Article Text

Abstract
Objectives Some failures in end-of-life care have been attributed to inconsistent provision of palliative care across England. We aimed to explore the variation in commissioning of services by Clinical Commissioning Groups (CCGs) using a data collection exercise.
Methods We sent a Freedom of Information request in the form of an open questionnaire to all 209 CCGs in England to assess their commissioning of palliative and end-of-life care services, mainly focused on the provision of specialist palliative care services.
Results 29 CCGs provided information about the number of patients with some form of palliative care needs in their population. For specialist palliative care services, CCGs allocated budgets ranging from £51.83 to £2329.19 per patient per annum. 163 CCGs (77.90%) currently commission 7-day admission to their specialist palliative care beds. 82.84% of CCGs commission 7-day specialist palliative care services in patients' own homes and out-of-hours services rely heavily on hospice provision. 64 CCGs (31.37%) commission pain control teams, the majority of whom only operate in regular working hours. 68.14% of CCGs reported commissioning palliative care education of any sort for healthcare professionals and 44.85% of CCGs had no plans to update or review their palliative care services.
Conclusions The most important finding from this exercise is that the information CCGs hold about their population and services is not standardised. However, information based on data that are more objective, for example, population and total budget for palliative care, demonstrate wide variations in commissioning.
- Communication
- Education and training
- Hospice care
- Hospital care
- Home care
- Service evaluation
Statistics from Altmetric.com
Introduction
Specialist palliative care is a specific level of service provided by professionals who have undergone specialist training in palliative care and who are members of a specialist palliative care team (including specialists in palliative medicine and palliative nursing). Specialist palliative care often supports patients who have a complex terminal illness, whether dying or earlier in their illness. More general, palliative and end-of-life care can be provided by any healthcare professional, who is not required to have specific palliative training, but may require support from specialist palliative care. For example, physiotherapists may provide support to a dying patient, but would not be required to have end-of-life care training to do so.1 The National End of Life Care Intelligence Network (NEoLCIN) estimate that currently 171 000 people across the UK receive specialist palliative care input, but that 92 000 people per year have unmet palliative care needs.2
In 2015, several reports highlighted deficits in the provision of all palliative care services. Marie Curie reported that 65% of medical professionals stated that poor coordination between different palliative care agencies left many with unmet palliative care needs.3 The Economist Intelligence Unit suggested that pain control and out-of-hours services needed improvement,4 and a BBC investigation revealed failures in out-of-hours medication.5
In May 2015, the Parliamentary and Health Service Ombudsman (PHSO) published a thematic report entitled ‘Dying without Dignity’, which identified six themes in palliative care failings in England6
Not recognising that people are dying, and not responding to their needs.
Poor symptom control.
Poor communication.
Inadequate out-of-hours services.
Poor care planning.
Delays in diagnosis and referrals for treatment.
The 2012 Health and Social Care Act requires that Clinical Commissioning Groups (CCGs) provide services to meet the needs of their local population. However, since this legislation passed, no comprehensive survey has reviewed current palliative care service provision across England.7 ,8 To address this, we sought data from all 209 CCGs in England about the palliative care services they commission.
This study was undertaken during preparation of the private members bill, Access to Palliative Care Bill 2015–2016, which has been retabled in Parliament in June 2016. In several parliamentary debates, MPs and Peers highlighted considerable variation in palliative care provision with variable services and no clear standards around what constitutes good end-of-life care.9
The study also uses the Welsh Palliative Care Strategy, which was developed in 2008, as a best practice model for comparison. The strategy aimed to establish fair access to specialist palliative care across Wales on a 24/7 basis at a time when Welsh Health Boards faced many of the issues identified by the PHSO's report. The success of the Welsh strategy was partly due to the development of a funding formula, which used data on the population to be served to provide community services, hospice beds and hospital support teams. This funding formula established services in deprived areas that previously had no specialist palliative care team, with specialist consultant telephone advice available at all times, improved access to medication, education of generalists and direct patient evaluation of their care.10 The funding formula was reiterated in the subsequent 2013 strategy.11
We compared the CCG information obtained through this exercise, with the Welsh funding formula model to explore differences in hospice bed provision when a national standard is not in place. We also explored variables in specialist palliative care and general end-of-life services commissioned.
Methods
Study design
Data on the commissioning of specialist and generalist palliative care services in England were obtained through a Freedom of Information (FOI) request. Prior discussion with a CCG lead clarified that FOI requests create an unwelcome workload with the CCG staff and that formal piloting of a questionnaire on this scale would be difficult. Therefore, continuous review of the responses was undertaken throughout the data collection, and adjustments to the FOI request were made as necessary (figure 1).
