Article Text

Abstract
Objectives To estimate past trends and future projection of adult palliative care needs in Malaysia.
Methods This is a population-based secondary data analysis using the national mortality registry from 2004 to 2014. Past trend estimation was conducted using Murtagh’s minimum and maximum methods and Gómez-Batiste’s method. The estimated palliative care needs were stratified by age groups, gender and administrative states in Malaysia. With this, the projection of palliative care needs up to 2030 was conducted under the assumption that annual change remains constant.
Results The palliative care needs in Malaysia followed an apparent upward trend over the years regardless of the estimation methods. Murtagh’s minimum estimation method showed that palliative care needs grew 40% from 71 675 cases in 2004 to 100 034 cases in 2014. The proportion of palliative care needs in relation to deaths hovered at 71% in the observed years. In 2030, Malaysia should anticipate the population needs to be at least 239 713 cases (240% growth from 2014), with the highest needs among age group ≥80-year-old in both genders. Sarawak, Perak, Johor, Selangor and Kedah will become the top five Malaysian states with the highest number of needs in 2030.
Conclusion The need for palliative care in Malaysia will continue to rise and surpass its service provision. This trend demands a stepped-up provision from the national health system with advanced integration of palliative care services to narrow the gap between needs and supply.
- palliative care
- projection
- Malaysia
- population based estimation
- need assessment
Data availability statement
Data are available on reasonable request. Mortality data were obtained from the National Registration Department and the Department of Statistics Malaysia on request. Population projection data were obtained from the Department of Statistics Malaysia website. Mortality projection data were obtained by personal contact with author Ngataman et al.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Malaysia is an upper middle-income country with a population of 32.6 million people and a crude mortality rate of 5.3 per 1000 population.1 Malaysia, like most countries, is witnessing an increasing number of people dying from life-limiting non-communicable diseases (NCDs) such as cardiovascular disease, cancer, chronic lung disease and renal disease.2 3 Designing adequate care for those in need has become an increasingly important national healthcare agenda in order to preserve patients’ rights to healthcare and their dignity to live, even at the last stage of life. Palliative care provides specialised care for people living with life-threatening illnesses and aims to improve the quality of life of patients and their families.4 WHO emphasises that palliative care is a component of universal health coverage (UHC) which, in turn, is embedded in sustainable development goals that have pledged to ‘leave no one behind’.5 6
Palliative care need is defined as the people who will benefit from the palliative care service.7 Globally, public health efforts have been made to develop methods to estimate the population needs for palliative care services.8–17 Epidemiological approaches have been used to estimate the population needs from the causes of death that would benefit from palliative care.8–13 Some approaches incorporated pain prevalence at the end of life as a multiplier to their mortality data.12 14 15 Other studies look beyond mortality data to include the disease and symptom prevalence of the non-deceased.16 17 More recently, the Lancet Commission on Palliative Care and Pain Relief has created a new construct—serious health-related suffering (SHS)—by combining 20 life-limiting health conditions and 15 corresponding physical and psychological symptoms requiring palliative care, for use in the assessment of the global burden of palliative care needs.16
Projection of future palliative care needs is important for informing policies. Two projection approaches have been described thus far.12 18 Etkind et al 12 used the annual change of the proportion of people requiring palliative care from the baseline years to project future needs. Sleeman et al 18 combined the newly developed SHS multiplier and the global cause-specific mortality projection modelled by the WHO to project future global needs.
Palliative care services were introduced in Malaysia in 1995 and have now been preliminarily integrated into the mainstream healthcare service provision.19 20 In 2016, Hospis Malaysia published the first report to estimate the palliative care needs in Malaysia.15 The authors used hospital mortality data and pain prevalence for selected diseases to estimate the national palliative care need in 2012.15 Despite the authors’ best efforts to provide an estimation for Malaysia, the value of the report was limited by only using a single-year analysis and the lack of comprehensiveness in the selection of illnesses that would benefit from palliative care.14 15 This report also did not provide insight on trends and future forecast.
Understanding the national palliative care needs is imperative for planning health services, but this has remained a knowledge gap in Malaysia. Our study intends to use the epidemiological approach to estimate past trends of palliative care needs and includes a projection of needs up to 2030. To our knowledge, this is the first study to assess national palliative care needs using this approach by an upper middle-income country in South East Asia. The estimation and projection are stratified by administrative states within Malaysia. This study will help policymakers make informed decisions in the development and improvement of palliative care in Malaysia.
