Article Text

Abstract
Background Family caregivers of patients with advanced cancer have been reported to provide long hours of care and be at risk for poor psychological outcomes. Although research has focused on the nature of caregiving burden, little attention has been paid to identifying protective factors that improve caregiver psychological outcomes.
Aim We examined the relationship between caregivers’ time spent caregiving and the following psychological outcomes: anxiety, depression and caregiving esteem. Subsequently, we explored the main and moderating effects of caregiver-perceived self-competency and sense of meaning on caregiver psychological outcomes.
Design/participants Cross-sectional analysis was conducted using the baseline data from an ongoing cohort study. Family caregivers of advanced cancer patients (n=287) were recruited from two tertiary hospitals in Singapore.
Results Time spent caregiving was not significantly associated with caregiver anxiety, depression or caregiving esteem. However, significant main effects of self-competency on anxiety and caregiving esteem; and sense of meaning on anxiety, depression and caregiving esteem were observed. Moderator analyses further indicated that self-competency attenuated the positive relationship between time spent caregiving and anxiety, while sense of meaning attenuated the negative relationship between time spent caregiving and caregiving esteem.
Conclusion Greater perceived self-competency and sense of meaning are related to better caregiver psychological outcomes, and protect caregivers from worsening outcomes as caregiving hours increase. Our findings suggest that screening caregivers for distress is an important part of care, and that supportive interventions for caregivers should aim to enhance their perceived caregiving competencies and the ability to make meaning of their caregiving role.
- caregivers
- cancer
- anxiety
- depression
- meaning-making
- competency
Statistics from Altmetric.com
Introduction
Cancer affects not just the individual patient but their family and loved ones as well. Informal family caregivers (hereafter referred to as caregivers) of patients with advanced cancer who are symptomatic and experience functional decline may be at risk for poor outcomes themselves.1 2 Prior studies have documented issues faced by caregivers related to caregiving responsibilities and their impact on daily life.3 4 Many of these, such as disrupted personal schedule, disruption in career advancement, loss of contact with friends and feelings of burnout, are linked to caregiving load and suggest that increased caregiving hours are associated with worse caregiver psychological outcomes.5 6
The caregiving role can occupy the caregiver at the expense of their own self-care and in some cases their self-identity. An estimated 20%–63% of caregivers of patients with cancer report psychological distress, defined as elevated levels of depression and anxiety.5 7 This may be accompanied by decreases in caregiving esteem, which refers to positive attitudes towards caregiving.8 9 Feelings of joy or reward (or conversely, distress or resentment) from caregiving can have consequences on caregivers sense of self-worth and quality of life.8 10
According to Pearlin’s stress process theory applied to caregiving, factors that predict caregiver outcomes may be generally classified as caregiver background/context, direct caregiving stress and social/psychological resources of the caregiver.11 Nijboer et al 12 further posited that intrinsic caregiver psychological resources have a moderating effect on caregiver outcomes to explain the variability observed in caregiver outcomes under similar caregiving circumstances. In this study, we conceptualised time spent caregiving as direct caregiving stress. We also examined two psychological resources of caregivers: self-appraisal of their competence and ability to engage in meaning-making, as they may be potentially protective for caregivers11 and are cognitively/behaviourally modifiable. Having a sense of mastery over caregiving tasks (ie, high self-competence) has previously been reported to lower the risk for depression of caregivers of cancer and non-cancer patients.12 13 Higher levels of caregiver spirituality (of which sense of meaning is a component) have also been associated with better mental health and have been shown to have a protective effect.14 15 However, no studies have specifically examined the moderating role of self-competence and sense of meaning in the relationship between time spent caregiving and caregiver outcomes.