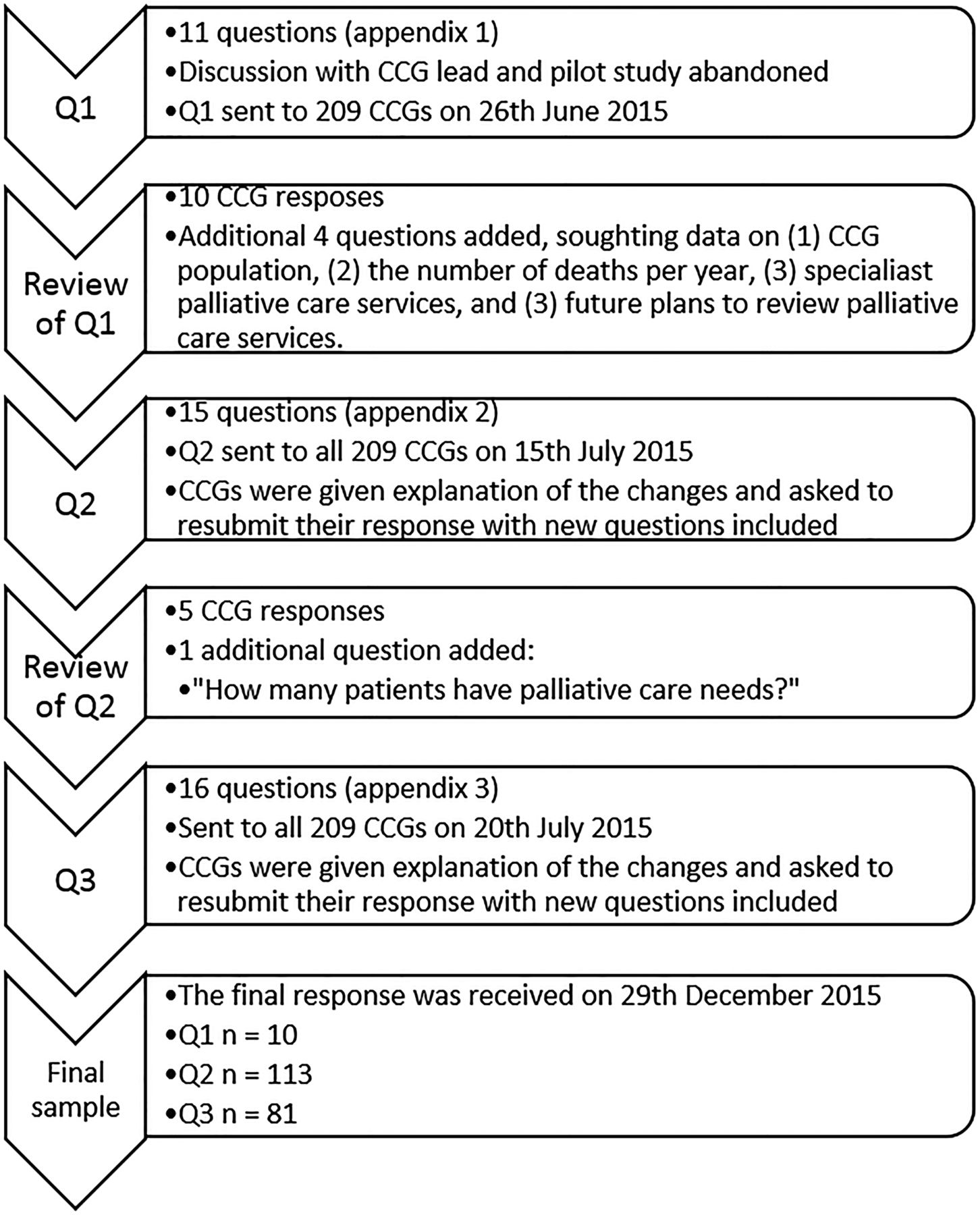
Schematic diagram showing methodology of data collection exercise. CCG, Clinical Commissioning Group; Q1, questionnaire 1; Q2, questionnaire 2; Q3, questionnaire 3.
An initial questionnaire, composed of 11 open-ended questions, was constructed and sent to the FOI department of all 209 CCGs on 26 June 2015 (see online supplementary appendix 1).12 After review of the first 10 responses, Questionnaire 2 (see online supplementary appendix 2) was developed, containing 4 additional questions from topic areas that would benefit from data collection, and sent to all CCGs on 15 July 2015, notifying them of the changes made and requesting their resubmission to include all new questions. A final question was added to the questionnaire and this final version (Questionnaire 3/online supplementary appendix 3) was sent to all 209 CCGs on 20 July, detailing the changes that had been made and again requesting resubmission (figure 1). FOI respondents are administrative staff who report on data held by the CCG and may consult with clinicians if they need to; it is beyond the scope of this study to take into account the differing levels of seniority of the administrative staff. The questionnaire included a definition of specialist palliative care to be used by the CCG when answering the FOI request (see online supplementary appendix 4).
