Article Text

Abstract
Objective Despite the importance of parenting-related responsibilities for adult patients with terminal illnesses who have dependent children, little is known about the psychological concerns of dying parents and their families at the end of life (EOL). The aim of this study was to elicit widowed fathers’ perspectives on how parental status may have influenced the EOL experiences of mothers with advanced cancer.
Subjects 344 men identified themselves through an open-access educational website as widowed fathers who had lost a spouse to cancer and were raising dependent children.
Methods Participants completed a web-based survey about their wife's EOL experience and cancer history, and their own depression (Center for Epidemiologic Studies Depression Scale, CES-D) and bereavement (Texas Revised Inventory of Grief, TRIG) symptoms. Descriptive statistics, Fisher's exact tests, and linear regression modelling were used to evaluate relationships between variables.
Results According to fathers, 38% of mothers had not said goodbye to their children before death and 26% were not at all ‘at peace with dying.’ Ninety per cent of widowed fathers reported that their spouse was worried about the strain on their children at the EOL. Fathers who reported clearer prognostic communication between wife and physician had lower CES-D and TRIG scores.
Conclusions To improve EOL care for seriously ill patients and their families, we must understand the concerns of parents with dependent children. These data underscore the importance of parenting-related worries in this population and the need for additional clinical and research programmes devoted to addressing these issues.
- Family management
- Cancer
- Bereavement
- Terminal care
Statistics from Altmetric.com
Background
Cancer is the leading cause of death for women aged 25–54 in the USA, the peak parenting years.1 Although rarely addressed by healthcare professionals, parenting concerns and responsibilities are of high importance to many patients with advanced cancer who have dependent children.2 Despite the impact of parental cancer and early parental death on families, there is a dearth of research on how parental status can impact the experience of cancer at the end of life (EOL) for patients and their families.
Parents with advanced cancer experience challenges when coping with a life-limiting illness that differ from non-parents. Prior research suggests that parents with advanced cancer who have dependent children may be less likely to acknowledge the terminal nature of their illness and more likely to choose treatment focused on life extension rather than to pursue palliative options.3 Another study has demonstrated that parents with metastatic cancer experience high rates of anxiety and depressive symptoms and that parenting concerns are correlated with these mood symptoms.4 ,5 The few qualitative studies of advanced cancer and parenting suggest that parents struggle with adaptation to incurable illness,6 ,7 concerns about the impact of their disease on children6 and the challenges of being a ‘good parent.’8 ,9
Several lines of evidence suggest that dying parents’ concerns about their family's coping are well founded. Co-parents who care for their terminally ill spouses are more likely than non-parents to experience symptoms of major depression and generalised anxiety.3 ,10 ,11 Following death, the surviving parent struggles with isolation, parental competence and maintaining family roles.11 ,12 ,13 Similarly, children of terminally ill parents are at elevated risk of developing depressive disorders during the periods of parental advanced illness and bereavement.14 ,15 Existing data suggest that the quality of parenting by the surviving parent is associated with children's psychosocial functioning and that positive parenting leads to improved adjustment of the bereaved child.16 ,17 Therefore, research that helps us to understand how families transition from parental illness through bereavement may be particularly useful.
Many parents with advanced cancer struggle to balance their roles as a parent and terminally ill patient,7 yet very little is known about their EOL concerns and dying experiences. Bereaved spouses’ perspectives on patients’ EOL experiences are rarely solicited and can provide important insights into the psychological concerns and dying experiences of parents with advanced cancer when direct assessment from the ill patient is neither possible nor practical.18 Additionally, perceptions of EOL care by bereaved caregivers may contribute to their development of complicated grief and other adverse mental health outcomes.19
The goals for this exploratory study were to: (1) better understand widowed fathers’ perspectives on how being a parent affected the EOL experiences of their wives with advanced cancer, and (2) identify possible relationships between these EOL experiences and bereaved fathers’ depression and bereavement symptoms. By focusing on the mother's concerns and treatment decision-making at the EOL, as reported by the husband, we hope to improve our understanding of how to optimise the EOL care for parents with advanced cancer and their families. We hypothesised that widowed fathers would report high degrees of maternal parental concerns at the EOL. We also hypothesised that widowed fathers’ negative perceptions of their wife's EOL experience and absence of hospice care would be associated with higher paternal depression and bereavement scores.
