
The authors thank the patients, family caregivers and health care professionals who participated in this study. The authors thank Liesbeth van Hoef and Loeke Hameleers for their assisting work in carrying out the research.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @StephanieAment
Contributors SA, MvdB-E, JMCM, JB, JMGAS, HEJHS, LB, H-PB-LR, YE and DJAJ contributed to the design and planning of the research. DJAJ is the prinicipal researcher of the I-HARP project. SA, DJAJ, JB and MvdB-E were mainly responsible for the development of the data collection methods and the interpretation of the data. SA was responsible for the data collection and data analyses. SA wrote the draft of the manuscript. SA, MvdB-E, JMCM, JB, JMGAS, HEJHS, LB, H-PB-LR, YE and DJAJ were involved in editing the manuscript. All authors have given final approval of the version to be published. All authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. SA is guarantor.
Funding This project has been made possible by a grant from the Netherlands Organisation for Health Research and Development (ZonMw) as part of the programme Palliantie (grant number 844001511).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The medical ethical committee of the Maastricht University Medical Centre (MUMC+), Maastricht, the Netherlands declared that the study did not fall under the Medical Research Involving Human Subjects Act (2018–0638).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information.