supplementary appendix
supplementary appendix
supplementary appendix
supplementary appendix
The questions in the FOI request addressed seven key themes, as shown in online supplementary appendix 3:
CCG population size and their assessment of palliative care needs
Allocated specialist and generalist palliative care budgets
Number of specialist palliative care beds
Provision of specialist palliative care out-of-hours services
Provision of specialist palliative care support teams
Education and training in specialist palliative care provision
Future plans for specialist palliative care services
Data collection and analysis
FOI request responses were received over the period 8 July 2015 to 29 December 2015. FOI request regulations state that a response must be provided within 20 working days; therefore, after this period, CCGs which had not responded were sent a reminder. A final reminder was sent to all unresponsive CCGs on 30 November 2015.
In total, 204 CCGs responded. Ten provided a response based only on Questionnaire 1, 113 responded to Questionnaire 2 and 81 responded to the final Questionnaire 3. This was to be expected after we decided to undertake a method of continuous review; therefore, the response rates we have calculated for each question in the Results section of this paper take into account the questionnaire used by the CCG and the total number of responding CCGs for that question. We feel this is the best way to analyse our data fairly.
CCGs were contacted via email throughout the study and data were collated using Microsoft Excel onto one central spread sheet by JD and MD. Answers were summarised, abbreviated or translated into usable data as needed at the discretion of the author (ie, budget information was translated into one quantitative figure for analysis), and all data were verified before analysis by the lead author (HL). The amount of information collected was greater than anticipated; therefore, data pertinent to each of the themes outlined were used to carry out a basic descriptive analysis.
The following Microsoft Excel descriptive statistics were used to analyse the data for each of the themes outlined above.
Themes 4, 5, 6 and 7 used sum and percentage formulae only; themes 1, 2 and 3 used minimum, maximum, median, quartiles, mean, sum and correlation coefficient formulae. The box and whisker plot created for theme 2 was constructed using BoxPlotR online tool.13 Correlation coefficients were interpreted using Mukaka's ‘Rule of Thumb for Interpreting the Size of a Correlation Coefficient’.14
Data benchmarking
Where CCGs were unable to provide information about the population size of their area, the unweighted populations published by NHS England in 2014 were used (uplifted by Office for National Statistics (ONS) for population growth).15
The Welsh Palliative Care Strategy 2008 funding formula states that 1 bed (actual bed or hospice at home virtual bed) per 15 000 population should be dedicated to specialist palliative care needs. This figure was used to draw comparisons between the number of specialist palliative care beds provided by Welsh Health Boards and English CCGs for their populations.10
It was important to correlate the data collected with the number of people within each CCG population with palliative care needs. However, the response rate to this question on our FOI was low. Therefore, we estimated that 0.75% of a population will have palliative care needs at any one time, and this was used as a benchmark throughout the data analysis. This figure is in accordance with Murtagh et al,16 Gómez-Batiste et al 17 and Marie Curie's End of Life Care Atlas (from 2011–2012 data).18
Results
The results have been grouped into the themes of the questionnaire, as outlined in Methods and online supplementary appendix 3.
Population size and palliative care needs under the CCG
(Questionnaire 2 and 3) (Q2 and Q3 only)
We asked CCGs to provide information about the size of the population they served and an estimate of the palliative care needs of that population.
Population
One hundred and seventy-nine CCGs (92.27% of respondents to Q2 and Q3) provided information about the size of the population they covered. The data showed a wide range from 73 000 people up to 915 000.
Number of deaths per year
Sixty-seven CCGs (34.54% of respondents to Q2 and Q3) held information on the total number of deaths per year in their population. Fifty-two CCGs also classified these deaths by age-group. On average, 98.92% were adult (aged 18 and above), 0.61% were child and 0.62% were neonatal deaths.
Populations with palliative care needs
(Questionnaire 3 only) (Q3 only)
Twenty-nine CCGs (35.80% of respondents to Q3) held information about the number of patients with palliative care needs in the population they serve. These data showed that on average, 0.43% of the population at any one time will have palliative care needs, with a range of 0.10–1.28%, and a median of 0.31%, as estimated by CCGs.
Specialist palliative care services commissioned
(Q2 and Q3 only)
One hundred and eighty-nine CCGs (97.42% of respondents to Q2 and Q3) provided qualitative data about the services they commissioned. Table 1 summarises the number of CCGs which recorded providing a specific palliative care service in their response.
Type of service commissioned
Specialist palliative care professionals
Forty-eight CCGs (24.53% of all respondents) provided information about the specialist palliative care consultants, nurses and allied health professionals they commissioned.
Thirty-eight CCGs provided specific information about the number of hours worked by these professionals in the form of a whole time equivalent (WTE) (figure 2).
