Article Text

Abstract
Background Research is essential for gathering evidence to inform best practice and clinical decision making, for developing and testing new treatments and services in palliative and end-of-life care (PEoLC). The participation of patients, carers and family members is essential, however, personal and ethical concerns are often cited by professionals as barriers to recruitment. There is evidence that patients and family members can benefit from participation in PEoLC research.
Aim To synthesise the evidence regarding patients’, family members’ and carers’ experiences of participating in PEoLC research. To identify recommendations for enhancing the experience of participants.
Design A qualitative rapid review and thematic synthesis.
Data sources MEDLINE, PsycINFO and PubMed were searched from 2010 to 2020. Studies reporting patients’, family members’ or carers’ experiences of participating in PEoLC research were included.
Results 4 studies were included and 7 themes identified relating to the benefits of, and barriers to, participation in PEoLC research. Both altruistic and personal benefits of participation were reported. Barriers (negative aspects) to participation included feeling overwhelmed, practical issues, reminders of being a patient, not seeing the research as relevant to them and unmet needs.
Conclusions A number of benefits (positive aspects) surround participation in PEoLC research. However, several barriers (negative aspects) can prevent or discourage participation. This review has identified recommendations for research teams to enhance the experience, and number of people who those participating in research in this field.
- methodological research
- supportive care
- terminal care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What was already known?
Recruitment to palliative and end-of-life care (PEoLC) research is challenged by factors including ethical considerations, characteristics of the population and potential gatekeeping. There is limited evidence of the experience of participation from the perspective of patients and their family or carers.
What are the new findings?
A summary of the experience of participation in PEoLC research. An overview of the perceived benefits (positive aspects—altruism and benefits for themselves) and barriers (negative aspects—feeling overwhelmed by the situation, participation not being seen as relevant, practical barriers, reminded of being a patient and unmet needs).
This paper highlights the paucity of research into patient and family members experience of participating in PEoLC. This evidence is needed to ensure that research in this area is designed with the patient at its heart and to minimise burden on participants.
What is their significance?
Clinical
An enhanced experience of participation has the potential to increase the number of people engaging in research at the end of life, potentially reduce research attrition rates and ultimately improve future PEoLC services and intervention.
Research
Recommendations for research teams conducting PEoLC research are provided which could lead to improved engagement and experience of participants research and could assist in the design of future research.
Introduction
Research is essential for the gathering of evidence needed to inform best practice and clinical decision making, and to develop and evaluate new treatments and services.1 For palliative end-of-life care (PEoLC) research, the participation of patients, carers and family members ensures the research provides meaningful insights into living with a terminal illness and opportunities for new treatments and interventions to be developed and evaluated. Yet, there can be resistance from individuals, including healthcare professionals,2 to discuss and invite research participation as assumptions are held about patient and family members’ vulnerability and associated burdens towards the end of life.3 The practical and ethical obstacles to research participation have been documented in the literature.4 Particular barriers include issues with gaining consent, additional burdens on patients and families (including distress and anxiety) and equipoise between care and research needs.4–6
However, the benefits of research participation have also been evidenced,7 8 including with vulnerable populations.9 Gaining a balanced and nuanced understanding of how adult patients, carers and family members actually feel about taking part in a research study at the end of life is important. Providing researchers with a better understanding of an individual’s research experience could lead to enhanced patient participation in research, and patient-orientated methodologies and protocols.
Aims
The aim of this rapid review is to gain a deeper understanding of the experiences and perspectives of adult patients, carers and family members who have participated in a PEoLC research study.
Methods
This rapid review was conducted between July 2020 and September 2020 and was informed by the guidelines put forward by the Palliative Care Evidence Review Service.10 A rapid review methodology was adopted due to time and resource constraints and to focus on the most recent research in this field. The review was reported according to Enhancing Transparency in Reporting the Synthesis of Qualitative Research guidelines.11
Inclusion and exclusion criteria
Inclusion criteria
Included papers reported on primary, qualitative studies that enquired specifically about adult patients’, carers’ or family members’ experiences of participating in PEoLC research, published between 2010 and 2020 in the English language and conducted in OECD (Organisation for Economic Co-operation and Development) countries.12
Exclusion criteria
Research exploring participants’ experience of involvement roles in research as defined by the National Institute for Health Research Centre for Engagement and Dissemination were excluded.13 This rapid review was specifically interested in the participant, carer and family member perspective on participation. Research exploring the views of other stakeholders (such as researchers, clinicians, nurses) was excluded. Studies were excluded if they explored curative treatments and those involving children under the age of 18, as these areas of research have their own specific issues relating to gatekeeping and accessing this population for research and cannot be studied alongside an adult population.14–18
Search and selection strategy
The search was conducted across three online databases (MEDLINE, PsychInfo and PubMed) for studies published from 2010 to 2020.