Methods
Study design and sample
We conducted an online survey of fathers following the death of their children's mother through an open-access educational website for widowed fathers due to cancer (http://www.singlefathersduetocancer.org). This survey was available to all individuals who visited the website and self-identified as a father of one or more biological or adopted children currently under the age of 18 whose mother died from cancer. Most widowed fathers due to cancer are not regularly in contact with cancer care providers and institutions after the death of their loved one, therefore a broad outreach strategy was employed to inform potential participants about the online educational resource. The website and survey were advertised through word-of-mouth among cancer support professionals and through print, television and radio media.20–22 The educational website contains written and video vignette information about coping with bereavement (for fathers and their children), common experiences related to single fatherhood, and resources for parents and professional providers. Suggested resources included books written by widowed fathers about their experiences, more general information about widowhood, and information about single fathers support groups. Website content was specifically developed for widowed fathers because cancer is the leading cause of widowed father-led families in the USA23 and due to concerns that widowed fathers may experience worse psychological outcomes than widowed mothers and potentially benefit from targeted interventions such as an online resource and support groups.24
Data were collected between October 2012 and December 2014. Owing to the small number of men who were not married to the mother of their children at the time of her death, the analysis was restricted to married men. The analysis was also restricted to men whose wife died within 5 years of completing the survey in order to focus on recently bereaved widows. Informed consent was obtained prior to start of the survey, which was approved by the University of North Carolina (UNC) at Chapel Hill Institutional Review Board.
Survey
Description of participants and details about the development of the survey have been previously reported.11 Fathers were asked questions regarding their current symptoms of depression (Center for Epidemiologic Studies Depression Scale; CES-D)25 and bereavement (Texas Revised Inventory of Grief; TRIG);26 sociodemographic characteristics; psychological adaptation (Psychological Adaptation Scale);27 and parenting self-efficacy (Kansas Parenting Satisfaction Scale28 and an investigator-designed, 12-item assessment of widowed parenting self-efficacy). The survey included multiple questions about their wife's cancer history and EOL experience, such as location of death, presence or absence of hospice and prognostic awareness. Additionally, the fathers were asked 13 questions specifically about her psychological and parenting concerns at the EOL. These EOL queries were presented as statements with a four-point ordinal response scale (0=‘not true at all’ to 3=‘very true’). Phenomena such as ‘saying goodbye’ and ‘feeling strain’ at the EOL are often more nuanced experiences than can be captured by a forced true/false choice, and for that reason we used a four-point scale. Investigator-designed questions were developed for this study and were based on the authors’ clinical experience and subsequently pilot tested with recently widowed men who had lost a spouse to cancer and were fathers of young children.
All data were collected online using Qualtrics software (Qualtrics, LLC, Provo, Utah, USA).
Data analysis
Descriptive statistics were employed to characterise the sample of widowed fathers and their wives, including frequency distributions, means, ranges and SDs as appropriate. Fisher's exact tests were used to evaluate associations between mother's parenting concerns at EOL and other EOL characteristics (eg, hospice and peace with dying). Separate linear regression models were fit to evaluate the associations between mother's EOL characteristics and father's CES-D and TRIG scores. Only respondents who completed all questions on the CES-D were included in final analyses. Time since wife's death (<6, 6–12, 12–24, >24 months) was included as a covariate in all regression analyses to control for possible differences in father's CES-D and TRIG scores based on time. Given the exploratory nature of this study, no other covariates were included in regression analyses.