The correlation coefficient for the WTE commissioned by specialist palliative care professionals and the estimated palliative care needs of the population is 0.12. Together with figure 2, this indicates a negligible correlation.14

Scatter graph showing total work time equivalent of all specialist palliative care practitioners commissioned by the Clinical Commissioning Group (CCG) each week, compared with the estimated number of people with palliative care needs in the CCG (0.75%×population). Linear trend line is indicated with a dotted line (n=39).
Specialist palliative care services in a community setting
(Q2 and Q3 only)
One hundred and eighty-seven CCGs (96.40% of respondents to Q2 and Q3) reported that they commissioned specialist palliative care services in a community setting with large variation in the services they provided.
Budget
We asked CCGs about the budget they have dedicated to specialist palliative care services and general palliative and end-of-life care services for the financial year 2015–2016.
One hundred and forty-two CCGs (69.61% of all respondents) provided quantitative data on their specialist palliative care budgets and 103 CCGs (50.49% of all respondents) provided quantitative data on their budget for other palliative care or end-of-life services (table 2).
The range of budgets for both categories was very wide. For generalist palliative care, the range could mean a budget difference of up to £6191.65 per patient per year (using our population estimate of 0.75% of population has palliative care needs).
Figure 3 shows the distribution of these budgets.
Only 19 CCGs provided data about their current palliative care needs population and annual specialist palliative care budget. Analysis of these two parameters gave a correlation coefficient of+0.45, indicating a low positive correlation between these parameters.14
Analysis of the data collected on annual Clinical Commissioning Group budgets for palliative care services
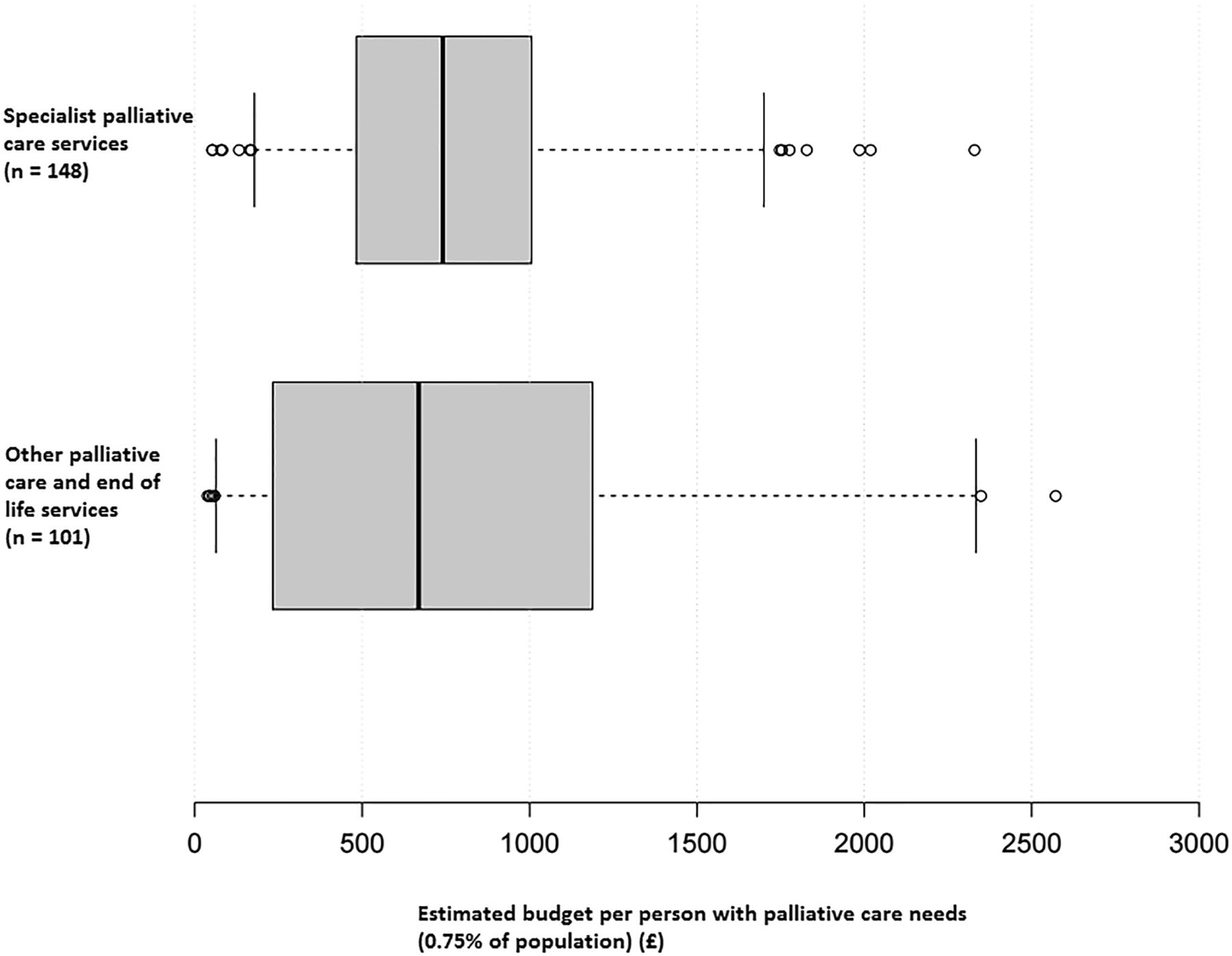
Box and whisker plot showing the estimated budget per person with palliative care needs (using the estimation that 0.75% of the population has palliative care needs) for specialist palliative care services and other palliative care or end-of-life services. One hundred and forty-eight Clinical Commissioning Groups (CCGs) gave data on their specialist palliative care