The aim of this paper was to investigate the relationship between time spent caregiving and the following caregiver psychological outcomes: anxiety, depression and caregiving esteem using caregiver self-reported data. We hypothesised increased caregiving hours to be associated with higher anxiety and depression and lower caregiving esteem. We also hypothesised that caregiver-reported self-competency and sense of meaning of their situation will have main and protective moderating effects on caregiver psychological outcomes. Specifically, we expected greater self-competency and sense of meaning to independently (1) attenuate the positive effect of time spent caregiving on anxiety and depression and (2) attenuate the negative effect of time spent caregiving on caregiving esteem. Understanding the potential value of these protective factors will help in the formulation of targeted interventions to improve outcomes of caregivers of patients with advanced cancer.
Methods
Participants
The current cross-sectional study utilises baseline data from family caregivers of advanced cancer patients from a cohort project described elsewhere.16 This study included informal family caregivers of patients with a diagnosis of advanced (stage IV) solid tumour malignancy where patient-caregiver dyads completed a self-report assessment. An informal family caregiver is defined as one of the main persons (1) providing care to the patient (eg, accompanying patient for doctor’s visits, helping the patient with day-to-day activities) or (2) ensuring the provision of care to the patient (eg, hire or supervise domestic helper, which is common practice in Singapore) or (3) involved in making treatment decisions on behalf of the patient. Hired domestic helpers were excluded.
Recruitment and data collection
The study recruited patients from medical oncology outpatient clinics of two tertiary hospitals in Singapore. Following screening of clinic lists, trained research assistants approached eligible patients and caregivers for study participation while they were in the clinic waiting rooms. Consent forms and surveys for study participants were administered in English, Mandarin or Malay. Study participants provided written consent and were compensated for their time. Surveys were completed in the clinic waiting rooms or, if the caregivers were pressed for time, at home via an online survey link.
Study outcomes
Time spent caregiving
Caregivers were asked the question ‘On average, about how many hours do you spend caring for or ensuring provision of care for the patient in a typical week?’.
Anxiety and depression
Caregiver’s level of anxiety and depression were assessed using the Hospital Anxiety and Depression Scale (HADS).17 The HADS has 14 items, which yield two subscales: anxiety and depression. The instrument has been validated for use in Singapore in English, Mandarin and Malay18–20 and has been reported to be valid and reliable (Cronbach α=0.74–0.85).20 A score of 0–21 was calculated, with a higher score indicating greater symptoms of depression or anxiety. A score of ≥8 on either subscale has been established to be a threshold of potential anxiety or depression.21
Caregiving esteem
The self-esteem subscale of the modified Caregiver Reaction Assessment Scale was used.22 The subscale consists of six items, which are used to measure caregiver’s positive feelings towards their caregiving duties. Example items include ‘Caring for patient is important to me’ and ‘Caring for patients makes me feel good’. The items were answered on a scale of 1–5 and summed to give a potential range of 6–30. Higher scores indicate higher caregiving esteem. The instrument has been validated and shown to be reliable for use in Singapore (Cronbach α=0.81).22
Self-competency
The 4-item Caregiver Competence Scale11 was used. Example questions include ‘How much do you feel that, all in all, you are a good caregiver to patient?’ and ‘How self-confident do you feel about providing care to patient?’ A total score ranging from 0 to 12 was calculated, with higher scores indicating greater perceived caregiving competence. The scale has demonstrated good validity and reliability (Cronbach α=0.86) among caregivers of patients in palliative care.23
Sense of meaning
Caregivers responded to eight items of the Meaning/peace subscale of the Functional Assessment of Chronic Illness Therapy-Spiritual (FACIT-Sp).24 Example items include ‘I feel peaceful’ and ‘I feel a sense of purpose in my life’. A score of 0–32 was calculated, with higher scores representing greater sense of meaning in life.
Data analytic plan
In order to determine the sample size for the moderation analyses, a power analysis was conducted using the G*Power program. With a medium effect size (f 2) of 0.15, an alpha of 0.05, a standard power level of 0.80, a total of 3 tested predictors and 13 total predictors, the results of the power analysis showed that a minimum of 119 participants would be needed to achieve an appropriate power level for this study.