Method
Study design and setting
Our study used secondary data from various sources in Malaysia for analysis. The study method was twofold. First, annual palliative care needs were estimated using national mortality data between 2004 and 2014. These results, together with Malaysian population and mortality projection data, were then used to project future palliative care needs up to 2030. In this study, only the adult palliative care population was considered, as the paediatric population would have differing life-limiting disease categories from adults, warranting a stand-alone needs assessment. Therefore, only the adult population aged 15 years and above was included in this study as per WHO adults age classification.21
Estimation of palliative care needs
Many studies have used mortality data to estimate palliative care needs, although these studies vary according to the diseases included in estimating palliative care needs.8–10 14 16 17 The use of mortality data were justified by the definition of palliative care,4 which is to improve patients’ quality of life in life-limiting conditions. We chose not to include the prevalence of pain or SHS in our estimation as the prevalence of symptoms in each illness in Malaysia was not readily available from published data. In our study, we applied methods from Murtagh et al 10 and Gómez-Batiste et al 17 to the number of mortality cases in the Malaysian population from 2004 to 2014. The method described by Murtagh et al was more feasible to conduct in Malaysia, given the limited availability of data and resources. Its scientific validity has been established by its adoption in other countries for the assessment of national palliative care needs.11–13 The estimation is presented in two forms: the absolute number of people requiring palliative care and the proportion relative to total mortality. The estimation methods are as follows:
Minimum estimation method from Murtagh et al 10
This method selects people who died from a selected list of chronic progressive diseases and for whom palliative care was expected to be beneficial. These diseases include malignant neoplasm, chronic heart disease, cerebrovascular disease, renal disease, liver disease, respiratory disease, neurodegenerative disease, Alzheimer’s disease, dementia and senility and HIV/AID (online supplementary appendix 1). The list was discussed and agreed on by the palliative care research and standards subcommittee from the National Palliative Care Development Strategy Technical Group, Ministry of Health Malaysia.
Maximum estimation method from Murtagh et al 10
This method hypothesises that everyone at the end of life will require palliative care, except for cases of sudden death. Therefore, this method suggests that all deaths, except poisoning, injury, maternal, neonatal and perinatal deaths, can benefit from palliative care services (online supplementary appendix 1).
Direct measurement method from Gómez-Batiste et al 17
Gómez-Batiste’s survey showed that approximately 75% of the population from a high-income country died from chronic progressive illnesses and might have benefited from palliative care services. Hence, the author suggests that 75% of all deaths in a country would require palliative care. The calculation is simply to multiply the total crude mortality by 0.75 to derive an estimate of palliative care needs. The estimation from this method served as a comparator and to determine if the 75% rule is applicable to an upper-middle income country.
Supplemental material
Projection of future palliative care needs
We applied the palliative care needs in proportion to population deaths from Murtagh’s minimum estimation method into Etkind et al’s12 projection method to forecast future palliative needs up to 2030. In this method, we calculated the annual change Δ in the age-specific and gender-specific palliative care needs proportion from 2004 to 2014. Then, mean annual change Δ was calculated by averaging the annual change from 2004 to 2014. Assuming that the need will grow in a linear fashion (ie, annual change is constant), we applied the mean annual change Δ to the last observed year to obtain the projection of the palliative care needs proportion of the subsequent years up to 2030.