budget and 101 CCGs gave data on their other palliative care or end-of-life care budget. Box and whisker constructed using BoxPlotR.13 In order to display the data more clearly, the following ‘other palliative care and end of life services’ values were excluded from this box and whisker plot: £4232.40, £6107.59, £6229.86 per patient. Whiskers positioned according to Altman (5th and 95th centile).13
Beds
We asked CCGs how many beds they commissioned specifically dedicated to specialist palliative care services, in a variety of care settings, and the access patients have to those beds (table 3).
Analysis of the commissioning of specialist palliative care beds
Number of dedicated specialist palliative care beds commissioned
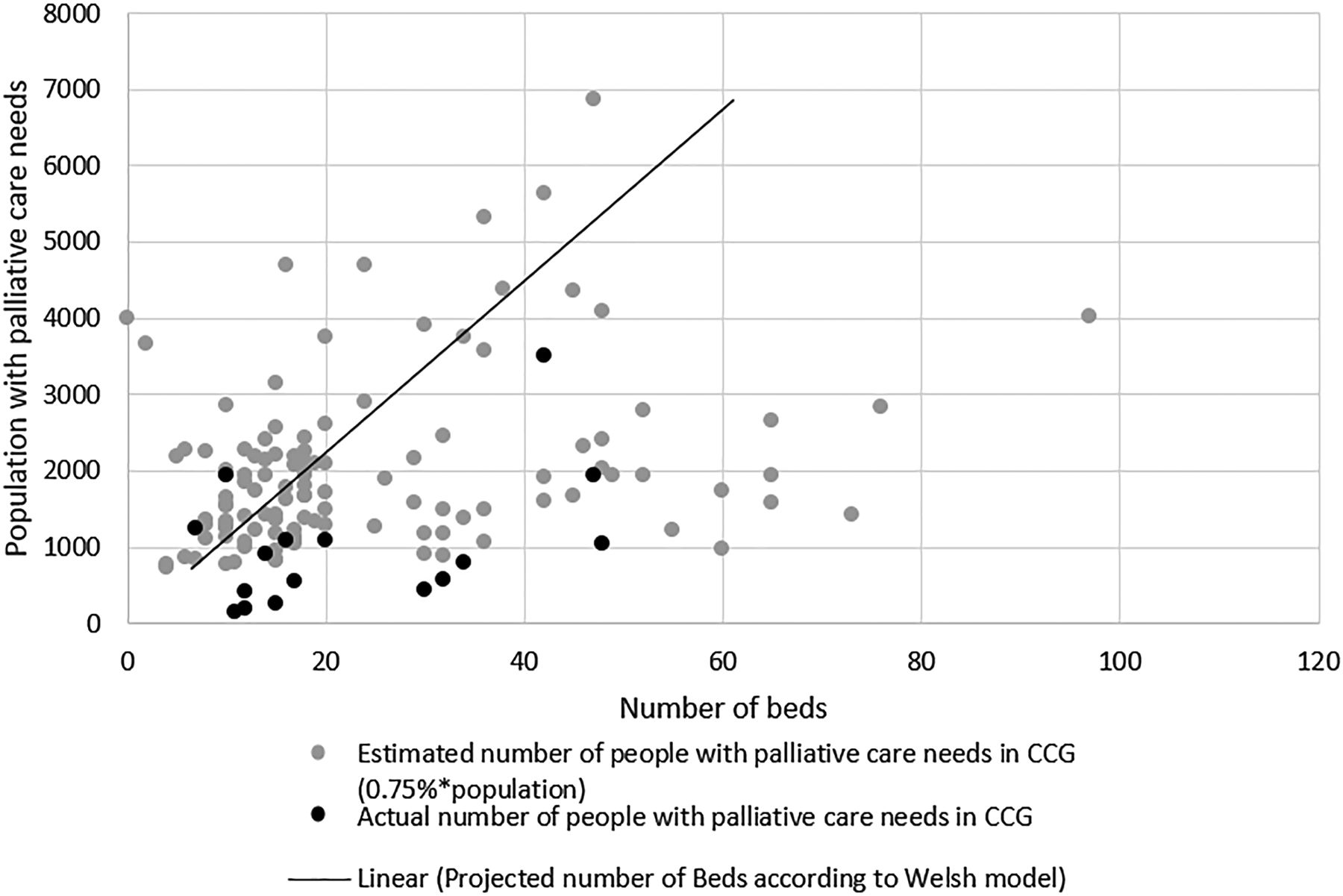
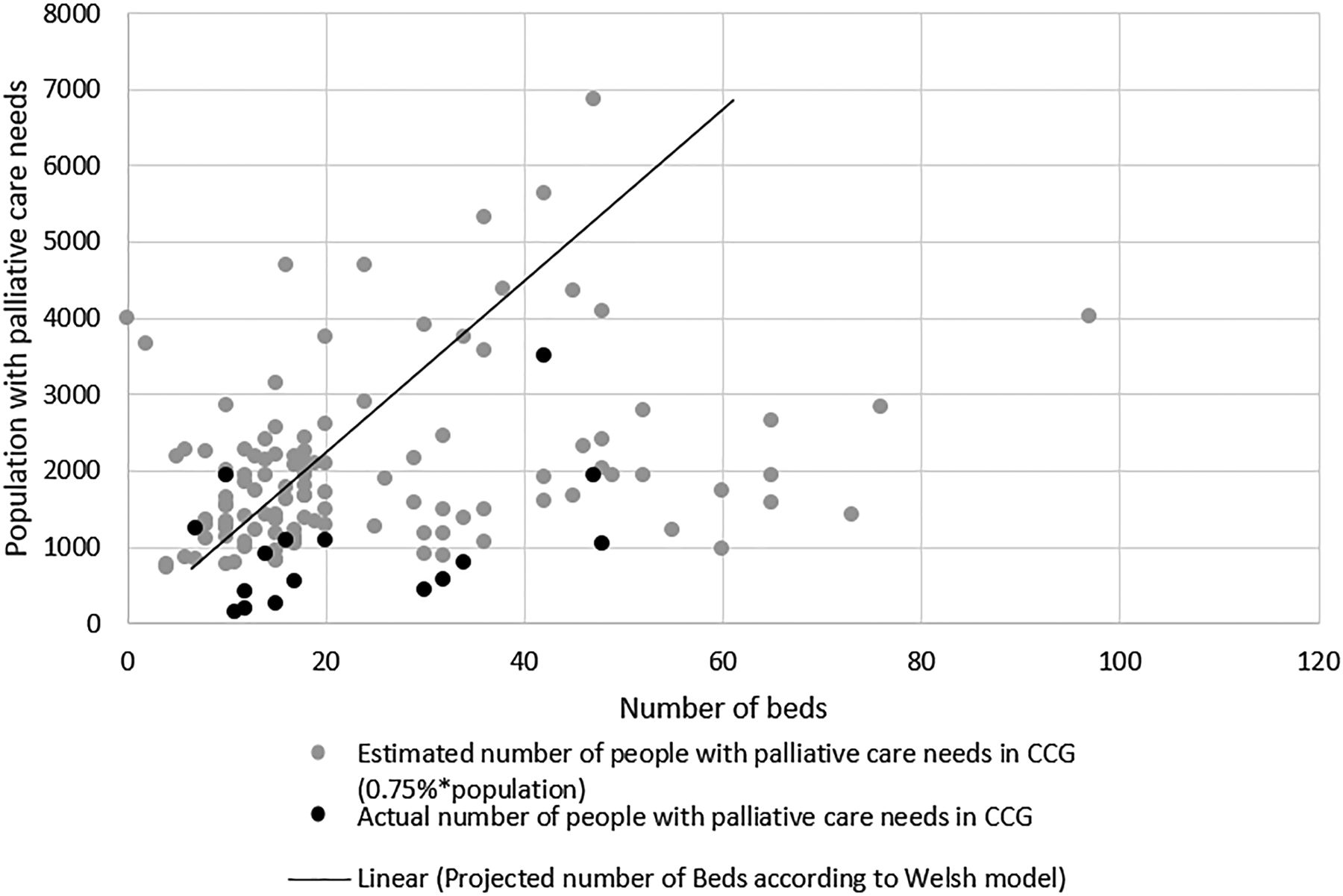
One hundred and twenty-one CCGs (59.31%) provided information about the number of beds they commissioned, of which 115 responses provided usable data for the quantitative analysis in table 3, and figure 4. (The remaining six responses were excluded from analysis as they did not provide quantitative data for these questions, or their response covered more than one CCG area).