Descriptive data on the sample’s sociodemographic and clinical characteristics, as well as study variables of interest were tabulated. Unadjusted and adjusted Pearson’s correlation coefficients were calculated to determine the associations among study variables of interest. The moderator regression analyses were conducted using Model 1 of the PROCESS macro developed by Hayes25 where the following were entered: independent variable (caregiving hours), dependent variables (anxiety, depression and caregiving esteem), moderator variables (self-competency, sense of meaning) and covariates (age, gender, relationship to patient, self-reported adequacy of finances (as presented in table 1), patient distress from the total HADS scores, caregiving duration and availability of caregiving help). Availability of caregiving help was assessed by asking caregivers one yes/no question: ‘In addition to you, did someone else also help the patient perform these activities? Include any members, friends, neighbour, maid, paid worker, visiting nurses, etc’. Caregiving duration was assessed by asking caregivers the question ‘About how long ago did you first start helping the patient do things that he or she was no longer able to do alone because of his/her illness/cancer?’ We did not control for patient’s physical status as patients were required to be completely ambulatory (Eastern Cooperative Oncology Group [ECOG] performance status 0 or 1) at the time of assessment.
Caregiver characteristics (n=287)
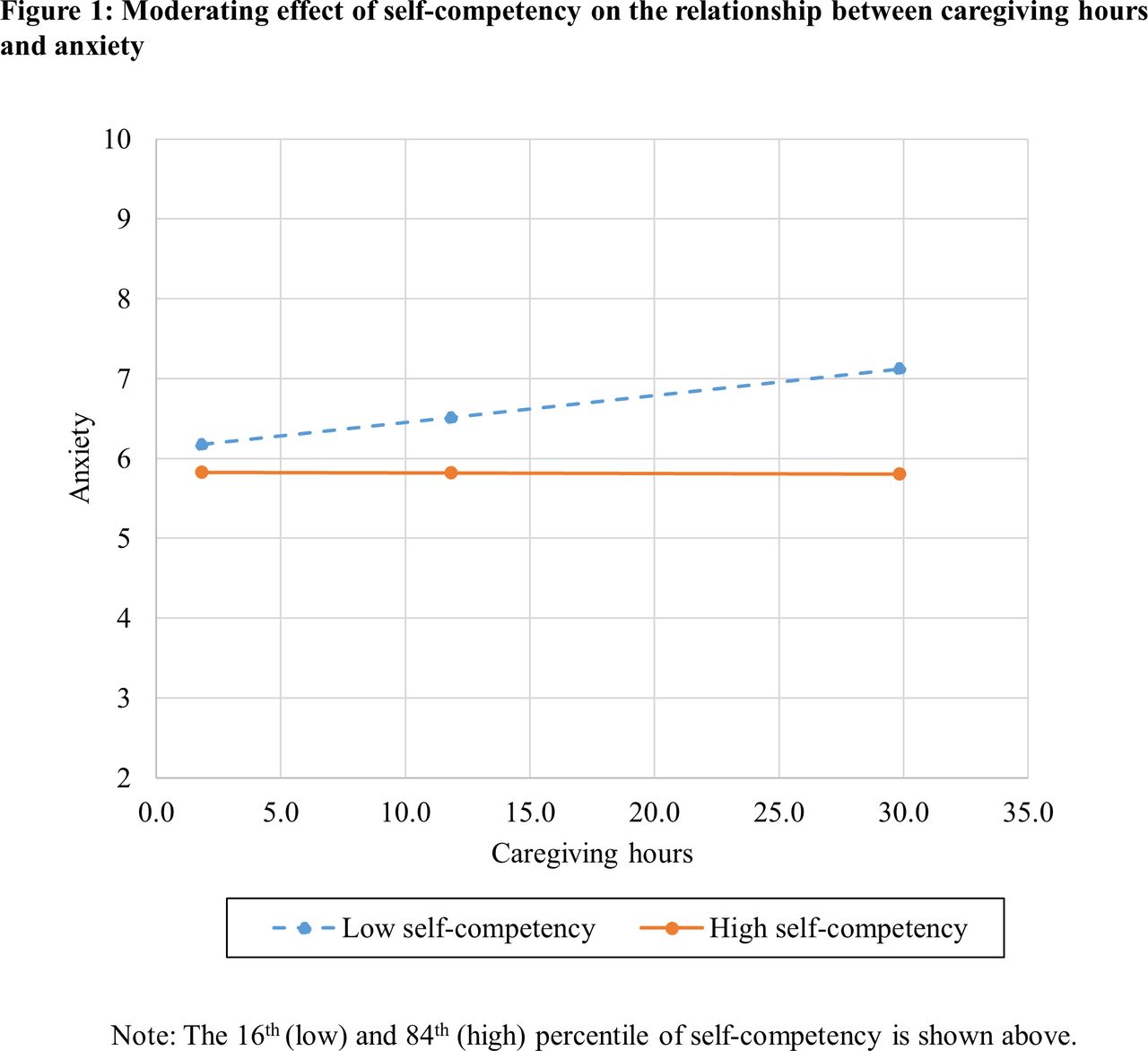
All predictor variables which were continuous (caregiving hours, competency, sense of meaning) were centred by subtracting the mean from the original score as recommended by Kraemer and Blasey.26 All predictor variables that were categorical were dummy coded prior to entering into the models. The moderating effect was estimated using an interaction term of the moderator and the independent variable. To visually inspect the relationship between caregiving hours and outcomes at different levels of moderating variables, we plotted graphs at two values of the moderator: the 16th and 84th percentile values because they correspond to the values of the mean±1 SD in a normal distribution. All statistical analyses were conducted using the Statistical Package for the Social Sciences 25.0. Statistical significance was set at p<0.05.
Results
Descriptive statistics