 , where i=2004, 2005, …, 2014.
, where i=2004, 2005, …, 2014.
 , where n is the n-th projected year after 2014,
, where n is the n-th projected year after 2014,
Pi=proportion in the observed year; Pn=proportion in the projected year.
Data source
National mortality data
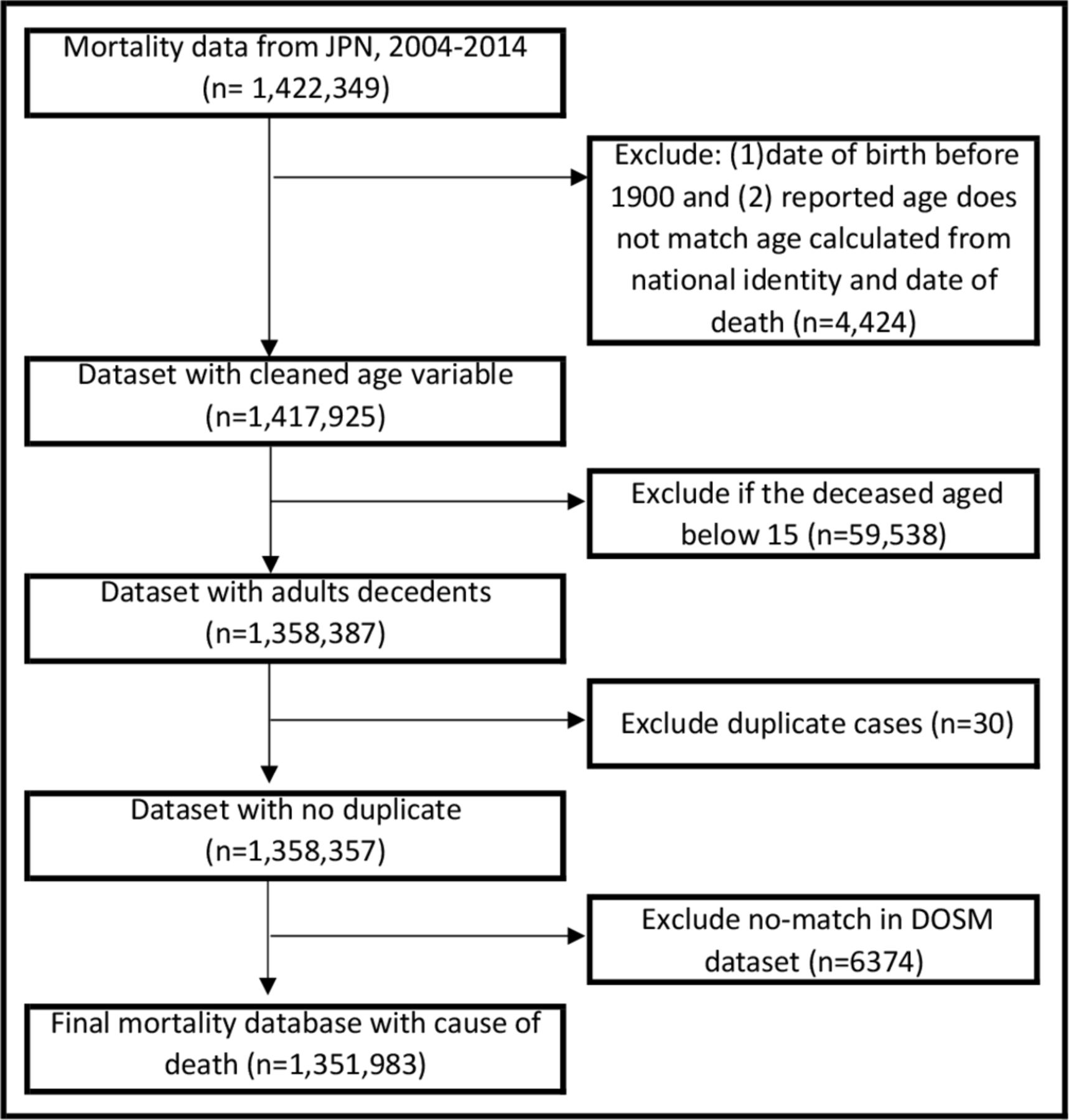
In Malaysia, the National Registration Department (Jabatan Pendaftaran Negara) registers all deaths and issues death certificates, while the Department of Statistics Malaysia (DOSM) categorises the recorded causes of death according to 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD). It was reported that approximately 50% of deaths that occurred in Malaysia were medically certified and ICD-10 coded.3 22 The remaining were non-medically certified deaths—deaths that were certified by policemen. In Malaysia, policemen are authorised to certify deaths that occur outside of medical facilities. The DOSM analysts categorise and code non-medically certified deaths in accordance with the department manual published by DOSM. Each DOSM code has a corresponding ICD-10 code that allows researchers to map the mortality causes according to the respective disease categories.23 In this study, we analysed mortality data from both medically and non-medically certified deaths for the years 2004–2014. Figure 1 shows the process of data cleaning.

Data preparation process for national mortality data. JPN, Jabatan Pendaftaran Negara.
Population data and population projection
Malaysia consists of 13 states and three federal territories.24 Every 10 years, DOSM conducts population and housing censuses in Malaysia. The last Malaysian census was conducted in 2010. DOSM estimated the population data of subsequent years using the 2010 census, and this estimation was revised in 2016 to incorporate changes in the latest mortality, birth and net migration rate. The population data estimation and projection up to 2040 is available on the DOSM website.25
Mortality rate projection (national and state)
We obtained the national age-specific and gender-specific mortality rate projection (2019–2030) from Ngataman et al.26 Subsequently, we multiplied these mortality rates with national population projection data to derive the number of mortality cases occurring nationwide in the projected years.
There is no available mortality projection data for each state in Malaysia. Assuming that the ratio of age-specific and gender-specific death cases in a particular state and nationwide remains constant throughout the years, we multiplied the mean of state-specific death ratio (death ratiosi ) with national mortality projection data to deduce the state-specific death data in projected years. The rationale for this assumption is that death ratiosi was shown to be consistent from 2004 to 2014 with the largest variance of 0.0002.
 , where i= 2004, 2005…2014.
, where i= 2004, 2005…2014.
Death ratiosi =Ratio of age- and gender-specific deaths in s state at year i.
Deathsi =Number of age- and gender-specific deaths in s state at year i.
Deathni =Number of age- and gender-specific deaths nationwide at year i.
Results
Overview of Malaysian population and mortality
Between 2004 and 2014, the Malaysian adult (15 years old and above) population has grown steadily from 17.5 million to 22.9 million. Within this time period, we have identified a total of 1 351 983 deaths in which mortality cases have climbed steadily from 106 836 cases to 141 172 cases annually. The annual mortality rate of the adult population has remained relatively constant at about 6%. By 2030, the Malaysian adult population and annual mortality is projected to be 30 million and 297 992 cases, respectively.