Data for this study came from a larger study evaluating bereavement outcomes of widowed fathers based on time since death. Since then, additional respondents have completed the survey but did not significantly differ from the original sample on sociodemographic or maternal illness characteristics or CES-D or TRIG scores.13 Of 420 survey responders, 76 were excluded from further analyses for the following reasons: 17 reported having no children under 18 at the time of death, 52 completed the survey more than 5 years after the time of death, and 7 since they were not married at the time of death. Unmarried men were excluded from the final sample due to their low numbers and because of prior research suggesting worse bereavement outcomes in spouses than other adult family caregivers.29
All analyses were performed using SAS V.9.3 (SAS Institute, Inc, Cary, North Carolina, USA). All p values were derived from two-sided statistical tests.
Results
Respondent and patient characteristics
A total of 344 self-identified married fathers of dependent children at the time of their wives’ deaths completed the survey within 5 years of their wives’ death. Mean time between death of spouse and survey completion was 1.3 (SD, 1.3) years. Three quarters of the sample (n=261, 77%) completed the survey within 2 years of their wife's death. Mean age of respondents was 46.4 (SD, 7.3) years. Eighty-nine per cent (n=276) were Caucasian and nearly three quarters of the sample (n=238, 74%) had a college degree or higher. Additional sociodemographic details are described elsewhere.11 Respondents’ mean CES-D score (n=291) was 23.9 (SD, 12.5), with 71% (n=206) exceeding the screening threshold criteria (score≥16) for major depressive disorder in community samples.30 The mean score on the TRIG-A (assessing bereavement symptoms at the time of death of the loved one) was 24.2 (SD 5.8). The mean score for the TRIG-B (assessing current bereavement symptoms) was 46.1 (SD 9.4).
Mothers’ characteristics are summarised in table 1. Mother's mean age at time of death was 43.7 (SD, 7.1) years. The most common type of cancer was breast cancer (n=125, 36%). Hospice services were involved for two-thirds of the women (n=231, 67%).
Mother characteristics
Characteristics of mother's dying experience
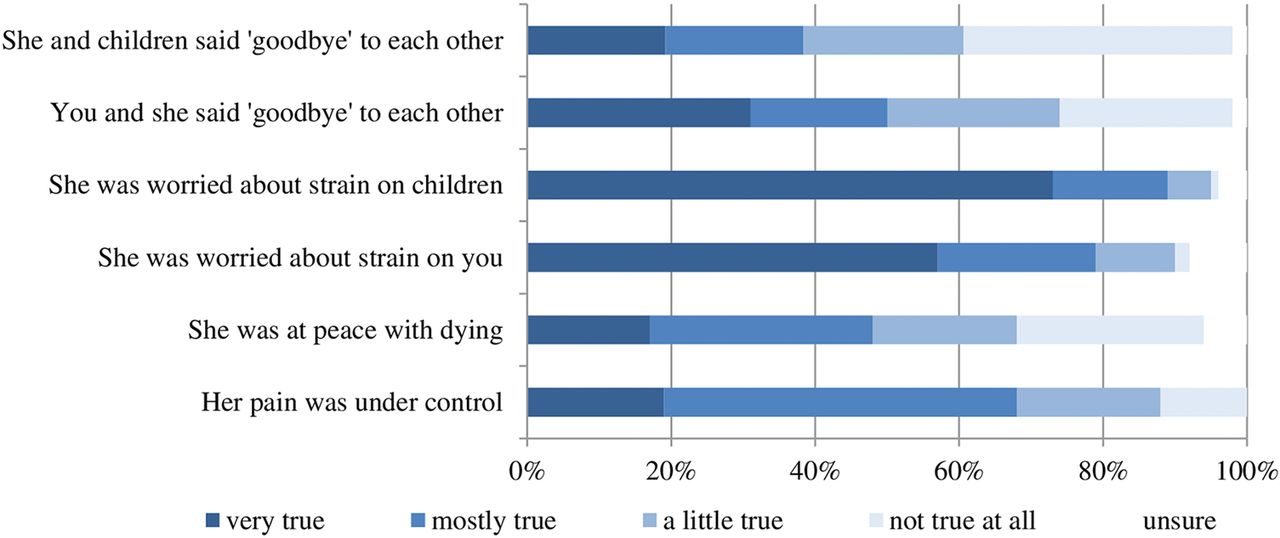
According to the fathers, most mothers experienced substantial worry about their family at the end of their lives (figure 1). Over three quarters of the fathers (n=269, 78%) stated that it was ‘very’ or ‘mostly’ true that their wives were worried about the strain on him at the EOL. Nearly 90% (n=307) of the respondents stated it was ‘very’ or ‘mostly’ true that their wives were worried about the strain on their children. Slightly less than half of the sample reported it was ‘very’ or ‘mostly’ true that their wife was ‘at peace with dying’ during the final weeks of life (n=165, 48%). Mothers who received hospice services were significantly more likely to be described by their spouses as being at peace with dying (77% vs 62% p=0.006). Widowed fathers who believed their wife's physician was clear with her about her prognosis were also more likely to describe their wives as being at peace with dying (78% vs 57%, p<0.0001) compared to those who were unclear or never discussed her prognosis. In contrast to their wife's psychological distress, fathers mostly described her as physically comfortable at the EOL, with two-thirds of fathers (n=232, 68%) reporting that it was ‘very’ or ‘mostly’ true that her pain was under control in the final weeks of life.