A total of 387 eligible caregivers were approached to participate in the study and 325 consented. The main reasons for non-participation were lack of time and disinterest. Most caregivers who declined were working full-time or stated they were too busy. Out of this, we used data from family caregivers where the patient-caregiver dyad completed the self-reported assessment (n=287) in order to control for patient distress scores. Caregiver and caregiving characteristics are presented in table 1. Mean age of caregiver participants was 51 years, and the majority were Chinese (76%), female (63%) and spouses of the patient (51%). Half of the caregivers had full-time jobs at the time of the survey. Three-quarters of caregivers co-habited with the patient (77%).
Patients being cared for had a mean age of 62 years (SD=10) with approximately half (52%) being female. The most common cancer site was lung (26%), followed by colorectal (15%) and genitourinary (15%). The majority of caregivers reported that they helped patients with at least one instrumental activity of daily living (eg, light housework, using public transport) and one healthcare-related task (eg, healthcare appointments, taking medicines). The mean caregiving hours per week was 17.43 hours and mean duration of caregiving was 2.5 years.
Table 2 presents the mean scores of the study variables of interest. More than a third (38%) of caregivers reported scores that met the threshold for potential anxiety, and almost a third (31%) reported scores that met the threshold for potential depression on the HADS (table 2). The mean scores for caregiving esteem, self-competency and sense of meaning were generally high.
Caregiver psychological outcomes and moderating variables (n=287)
Correlations between time spent caregiving and study outcomes of interest
Table 3 shows that caregiving hours were not associated with anxiety, depression or caregiving esteem. Caregiving hours were positively correlated with self-competency (p<0.01) in unadjusted and adjusted analyses. Correlations between other study variables of interest were in the expected directions.
Correlation between caregiving hours and caregiver psychological outcomes (n=287)
Main effects of self-competency and sense of meaning
Results from the multivariable linear regressions analyses are presented in table 4. The main effects of self-competency were statistically significant for anxiety (p<0.05) and caregiving esteem (p<0.01). Among caregivers who had an average level of caregiving hours (zero after mean-centering), higher self-competency was associated with lower anxiety and higher caregiving esteem.