Estimation and projection of palliative care needs, 2004–2030
As per figure 2A, palliative care needs have increased over the years regardless of the estimation methods. The estimated number of people requiring palliative care in 2014 is 100 034 with Murtagh’s minimum estimation method, 132 498 with Murtagh’s maximum estimation method and 105 879 with Gómez-Batiste’s fixed percentage estimation method. While the graph of absolute numbers (figure 2A) demonstrates an apparent upward trend, figure 2B illustrates that the proportion of palliative care needs in relation to deaths hovers at 71% using Murtagh’s minimum estimation method. Projecting these needs to 2030 anticipates a 240% increment from 2014, which equates to 239 713 cases for both genders (figure 3).
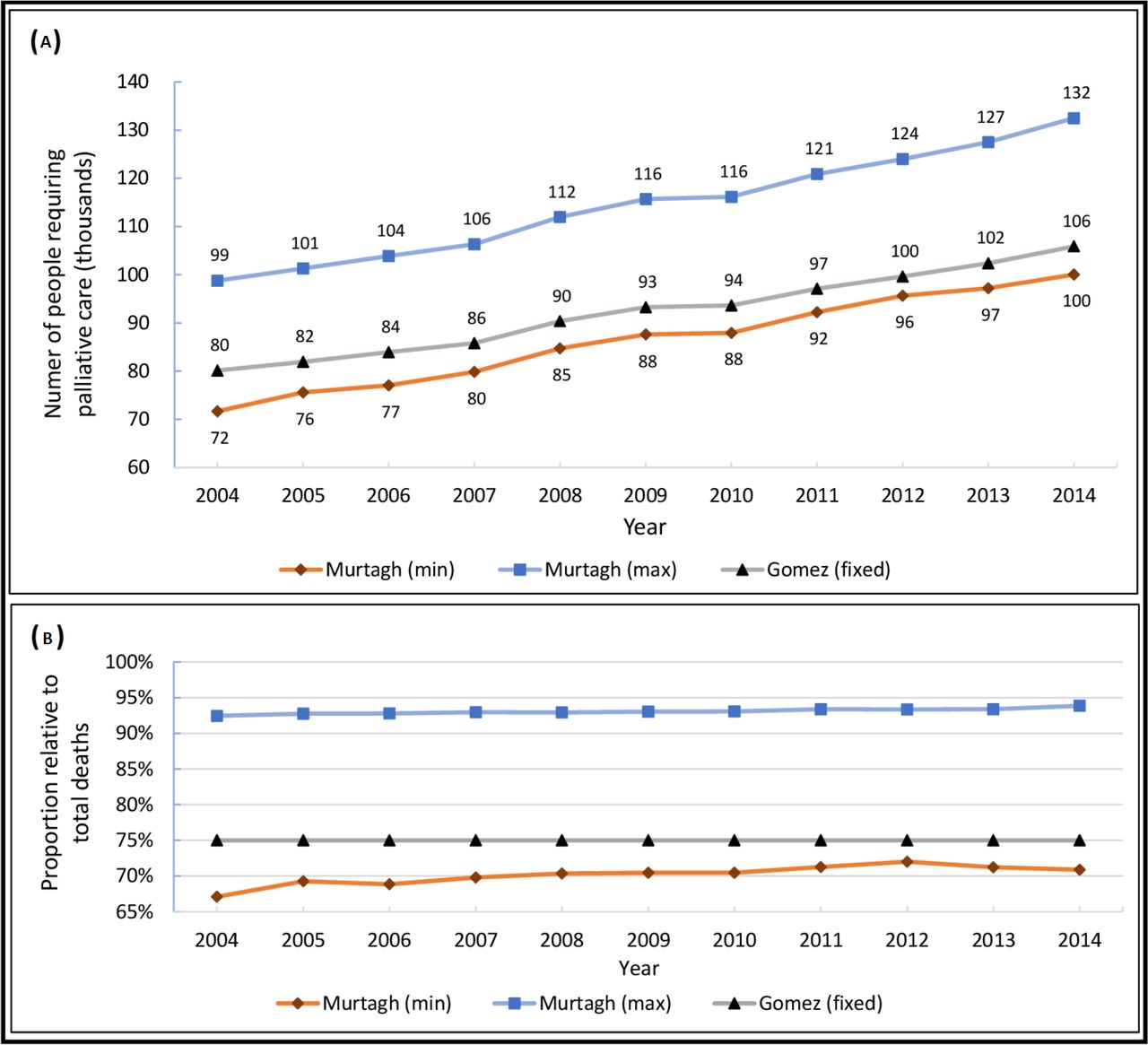
Estimation of palliative care needs from 2004 to 2014 by maximum, minimum and direct measurement estimation methods. (A) The absolute number of palliative care needs in a certain year. (B) The proportion of palliative care needs relative to the number of deaths in a certain year.