Thirteen CCGs (6.37% of all respondents) stated they did not commission dedicated specialist palliative care beds.
Fifty-five CCGs (29.96% of all respondents) declared this information was not held by them.
The average number of beds was 13.58 per 1000 people with palliative care needs in any given area. There was wide variation, with 1 CCG commissioning 61.65 beds per 1000 people and another commissioning 0.55 per 1000 people, a range of 61.10.
The correlation coefficient between the number of beds commissioned and palliative care population is negligible to low at 0.29.14
Figure 4 shows the number of beds commissioned by each CCG and their palliative care needs population. Where CCGs did not provide data on their palliative care needs population, this has been estimated as 0.75% of the population for the CCG (see the Methods section).
Sixty-nine out of 115 CCGs (60%) commission more specialist palliative care beds than the Welsh model would forecast for their population. However, the majority of the CCGs who provided data on their palliative care needs assessment (black plots), actually fell below this benchmark (solid line indicate 1 bed per 15 000) (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatter graph showing the total number of specialist palliative care beds commissioned compared with the estimated number of people with palliative care needs in the Clinical Commissioning Group (0.75%×population) (n=115). A linear trend line has been added to provide a benchmark for the number of beds that should be commission for that population according to the Welsh funding formula.10
Patient accessibility to specialist palliative care beds
Analysis of patient admission to specialist palliative care beds (table 3) shows that 163 CCGs (77.90% of all respondents) commission for 7-day admission to specialist palliative care beds.
According to these data, 74.85% of these beds are from hospices, and between 4.9% and 6.1% of these beds are known to be NHS provided.
We could not draw conclusion about patient accessibility to NHS-funded beds as approximately three-quarters of CCGs responded ‘not applicable’ to this question.
Out-of-hours services
The commissioning of 24/7 specialist palliative care services varied widely.
One hundred and seventy-two CCGs (84.31% of all respondents) reported that they commissioned 7-day access to some form of specialist palliative care, ranging from some CCGs providing a telephone advice line to others providing a 24-hour on-call specialist palliative care team.
One hundred and sixty-nine CCGs (82.84% of all respondents) reported that they commissioned 7-day specialist palliative care services for patients in their own homes. Again, this varied from solely advice lines to dedicated night care teams.
Table 4 shows the most common 7-day services CCGs commission in patients own homes. Hospice-led or hospice-at-home service only was the most common response, followed by a combination of services, most likely hospice or hospice-at-home with community nursing or night-time services.
In addition, 163 CCGs (79.90% of all respondents) reported that they commissioned 24/7 specialist palliative care advice. Of these:
One hundred and twenty-three (75.46%) provided advice from a consultant to all other out-of-hours' healthcare professionals in the area.
One hundred and seventeen (71.78%) provided advice directly to patients and their carers.
Support teams
Hospital support through a specialist palliative care support team or a pain control team was also variable. Sixteen CCGs (7.84% of all respondents) reported that they commission neither type of support to hospital patients.
One hundred and sixty-six CCGs (81.37% of all respondents) reported that they commissioned specialist palliative care support teams in hospitals.
Sixty-four CCGs (31.37% of all respondents) reported that they commissioned 7-day hospital acute pain control team services. However, it was still unclear what services were available out of the usual Monday–Friday, 9:00–17:00 hours. Only 10 CCGs provided details of their services, showing weekend and evening services were predominantly on-call consultants or telephone helpline. Fifteen CCGs named acute trusts in their area which were responsible for coordinating support teams and 13 CCGs gave no details.
Analysis of the specialist palliative care services commissioned in patients own home
Education
We asked CCGs what educational support they commission for specialist palliative care services.
One hundred and thirty-nine CCGs (68.14% of all respondents) commissioned or named a provider who gave educational support in specialist palliative care. There was variation in the type of educational support that CCGs commission, with some offering a comprehensive package including regular training for GPs and in communication skills, while others provided occasional education days.
Of those 139, 99 CCGs commissioned educational support requiring palliative care specialists to educate other healthcare professionals.
Future
Finally, we asked CCGs if they had plans for any new specialist palliative care services in the future.
(Q2 and Q3 only)
One hundred and eighty-eight CCGs provided details on whether they had any plans in place for the future of their specialist palliative care service.
Of the 188 in this analysis, 101 CCGs had plans for new services, were under review or had a review planned with the scope of implementing developments. These plans were at various stages of development and ranged from the extension of 7-day services to putting systems in place to ensure that each patient has a key worker and access to comprehensive care whenever needed.
Eighty-seven CCGs had no plans for future services.
Discussion
This study was undertaken during preparation of the Private Members Bill, Access to Palliative Care Bill 2015–2016, and was subsequently used to inform debate during the legislative second reading in the House of Lords (23 October 2015).