Linear regression examining main and moderating effect of self-competency and sense of meaning (n=287)
Furthermore, the main effects of sense of meaning were statistically significant for anxiety, depression and caregiving esteem (all p’s<0.01). Among caregivers who had an average level of caregiving hours, higher sense of meaning was associated with lower anxiety and depression and higher caregiving esteem.
Moderating effects of self-competency and sense of meaning
Self-competency moderated the relationship between caregiving hours and anxiety (b=−0.01; p<0.05) (table 4). As seen in figure 1, for caregivers who reported high levels of self-competency (84th percentile), anxiety levels were maintained as caregiving hours increased, while for caregivers who reported low levels of self-competency (16th percentile), anxiety increased as the number of caregiving hours increased.
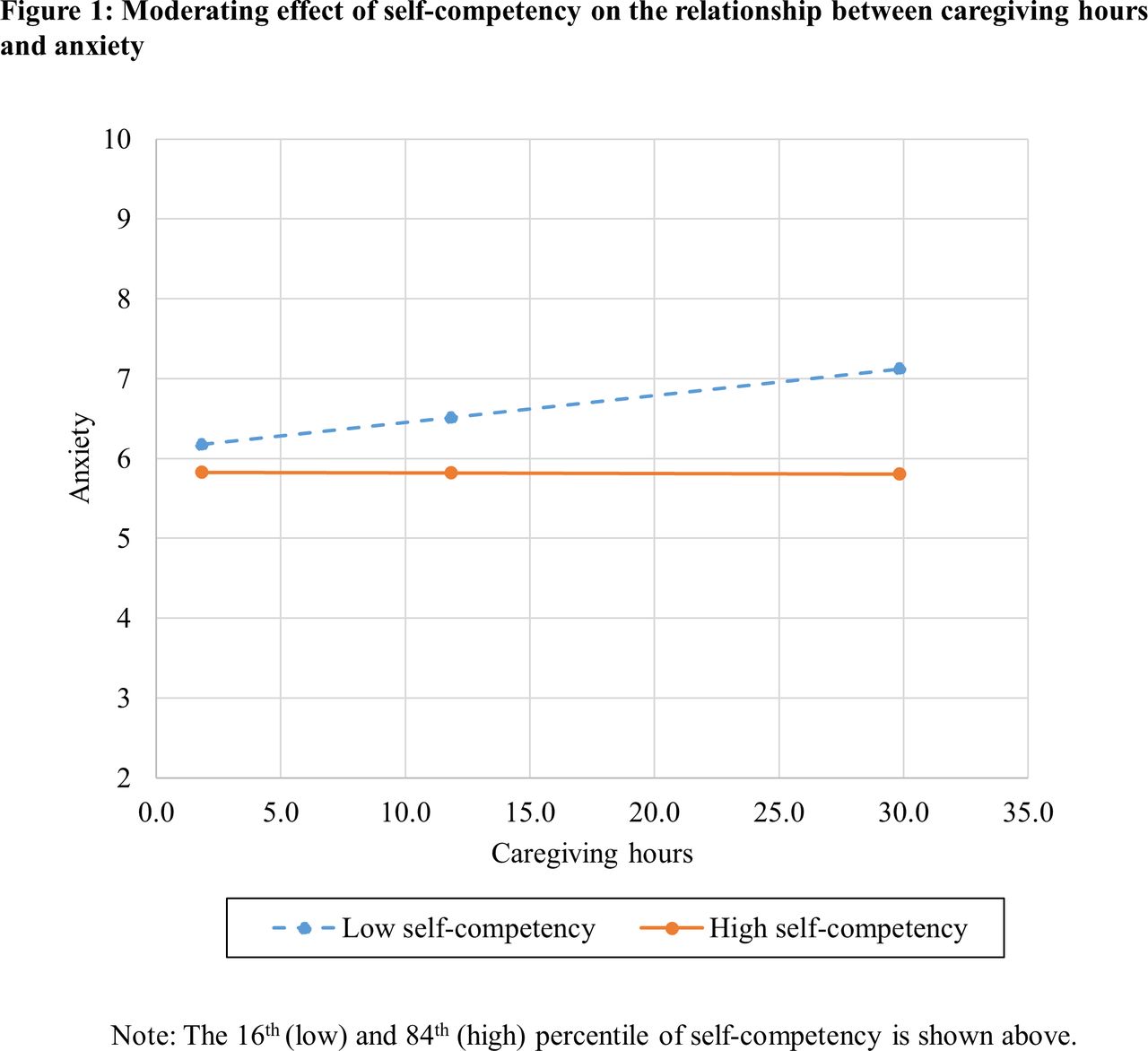
Moderating effect of self-competency on the relationship between caregiving hours and anxiety.