A predefined search criterion was applied and was based on that used in a similar paper1 with the removal of ‘involvement’. The search terms used were as follows: (palliative or terminal or end-of-life, or hospice, or death or dying or bereave or supportive care)) AND ((attitude or experience or perspective or challenge or benefit or burden) AND (research).
Three independent reviewers (BFH, CH and LEC) screened titles and abstracts of citations for eligibility using Endnote X8.19 Full texts were consulted where necessary. Disagreement between reviewers was resolved through discussion with an additional reviewer (KK).
Data extraction and synthesis
The following data were extracted from each paper and entered into Excel: methodology including study aim, what participation entailed, duration of participation; setting; method of recruitment; participant characteristics, clinical information including diagnosis and stage of illness; participant reported benefits of, and barriers to, research participation participant retention and study conclusions.
Eligible papers were transferred into Nvivo V.11 for analysis.20 Thomas and Harden’s thematic synthesis method21 guided the data extraction and synthesis processes. This involved three stages: (i) line-by-line coding of extracted text, (ii) development of descriptive themes and (iii) generating analytical themes from the studies’ data. The review was not registered on PROSPERO, as there are no direct health-related outcomes. Line-by-line coding of the findings of each study, including participant quotes was undertaken by reviewers. Through discussion between reviewers the codes were refined. Similarities and differences between codes were identified and clustered to inductively generate descriptive themes. Analytical themes and subthemes were generated through additional discussion, reflection, and iteration.
Quality assessment
To assess the quality of the included research papers, Hawker’s Risk of Bias tool22 was used and produced a score for each study of a minimum of 9 points and a maximum of 36 points. This assessment included scoring of the abstract, methodology, sampling, analysis, ethics and bias, generalisability, and implications. It should be noted that scores were not used to exclude studies but to provide an indication of the quality of each included paper. See online supplemental table 2 for individual scores.
Supplemental material
Primary data collection
In addition to the rapid review, a survey and focus group was undertaken to explore wthe themes and recommendations identified in the review. A survey was developed using Microsoft Forms to gather information from attendees at the Marie Curie Palliative Care Virtual Research Conference In November 2020 (from 27.22 min), at which early findings of this review were presented. The survey (online supplemental appendix 1) was distributed electronically to attendees during and after the presentation. The audience were clinical professionals in PEoLC and responding to the survey was entirely optional indicating implied consent from those who chose to respond. No demographic information is available for survey respondents.
Supplemental material
A virtual focus group was held with five Marie Curie Research Leads and Fellows who are academics with extensive experience in conducting PEoLC research. The same question format as the survey was applied to the discussions to explore feedback on the recommendations and whether the benefits and barriers in the review were reflective of their experience as researchers. The focus group discussions were recorded using Microsoft Teams.
Patient and public involvement
Three members of the Marie Curie Patient and Public Involvement (PPI) group, called Research Voices were involved throughout the process of this rapid review and two are coauthors on the paper (MB and SP). The Research Voices generated the analytical themes and subthemes with the remainder of the authors. They shared their experiences and expertise in PEoLC, and research which helped to clarify the themes, and to ensure that the recommendations that were drawn up were both practical and reasonable. The Research Voices challenged any assumptions held by the remainder of the authors and provided insight that helped shaped the review. The Research Voices commented on each draft and any extra materials generated related to the work (eg, presentation materials for the Marie Curie Palliative Care Virtual Research Conference).
Results
Search and selection strategy
Across the three databases, 3578 papers were identified, of which 157 were duplicates. An additional paper was identified by contacting experts in the field. Of the remaining 3423 studies, 3341 were excluded after screening the abstracts and titles.
The full texts of 41 papers were reviewed and a further 37 were excluded. Figure 1 presents the search and selection process.