Although this exercise aimed to provide evidence of the variations in the commissioning of palliative and specialist palliative care services by CCGs, it became apparent that the actual data held by CCGs were also inconsistent—some CCGs provided accurate data on the number of deaths and palliative care needs of their population, but others declared they did not hold such information. CCGs, and in turn their services, may benefit from national guidelines on what baseline information should be used to best commission their healthcare services.
Our most reliable conclusions come from the annual palliative care budget data. There is limited correlation between the palliative care needs of the population and the budget allocated to palliative care services. Although greater spend per patient does not necessarily equal better services, the fluctuating budget per patient provides evidence to support concerns about a ‘postcode lottery’ raised in parliamentary debates.19 Further work would be needed to assess whether budgets truly reflect the needs of the local population, and how CCGs calculate their budget allocations.
The data collected on specialist palliative care beds are encouraging. The majority of CCGs (60%) who provided quantitative data on beds actually commission more specialist palliative care beds than the Welsh model would forecast for their population. Poor patient accessibility to beds has been documented as a problem in a number of reports;1 ,6 ,10 therefore, further work would be needed to determine whether the organisation of these resources may be an underlying problem.
The provision of round-the-clock access to specialist palliative care and pain control is inconsistent. While some of the data we collected are encouraging, the variation in services means that some areas are only served by a basic out-of-hours service such as a telephone line that does not involve consultant advice; while others are supported by dedicated night-time services and support networks. Further work would be needed to fully understand areas which are struggling due to staffing shortages.
The PHSO's report has shown how essential it is that educational training is provided to all staff involved in care of the dying. Our data suggest that the type of training provided to healthcare professionals on palliative care may be inconsistent, but it is not clear whether this contributes to the variation in service level.
Our data suggests that only half of those who responded are committed to improving their services in the future. There is currently no national initiative in place to monitor how often services are reviewed, or to support CCGs in developing their services and sharing best practice.
The information obtained in this FOI exercise reflects some of the key failures identified in the PHSO's report, and has also highlighted the need for CCGs to hold standard data on the healthcare needs and service provision across their population.
Limitations
The most important finding from this exercise is that information is not standardised, is poorly defined and therefore very difficult to interpret. Our data were also collected via an open questionnaire, which meant the responses were of varying length and detail, and did not always provide the quantitative parameter needed for analysis. In addition, the low response rate on some of our questions resulted in a small sample size. In particular, the low response rate to our question on the palliative care needs population size, led us to use 0.75% as a reliable benchmark figure throughout our analysis. It is important to acknowledge that the palliative care needs population will vary across the country, and this figure will not truly represent the needs of every CCG's population.
Conclusions
This study goes some way to provide evidence that while there is excellent specialist palliative care provision in parts of England, there is a vast degree of variation across the country and across different services. Most strikingly, there is little uniformity in the data CCGs are required to hold, and disparity in the responsibility of service provision between CCGs, Trusts and local hospices. As a result, a paucity of services means that patient choice at the end of life cannot always be honoured and unless national guidelines are put in place to support CCGs in commissioning care, the deficits described in the PHSO's report will not be addressed.
Palliative care needs to be available at all times because crises often occur out of hours. In Wales, specialist staffing levels have been determined within the available funding, and a dedicated number of palliative care beds ensures fair access to specialist palliative care across 7 days. This model provides a starting point for CCGs to benchmark and improve provision for their population.
Our data reveal that the devolution of decision-making down to CCGs suggests that palliative care provision is not being considered as a core service in some parts of England. Despite much evidence of its cost efficacy,20–22 the provision of specialist palliative care is in need of a national framework to ensure that patients achieve good end-of-life care everywhere.
Acknowledgments
The authors would like to thank all the CCGs who completed the FOI request and provided data for this data collection.
Supplementary materials
Press Release
Files in this Data Supplement:
Footnotes
Contributors MD and BIF designed the FOI request and study. MD and JD communicated with all CCGs and undertook preliminary data entry. HL entered data, checked all data entry for consistency, analysed the data and led writing of the paper at all stages. BIF discussed the possibility of piloting, oversaw the process, checked calculations based on the data and edited all drafts of the paper.
Funding The FOI request incurred no cost. All funding for analysis and writing was provided by IF.
Competing interests BIF wrote and introduced the Private Members' Bill the Access to Palliative Care Bill to the House of Lords in 2015–2016. HL is currently employed as Parliamentary Researcher to BIF, MD and JD have previously been employed as Parliamentary Researchers to BIF.
Ethics approval As the Freedom of Information Act was used to request data and no person identifiable data were sought, there were no aspects to this survey requiring ethics committee approval. All CCGs were notified of our plan to publish the study findings, and all data have been reported anonymously in our analysis.
Provenance and peer review Not commissioned; externally peer reviewed.