Sense of meaning moderated the relationship between caregiving hours and caregiving esteem (b=0.004, p<0.05) (table 4). As seen in figure 2, for caregivers who reported a high sense of meaning (84th percentile), caregiving esteem increased with the number of caregiving hours, while for caregivers who reported a low sense of meaning (16th percentile), caregiving esteem decreased as the number of caregiving hours increased.

{kind=link}
{kind=link}
Moderating effect of sense of meaning on the relationship between caregiving hours and caregiving esteem.
Discussion
The current paper sought to investigate the psychological outcomes of informal family caregivers of patients with advanced cancer and the extent it was associated with time spent caregiving. We also examined the main and moderating effects of caregiver-reported self-competency and sense of meaning on the relationship between time spent caregiving and caregiver psychological outcomes. The scores indicative of anxiety and depression for our sample were consistent with other studies among informal caregivers of patients with cancer in Singapore27 and other countries.28 29 Caregiving esteem scores in our sample were also comparable with estimates from a national survey of primary informal caregivers of older community dwelling Singaporeans with functional limitations.22
Contrary to expectations, we found that time spent caregiving was not significantly associated with depression, anxiety and caregiving esteem. This indicates that caregiving hours per se may neither be directly related to nor be the sole predictor of caregiver psychological outcomes. We found, instead, that the associations between time spent caregiving and certain caregiver psychological outcomes vary by levels of caregivers’ perceived self-competency and ability to make meaning of their situation, controlling for caregiver demographic characteristics, patient distress and availability of caregiving support. We also found self-competency and sense of meaning to be directly related to psychological outcomes.
Higher levels of self-competency were associated with lower anxiety and higher caregiving esteem. Caregiver’s perceived self-competency also moderated the relationship between time spent caregiving and anxiety. Our findings suggest that feeling competent–in this case, feeling capable of providing care to an advanced cancer patient successfully–protects a caregiver from feeling anxious even as caregiving hours increase. For instance, at 30 hours of caregiving per week, the difference in scores for caregivers who report high versus low competency is approximately 1.3 points on the HADS anxiety, which is approaching a meaningful clinical difference.30 An important aspect of competency is the feeling of being in control (ie, the opposite of feeling helpless), which can help the caregiver cope with the stress from caregiving demands.11 13 Our findings are consistent with one previous study that reported mastery to moderate caregiver outcomes, though the moderated relationship was different.12
Caregiver’s sense of meaning was negatively associated with levels of anxiety and depression, while positively associated with caregiving esteem. Sense of meaning further moderated the relationship between time spent caregiving and caregiving esteem. The results indicate that caregivers who are better at making meaning of their situation are more likely to have positive feelings towards their caregiving role even as caregiving hours increase. Our findings are consistent with the limited existing literature on cancer caregivers, which reports spiritual well-being (a composite measure including sense of meaning and faith) to be positively associated with caregiving esteem31 32 but not associated with caregiving hours.33 Furthermore, a study on cancer caregivers indicated that higher overall spirituality can serve as a protective buffer from negative mental health outcomes.34 This may explain why caregiving esteem, a subjective aspect of the caregiving experience, can increase for those who are able to make meaning of their circumstances despite rising demands of caregiving.