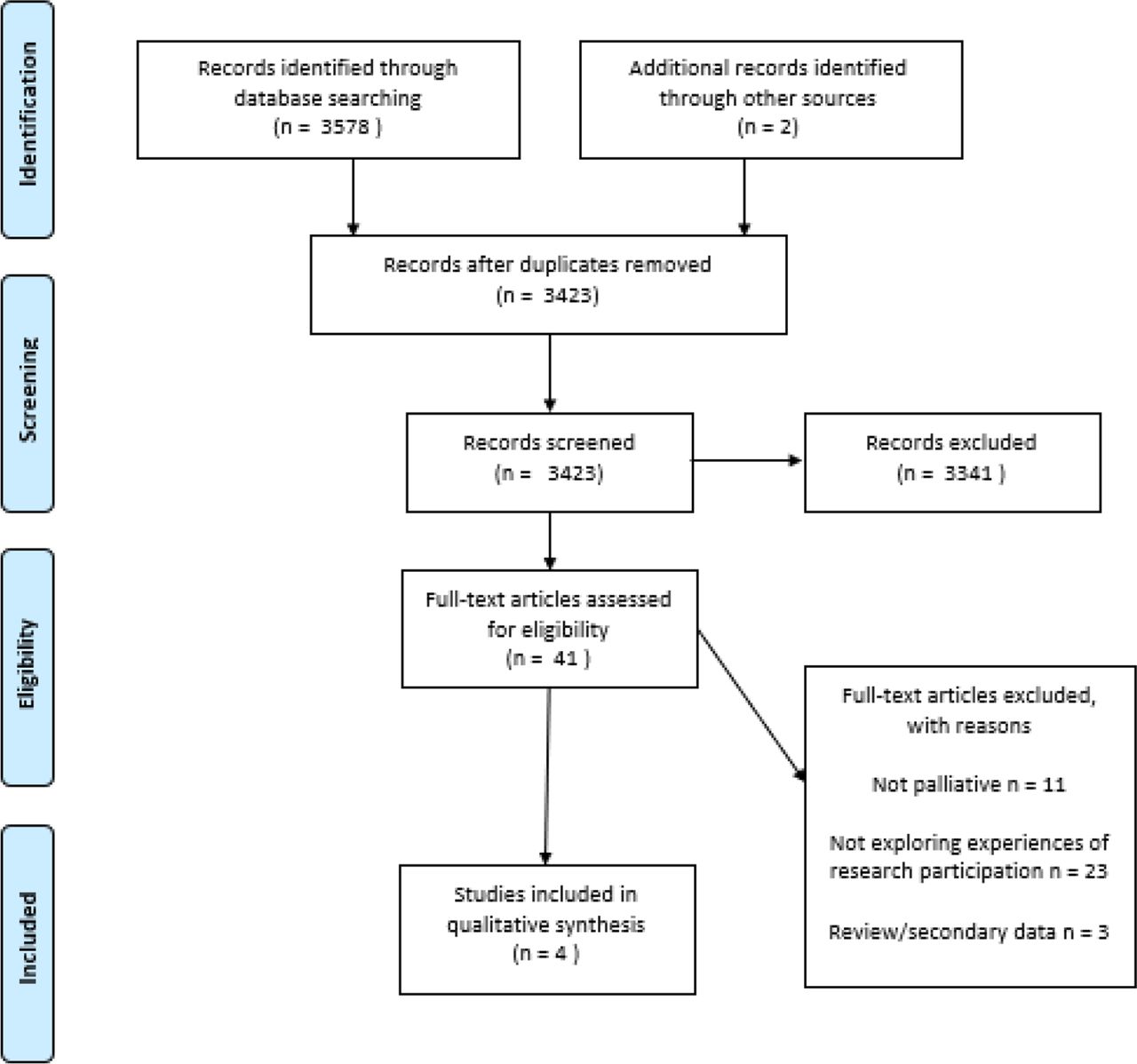{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram.
Four papers were included in the final thematic analysis.23–26
Characteristics of included studies
The characteristics of the four included studies are summarised in tables 1 and 2.
The nature of the evidence
Study characteristics
Two studies explored the views of patients participating in PEoLC,23 26 and two explored the views of family members or carers a person with a terminal illness.24 25 In total, the papers represent the experiences of 70 patients and 347 family members. Patients who participated in the studies were those with cancer (n=52)23 and severe Chronic Obstructive Pulmonary Disease (COPD) (n=18).26 The majority of participants in included papers were white females.