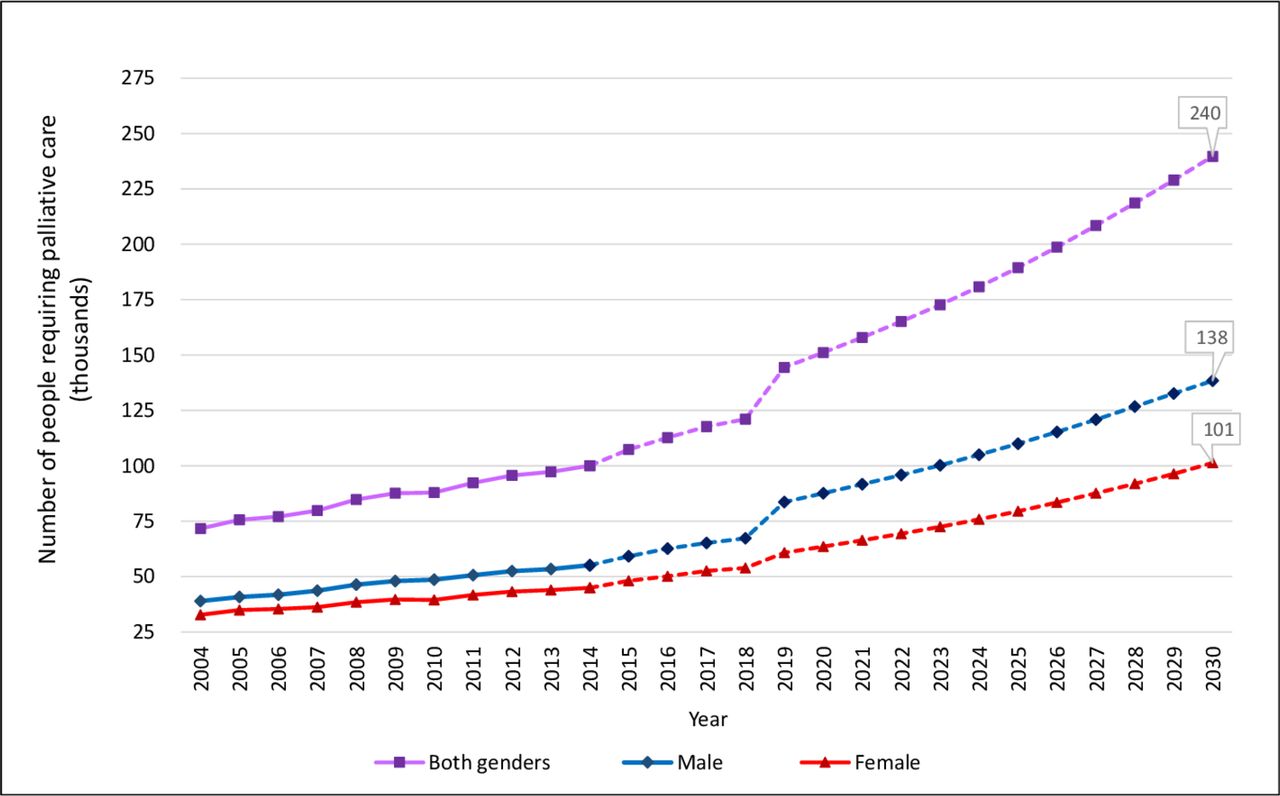
The projection of palliative care needs from 2015 to 2030 for both genders.
Palliative care needs stratified by age and gender
When comparing the palliative care needs of 2004, 2014 and 2030, it is noticeable that palliative care needs in the male population have increased drastically in two age groups: the 65–69 and 80+ years age groups (figure 4A). In the female population, the increment is akin to an exponential curve with the most drastic increment in the 80+ years age group (figure 4B). Overall, men have higher palliative care needs than women across all years (figure 3). In 2014, an estimated 5000 men require palliative care in the 55–59 years age group, while a similar number is only seen in the female population in the 70–74 years age group. The highest increment (47%) in palliative care needs for the female population occurred at the 80+ years age group between 2004 and 2014. It is also only in this age group that more women than men need palliative care. However, by 2030, the projected numbers show that gender difference will no longer be significant in the 80+ years age group, where both men and women will have similar palliative needs (approximately 47 500).

Age-specific and gender-specific palliative care needs in Malaysia in the 2004, 2014 and 2030. (A) Palliative care needs among men and (B) palliative care needs among women.