Mothers’ EOL characteristics as reported by widowed fathers. EOL, end-of-life; CES-D, Center for Epidemiologic Studies Depression Scale.
Influence of maternal role on decision-making
When asked about the influence of the parental role on their wife's advanced cancer treatment decision-making, nearly a quarter of the sample (n=83, 24%) reported that their wives’ decision-making was ‘almost totally’ impacted by being a mother. An additional 16% (n=56) said it moderately impacted her decisions, and 20% (n=67) reported parental status was a small impact. Of the 206 respondents who said their wives’ treatment decisions were influenced by being a mother (either a small amount, moderate amount, or almost totally), 64% (n=132) of them reported that her treatment choices were more aggressive due to being a mother. Only 16 men (8%) believed that their wives opted for less aggressive treatment because of having dependent children. Despite the importance of the parental role in their wife's treatment decision-making, only half of the sample (n=104, 51%) believed that her physician ‘completely’ understood this. There were no significant associations between a father's report of how maternal status influenced his wife's treatment decision-making and his own depression and bereavement scores.
Preparation for death
Only half of the widowed fathers reported that they and their wives had said goodbye to each other in the final weeks of life (n=171, 50%, figure 1). A smaller percentage (n=132, 39%) believed that their wife and children had said goodbye to each other and over a third (n=127, 37%) of men reported that saying goodbye to the children was ‘not true at all’ for their wife.
Fathers whose wife received hospice services were more likely to report that they had said goodbye to each other before her death (83% vs 61%, p<0.001). They were also far more likely to report that their wife and children had said goodbye (73% vs 40%, p<0.001). Father's reports of clearer prognostic communication between physicians and wife (how clear do you feel doctors were with her about her prognosis: completely/mostly clear vs not at all/never told) were also associated with having said goodbye to spouse (79% vs 65%, p=0.014) and children (66% vs 50%, p=0.01).
Associations between mother's dying characteristics and father's depression and bereavement
There were no significant relationships between a mother's participation in hospice services or having died at her preferred location with the father's CES-D and TRIG scores. Table 2 demonstrates the univariable analyses between mother's EOL characteristics and father's CES-D and TRIG scores, after controlling for time from mother's death to survey completion. All of the mother's EOL characteristics, except for having said goodbye to her children, were significantly associated with either the father's CES-D or TRIG scores in univariable analyses (see table 2). Multivariable regressions for CES-D, TRIG-A and TRIG-B were also performed but no individual maternal EOL characteristic was predominantly predictive of father's depression and bereavement scores.