We note that the average time spent caregiving in our sample was only around 17.4 hours per week (approximately 2.5 hours/day); this figure is relatively low compared with estimates of caregiving hours in the literature, perhaps because the patients being cared for were required to be independent in self-care and ambulatory (ECOG status ≤1) and a majority of our sample reported receiving caregiving help, including from domestic workers. A recent study among caregivers of patients with advanced cancer in Singapore27 reported a majority of caregivers to spend 84 hours or more per week providing care. Similarly, caregivers of terminally ill cancer patients in Taiwan also reported higher estimates of caregiving hours (46% reported 56 hours or more per week)35 relative to our sample. However, both these estimates are obtained from caregivers of patients who had been admitted to hospital and thus, were likely to have poorer functional status than patients in our sample. As we analysed only baseline data from our cohort study, the majority of caregivers in our sample were recruited when their patients were relatively well. We expect caregiving demands for patients to increase over time as patient’s functional status decline.
Our study has several clinical implications. First, given that a significant proportion of caregivers experienced clinically relevant distress (anxiety and depression) scores, screening caregivers of advanced cancer for distress should be an important part of care. Second, while caregivers are usually not targeted during cancer patients care trajectory, existing literature suggests that caregiver’s psychological outcomes are significantly associated with patient’s well-being.1 2 This supports the development of interventions that target advanced cancer patient-caregiver dyads as a unit of care rather than focusing exclusively on patients, such as the FOCUS program for prostate cancer,36 psychosocial programme for lung cancer37 and pain tele-monitoring programme for advanced cancer.38 Additionally, our results indicate that supportive interventions for caregivers should target enhancing caregiver’s ability to make meaning of their situation and perceived caregiving competency, as our findings suggest them to be protective. Although there are a number of interventions for caregivers that target caregiving skill competency,36 37 there is currently a paucity in those that focus on meaning-making.39
From a public health perspective, delegation of caregiving to family caregivers is crucial as it prevents the overburdening of the formal healthcare system. However, support for informal caregivers is essential to prevent burnout, which can have dire consequences for the patient, caregiver and the rest of their family. As with many other ageing populations, Singapore expects the needs of individuals providing informal care to increase in the near future and has recently developed a multipronged Caregiver Support Action Plan, which among other offerings provides training grants to improve caregiving skills and caregivers of palliative patients home-based respite services.40 Building on these initiatives will be critical as the caregiving burden among family caregivers increases. Apart from caregiving competency and meaning-making, there may be other psychosocial resources (eg, problem-solving skills, self-care, religious coping) which can be helpful to caregivers and, thus, warrant further investigation.
Our study has several limitations. First, not all caregivers of patients in the cohort study participated. We also only analysed cross-sectional data from a cohort study and did not examine changes in caregiver outcomes as the patient’s disease progresses. It is possible that the association between the outcomes of interest change over time as the patient gets closer to death. In addition, being a cross-sectional study, we cannot infer causality but only associations. Lastly, there are other indices of caregiving intensity other than caregiving hours, for instance complexity of caregiving tasks, that were not available and hence, were not considered in this study.
In summary, this study contributes to the understanding that caregivers’ perceived competency and their ability to make meaning can play a protective role for caregiver anxiety and caregiving esteem as demands for caregiving increase. Future research should consider prospective data to enable us to examine how caregiving outcomes evolve over time and also consider the effectiveness of interventions that target caregiver competency and sense of meaning of their situation.
References
Footnotes
Contributors IT, SOVD, CM, RS, YBC and EF were involved in study planning. IT, RS, GMY, PSHN, RK, NBK and LHL were involved in study conduct. IT, DB and RS led to the preparation of the manuscript. All authors were involved in the reporting and reviewing of the manuscript.
Funding The study is funded by Singapore Millennium Foundation (2015-SMF-0003) and Lien Centre for Palliative Care (LCPC-IN14-0003).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study protocol was approved and is being monitored by the SingHealth Centralised Institutional Review Board (Ref: 2015/2781).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data that support the findings of this study are available from the
corresponding author upon reasonable request.