Palliative care needs stratified by state
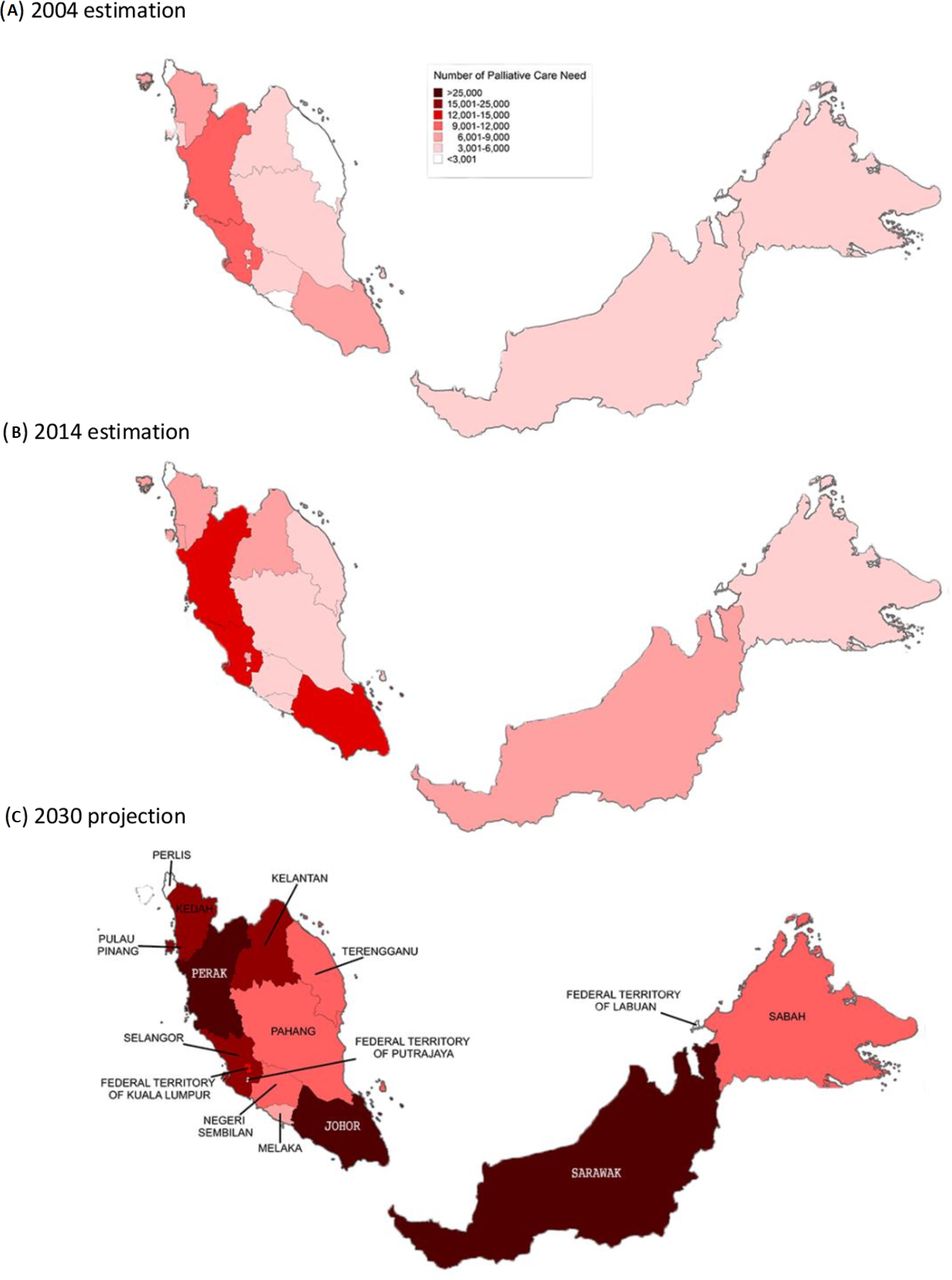
Stratification by state shows that the age-specific and gender-specific palliative care needs in all states and federal territories have increased over the years (figure 5) but at different rates. The areas of higher palliative care needs are concentrated on the West Coast of Peninsular Malaysia. In 2004 and 2014, the highest demand is noted in the West Coast states of Perak, Selangor and Johor. However, the projection illustrates that Sarawak (35 065 estimated cases) will overtake them and top the list by 2030, followed by Perak (27 972 estimated cases), Johor (27 312 estimated cases), Selangor (23 419 estimated cases) and Kedah (20 344 estimated cases). Together, these top five states will contribute to 55% of the country’s total estimated palliative care needs in 2030.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Palliative care needs assessment and projection, stratified by Malaysian states.
Discussion
Key finding
This is the first study in Malaysia and among Southeast Asian countries where a nationwide estimation and projection of palliative care needs has been conducted. This study used 11 years of data to provide insight from the perspective of an upper middle-income country. The estimated population palliative care needs in Malaysia grew 40% from 2004 to 2014 and are projected to increase another 240% by 2030 while the proportion of needs, relative to total mortality, hovered at 71%.
National trend of palliative care need, 2004–2030
The upward trend of palliative care needs (figures 2A and 3) in Malaysia is inevitable as the population and mortality count have increased over the years. This observation is also in line with the fact that Malaysia is undergoing demographic and epidemiological transitions, moving towards an ageing population with a rising burden of NCDs.27 Nine out of 10 leading causes of death in Malaysia in 2017 as published by the Institute for Health Metrics and Evaluation were NCD related28 and could have benefited from palliative care services according to the definition of our study. In this study, needs estimation was conducted using three different methods in order to show the maximum and minimum palliative care needs. Such information is important for healthcare policy makers as it provides an idea of the gravity of the situation and an estimation of the minimum level of service to develop. Globally, only 14% of all who need palliative care are currently receiving it.29 This percentage is even lower in low-income and middle-income countries where palliative care services are not yet fully integrated into national healthcare systems. Therefore, even to meet the minimum need could be challenging for many countries, including Malaysia.