Linear regression model results for mother's EOL characteristics and father's CES-D, TRIG-A, and TRIG-B scores*
In univariable analyses, men who believed it was more true that their wife was ‘at peace with dying’ reported lower depression and bereavement scores (see figure 2). With each increasing level of agreement regarding peacefulness, fathers’ CES-D scores decreased by an average of 1.68 points (p=0.02). Similarly, with each level of agreement about peacefulness, TRIG-B scores also decreased (p<0.001).
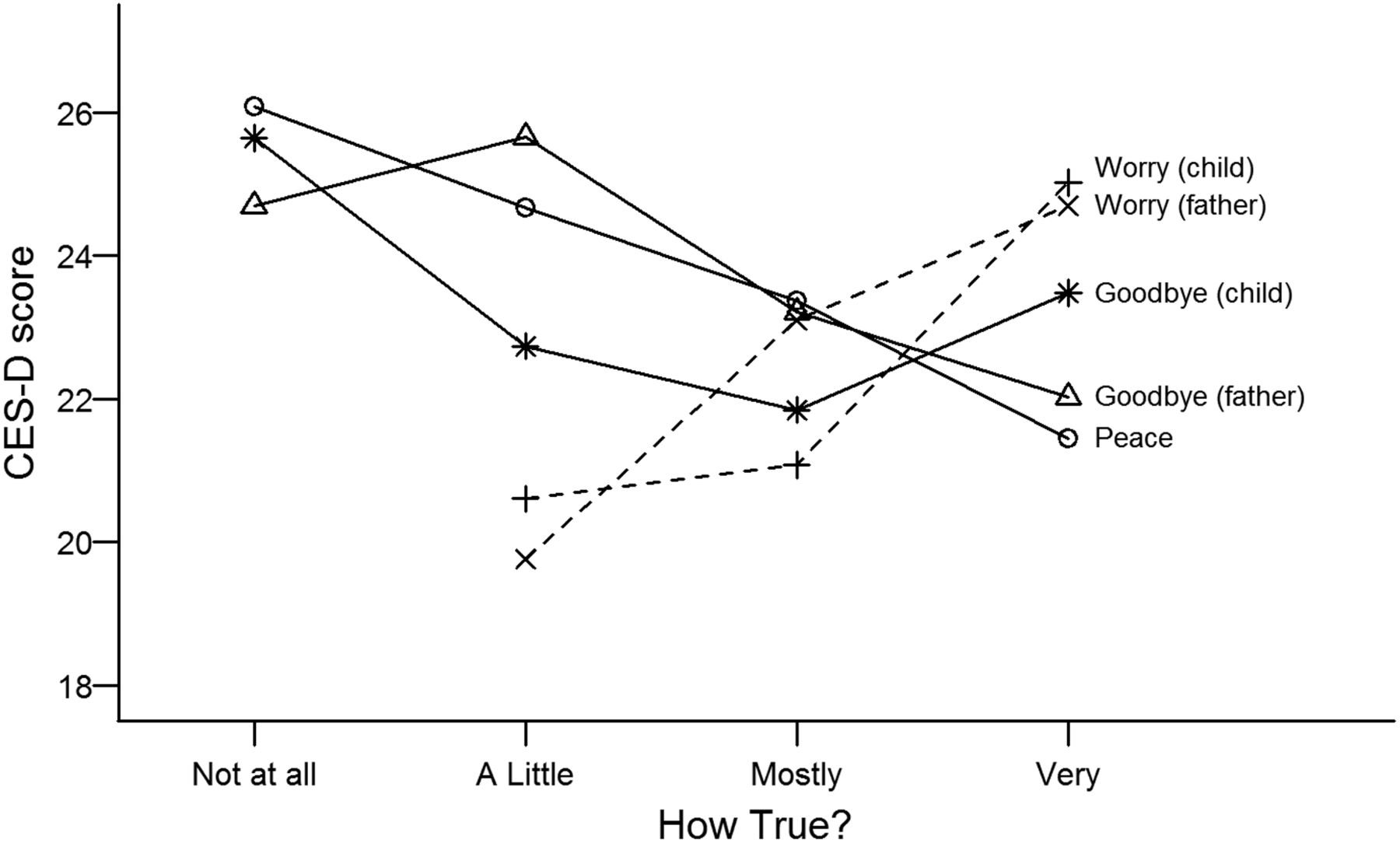
Relationships between mother's EOL characteristics and father's CES-D scores*. EOL, end-of-life; CES-D, Center for Epidemiologic Studies Depression Scale. *The following data points for ‘not at all’ are not shown due to low n: worry (father) n=8; worry (child) n=1.