The estimated number of people who needed palliative care in 2015 in our study was lower than the estimation from the Lancet commission on global access of palliative care and pain relief report (107 296 vs 224 000).16 This dissimilarity arises from methodology differences. The Lancet commission reported a higher estimation because it also included the prevalence of SHS from the non-decedents. The prevalence of SHS was a global average, produced by literature review and then adjusted based on the consensus of a 10-member palliative care clinical expert panel. Our study team chose not to apply this average prevalence in our calculations because of the uncertainty of its representativeness in the Malaysian context. Local SHS data are not available.
Our study revealed that the proportion of palliative care needs relative to deaths in Malaysia hovered around 71% in 2010–2014 (figure 2B, Murtagh(min)). Our estimated needs are lower compared with the UK (75%),12 Ireland (80%),30 Germany (78%)13 and various other high-income countries (>75%),11 as well as Gómez-Batiste’s direct measurement method of 75%.17 This difference corresponds with the countries’ NCD burden as the NCD mortality in Malaysia was estimated to be 74%—lower than in the UK (89%), Ireland (90%) and Germany (91%).31 Therefore, we suggest that the palliative care needs for a developing, upper-middle income country—those with similar NCD burden and development status to Malaysia’s—are slightly lower than those of a high-income country.
In figure 3, there was a noticeable increase in the number of people who needed palliative care between 2018 and 2019. This was because we have used two different data sources for calculation. For 2015–2018, the annual change was multiplied with actual, aggregated mortality numbers from vital statistics; for 2019–2030, the annual change was multiplied with projected mortality numbers. We speculate that the mortality projection might have overestimated the deaths in the older age groups, more noticeably in men, and led to the jump between 2018 and 2019.
Palliative care needs of an ageing population
Malaysia is facing the prospect of becoming an ageing country. By 2030, the proportion of the Malaysian population aged 65 years and above will rise to 10%32; the number of deaths will double in the 65+ years age group and triple in the 85+ years age group.32 It is speculated that the aggregated factors of ageing population, longer life expectancy and better healthcare have resulted in the burgeoning increase in palliative care needs. The advancement in the management of chronic diseases in a country with an increasing proportion of the elderly results in more elderly people living longer with multiple comorbidities, requiring palliative care not only at the end of life but in the preceding years. It is evident that palliative care needs are high among an ageing population and palliative care should be integrated into any model of care for the elderly. However, the population growth rate in Malaysia is gradually declining and was as low as 0.6% in 2019. Therefore, population growth rate is not expected to be an influential factor to the increasing palliative care needs.
Current demand and challenges
In line with the national palliative care service development, our projection extended to 2030. Any forecast beyond that may lack accuracy and meaningful application due to the fast-changing healthcare landscape. Our evidence-based forecast reveals that palliative care needs will increase markedly (240%) by 2030, and this poses a significant challenge to the national healthcare system, especially to the palliative care and healthcare planning division.
According to the latest mapping exercise commissioned by the Worldwide Palliative Care Alliance to categorise countries based on perceived levels of palliative care development, Malaysia was placed in ‘Group 4a’, which means a country with preliminary integration of palliative care into mainstream service provision.20 In Malaysia, hospital-based palliative care services are largely delivered by public hospitals and to a smaller extent by private hospitals. Provision of specialist palliative care services are largely concentrated in only a few urban areas.15 Out of 154 Malaysian public hospitals, only seven are staffed with resident palliative care physicians. In 2017, these seven public hospitals and two teaching hospitals collectively received 6628 new referrals for in-patient palliative care.33 However, most community palliative care services are delivered by non-governmental organisations, with an emerging role by domiciliary services from Ministry of Health primary care providers. As with hospital-based services, community palliative care services are also unevenly distributed throughout the country with more services in highly populated regions.15 In 2017, all community palliative care service providers collectively cared for less than 6000 patients.33 This number most likely overlaps with patients reported in hospital-based services due to the lack of a centralised and shared patient registry. The summation of both figures indicates that in 2017, the total number of patients seen in public hospitals and community palliative care services is at best approximately 12 600. This number is just a small fraction (10%) compared with our estimation of 117 673 patients who required palliative care in 2017. Therefore, meeting the current demand remains a significant challenge with many perceived gaps in service provision.