Men who reported that their wife's physician was ‘completely’ or ‘mostly’ clear with her about prognosis had, on average, a six-point lower score on the CES-D (22.7, SD, 12.3) as compared to those who reported that her physician was ‘not very’ or ‘not at all’ clear (28.6, SD, 12.1) (p=0.003) (see figure 3). A relationship was not found for fathers’ bereavement scores and reported physician prognostic clarity.

{kind=link}
{kind=link}
{kind=link}
Physician's clarity about death and father's CES-D scores. CES-D, Center for Epidemiologic Studies Depression Scale.
Father's report that it was true that he and his wife said goodbye before her death was associated with a small decrease in his CES-D scores (p=0.05) and his report of maternal worry about their children was associated with both his depression and bereavement scores. For each level of father's report of maternal worry, father's CES-D scores increased 3.0 points (p=0.017), TRIG-A scores increased by 1.6 points (p=0.012), and TRIG-B scores by 2.8 points (p=0.006) (figure 2).
Conclusions
Parents dying with cancer are an under-examined population despite high levels of distress among these individuals and the far-reaching consequences of early parental loss for bereaved families. These patients have unique concerns at the EOL and their parental status may influence their dying experience in important ways.3 Additionally, widowed partners must grieve their own loss while simultaneously addressing the bereavement and parenting needs of their children.10 ,13 ,23
Information from widowed fathers suggests that at the EOL, mothers with cancer experienced substantial worries about their family and low levels of peacefulness. These results indicate that additional clinical programmes and studies are needed to address the unresolved psychological distress of dying parents at the EOL. In addition, according to the surviving fathers, many of the women described in our sample had not said goodbye to their spouses and the majority did not say goodbye to their children. The inability to say goodbye is noteworthy because of the importance that families, patients and healthcare providers place on life completion as a component of a good death. Research by Steinhauser et al31 has demonstrated that the opportunity to say goodbye to important people is consistently valued among patients and their family members at the EOL.
Although these findings cannot demonstrate causality, they do suggest that worry at the EOL, unresolved tasks associated with life completion, and unclear prognostic communication between ill mothers and their physicians are positively correlated with depression scores of widowed fathers with dependent children. Identifying EOL variables that influence father's depression symptoms are particularly important given the relationship of the surviving parent's well-being and parenting style with their parentally bereaved children's psychological adjustment.32 Our results are consistent with prior research, which has demonstrated an association between complicated grief among bereaved caregivers and their perception that their loved one did not achieve a sense of completion about his or her life.19 Similarly, research from the Coping with Cancer study found that the perception of patient suffering is associated with poorer bereaved caregivers’ mental health.33
A larger percentage of mothers described in this sample received hospice services at the EOL, as compared to the national average of 44.6%.34 In this study, fathers whose wife received hospice services were more likely to report that their wife was at peace with dying and that she said goodbye to her spouse and children. While this study does not demonstrate causality, these results suggest a positive relationship between receipt of hospice services and improved EOL experiences for mothers with advanced cancer. We did not find an expected relationship between maternal participation in hospice care and lower measures of fathers’ depression and bereavement. However, we did not collect data on the duration of hospice use. Very brief hospice utilisation may not be associated with measurable improvements in depression and bereavement scores of surviving spouses with dependent children. A study by Bradley et al35 found higher rates of major depression in surviving caregivers when the ill patient was enrolled in hospice for less than 3 days as compared to caregivers of patients with longer hospice enrollment. Other studies have demonstrated greater caregiver benefit with longer lengths of stay in hospice.36 ,37
Parental status may also influence advanced cancer treatment decision-making. Nearly a quarter of widowed fathers reported that their wife's decisions about treatment were ‘almost totally’ impacted by being a mother. The influence of parental status on advanced cancer treatment decision-making has been understudied despite the potential impact this may have on cancer and EOL outcomes.3 This study was not designed to specifically evaluate this issue, but for at least a subset of these parents, parental status was motivation to seek an aggressive course of cancer treatment. Widowed fathers’ assessment of mother's advanced cancer treatment preferences were not associated with their own grief or depression outcomes, but future prospective studies of this phenomenon may provide a more nuanced understanding of potential relationships between patient's treatment decision-making for advanced cancer and bereavement outcomes of surviving family members.
Owing to the open-access nature of this web-based survey, we could not confirm whether men who completed the survey met eligibility criteria. A related limitation concerns the representativeness of this sample. Respondents were a group of men with relatively high levels of education and income, were predominantly Caucasian, and married to their children's mother at the time of her death. Further, it is possible that widowed fathers who found the website and took the survey were more likely to be distressed about their wife's EOL experiences than typical widowed spouses or that exposure to informational content about depression and bereavement on the website influenced the fathers’ recognition or reporting of depression symptoms. The website itself serves as an intervention for these at-risk fathers and we do not know how interactions with the website may have influenced their reporting of their wife's EOL experiences or their own psychological symptoms. The average CES-D score of our respondents is consistent with ‘probable’ depression,38 and it is possible that depressive symptoms may influence their reporting of their wife's dying experience through recall bias. Depression itself is associated with biases in attention and memory and these cognitive processes may lead to increased propensity to recall negative life events.39 In turn, these cognitive biases may contribute to negative perceptions of their communication with their wife or encounters with her oncologist. It should also be noted that the information learned about mothers’ dying experiences was provided by their spouse, which therefore reflects the perception of concerns and experiences of these mothers, rather than direct ascertainment from the dying parents themselves.
Despite these limitations, these findings suggest a need for further exploration of the influence of the parental role on the dying experience of terminally ill patients with cancer. The complex experiences of parents with advanced cancer support the need for qualitative studies providing in-depth analyses of these processes.7 Further studies that utilise prospective assessment of patients, caregivers and their providers may also help build a framework for how and when parental status impacts treatment decision-making, ability to prepare for death, and EOL concerns. Studies that incorporate other models of data collection, such as face-to-face interviews, are also needed as these may reveal differential responses as well as a more diverse participant population. In addition, as this study only reported on the experiences of mothers with advanced cancer, future research that incorporates ill fathers and mothers, as well as those with other life-limiting illnesses, would provide greater understanding of these phenomena.
In summary, families affected by the premature death of a parent due to cancer face serious challenges during the period of advanced illness and after death. Widowed fathers’ assessments indicate that the EOL experiences of dying mothers with cancer are in need of substantial improvement. Further research is needed on how to optimise the care of these patients and their families.
Acknowledgments
The authors wish to gratefully acknowledge the caregivers who participated in this study and who gave their time to share their experiences as well as Chai Core for assisting with website design.
References
Footnotes
Contributors EMP, JMY, DLR were responsible for the study concept and design. EMP, JMY, DLR, AMD, TE acquired the data. All authors were involved in the analysis and interpretation of data. EMP drafted the manuscript and all authors revised it critically for important intellectual content. EMP is the guarantor.
Funding The project described was supported by the University Cancer Research Fund of North Carolina and the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Numbers 1UL1TR001111 and 1KL2TR001109. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Competing interests None declared.
Ethics approval University of North Carolina at Chapel Hill Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional unpublished data from the study is available to the primary study team via a secure server.