Looking to the future
The overdemand, undersupply situation in Malaysia beckons a new palliative care delivery model that can meet the dire need of people in high demand states. The national palliative care development strategy committee plans to execute a ‘palliative care hub model’ to serve different regions in Malaysia (North, South, East, Central, Sabah and Sarawak). These palliative care regional hubs will focus on strengthening and developing services for both inpatient and community palliative care needs, increasing human resource capacity through education and training of generalists and specialists, as well as running research and quality improvement activities to ensure care is in accordance to globally accepted standards of care. Therefore, the findings of this study are well timed to assist healthcare service directors and policy makers in Malaysia to make informed decisions regarding future allocation of human resources and the locations of regional hubs in the country.
Limitations
There were a few limitations in our study. First, we were constrained by data availability and could not include more recent data to improve the accuracy of our projection. Second, the national mortality rate projection may have overestimated the number of deaths in the older age group, hence the jump in figure 3. The mortality rate projection was only available up to 2030, hence limiting the number of years that we can project forward. We decided to use it nonetheless because it was the only available projection data officially published. Third, we used disease mortality, instead of disease prevalence, to estimate the palliative care needs. This led to an underestimation in certain disease groups such as dementia and neurodegenerative diseases because these diseases are rarely recorded as the cause of death in death certificates.34 We acknowledge that the level of accuracy in recorded causes of death can hamper the estimation in our study. Despite the limitation, the national death registry has served as a key resource in generating nationwide statistics for guiding policy making and has contributed to research work both nationally and internationally. The accuracy and validity of the national death registry is acceptable for research purposes. Fourth, the application of this study is limited to the adult population (>15 years old) as paediatric palliative care services would include different groups of diseases in estimating needs for their unique patient population. An estimation conducted on the Malaysian paediatric population has already been published.35 Fifth, the cases with ICD codes I12 (death due to hypertensive renal disease) and I13 (death due to cardiorenal disease) were included twice in our calculation, in both chronic heart disease and chronic renal disease categories. These ICD codes could not be confidently reclassified into either category and so were kept in both categories and double counted. However, there were only 30 such cases (<0.005%) throughout the 11-year period. Next, our projection analysis assumed the growth rate of palliative care needs to be in a linear fashion, and we did not account for potential changes of patient outcomes and medical treatments in the future. However, the robustness of this method has been proven in previous literature.12 Lastly, we assumed the state-to-country death ratio to remain the same in the projected years. This assumption was justified by the static ratio observed in the past decades and is not expected to vary much except in situations of mass casualty or pandemic.
Implication
This is the first study to simultaneously apply estimation and projection methods from Murtagh et al, Gómez-Batiste et al and Etkind et al in order to gain insight into the population palliative care needs in an upper middle-income, developing country. Although more comprehensive methods of needs assessment are available, developing countries often face impediments from the lack of manpower and financial resources, complete and representative datasets, and technical expertise. Apart from applying the aforementioned methods, our study demonstrated a way to overcome the lack of state mortality projection to project state-level needs. Our study exemplified feasible methods to perform an estimation and projection exercise in any developing country seeking a quick estimation for its population palliative care needs.
Conclusion
Quantification of palliative care needs and a thorough understanding of its demography stratification is a crucial first step to designing a better palliative care model for Malaysia. It is apparent that palliative care needs in Malaysia will continue to exceed the service provision as the number of NCD cases, population life expectancy and patients’ expectations for healthcare services increase. In light of the increasing burden of palliative care and a national commitment to achieve UHC, a national health system with advanced integration of palliative care services must be implemented.
Data availability statement
Data are available on reasonable request. Mortality data were obtained from the National Registration Department and the Department of Statistics Malaysia on request. Population projection data were obtained from the Department of Statistics Malaysia website. Mortality projection data were obtained by personal contact with author Ngataman et al.
Ethics statements
Patient consent for publication
Ethics approval
This study was conducted in accordance to the ethical principles outlined in the Declaration of Helsinki and the Malaysian Good Clinical Practice Guideline. The study was registered under the National Medical Research Register (NMRR-18-3311-45428) and approved by the Medical Research Ethics Committee, Ministry of Health Malaysia.
Acknowledgments
The authors would like to thank the Director General of the Ministry of Health Malaysia for his permission to publish this article. The authors also wish to extend their sincere appreciation to the National Registration Department, Department of Statistics Malaysia, Research and Standards Subcommittee from the National Palliative Care Development Strategy Technical Group and Centre for Clinical Outcome Research from the Institute for Clinical Research for their support in this study. The authors would like thank Mr Christopher Wylie for his kindness to proofread the manuscript.
References
Footnotes
Contributors SLY, YLW and CCOT have contributed to the conception or design of the study; SLY, YLW and CTL have contributed to data collection; SLY, YLW and CTL have contributed to the data analysis; SLY, YLW, CCOT and RL have contributed to data interpretation; SLY drafted the manuscript; SLY, YLW, CCOT and RL were involved in critical revision of the manuscript. All authors gave their final approval of the version to be published.
Funding This study was fully funded by the operating budget of the Institute for Clinical Research, Ministry of Health Malaysia.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.