Two studies were conducted in the USA, one in Switzerland and one and in Australia. All studies explored the views of patients or carers who had participated in clinical trials
All studies utilised retrospective interviews. Two studies conducted face to face interviews,25 26 two used telephone interviews24 25 and the method of interview was not reported in one study.23
Three of the four included studies involved participation in hospital-based studies,23 25 26 and the other was home based.24 Participants across the studies were in receipt of different interventions, see table 2.
Thematic synthesis
Seven high-level themes were identified from the four studies: benefits or positive aspects included altruism and perceived benefits for participants themselves. Feeling overwhelmed by the situation, participation not being seen as relevant, being reminded of being a patient. Unmet needs, practical issues, not seeing the research as relevant to them, being reminded of being a patient and feeling overwhelmed were identified as barriers or negative aspects of participation (table 3).
Benefits and barriers to participation in palliative and end-of-life care research, and recommendations to facilitate participation
Benefits or positive aspects of participation
Two overarching themes encompassing the benefits participants reported in their experiences of PEoLC research—altruism and benefits for themselves—were identified.
Altruism
Improving things for other patients and carers
Altruistic factors were identified as motivators for research participation. Patients and carers described wanting to help improve matters for others in similar situations in the future. One patient described their reason for participating:
"A psychological benefit in knowing that someone is thinking about these issues actually helped me. At least someone is doing research in this area and may make some changes to help others in our situation". (Control 128)24
This often reflected less of an attempt to improve matters for themselves and more of an acceptance that changing the eventual outcome for themselves at this stage was not possible.
Raising awareness
Participants reported wanting to raise awareness, including making a difference for others by helping to shape government priorities and contributing to knowledge in the field to increase healthcare professionals’ understanding of conditions and caring:
"I am happy to do whatever I can to help if it makes a difference for others. Unless the government knows the details of what we need they can’t make a difference." (Control 77)24
"Well, I guess my attitude is that, um, knowledge is power. The more that the scientists and the doctors know, the sooner there is going to be a cure, or there is going to be a treatment that is going to prolong somebody’s life". (P3 Intervention; Breast)23
Benefits for themselves
Practical insight and access
In addition, participation in research in PEoLC provided benefits to the participant themselves, including gaining practical insights, for example, access to information. Patients and carers reported that having an increased number of contacts within the medical/research field provided further sources of information, which sometimes was not provided by their primary clinicians.
"I remember thinking that it could probably only be a positive thing to maybe get some extra information or some extra help with getting information. So I couldn’t see any downside". (Group 1; ID# 2)25
Emotional insight and support: feeling supported and reassured, giving a sense of hope
Patients and carers found that their participation also provided emotional insights and support, including feelings of reassurance, support and giving a sense of hope. The sense of hope was not hope for recovery or a cure but hope for receipt of extra support, information or improvement in quality of life.
The feelings of support and reassurance were particularly important and were achieved for some participants in simple ways, including having regular check-ins with researchers:
"… the phone calls. Especially in the beginning when I felt really lousy from the chemo … I think it’s kind of made everything just a little easier". (P4 Intervention; Breast)23
Moreover, participants found that the research gave them further practical insights and access, including enhanced problem solving. A strong theme arising from the studies was that the research provided an opportunity for participants to gain a better understanding of their own condition:
"She [nurse] especially brought me practical elements that nobody else could give me, in fact. Doctors don’t treat us like that. So she did the transition between the simply human side, and the doctor who never answers those questions: ‘how should I eat’ or ‘what I could do to breathe better". (Participant 14, palliative care, female, 70 years old)26
Having someone independent to talk to
Carers reported that research participation also provided an opportunity to speak to an independent person allowing an impartial space for them to express themselves in.
"I can tell you and you are impartial with my answers. I think it was very beneficial". (Control 8)24
Validation of the caring role
A carer explained how the research had offered time for reflection on their role as a carer and validated their caring role:
"It makes you think a little, made me realise the emotional side of caring and how [with] a lot of those issues you tend to ‘soldier on’’’ (Intervention 115).
Moreover, as caregivers we’re prompted to reflect about the issues at hand, they developed greater insight into both their own need for support and the services available to them.24
Barriers or negative aspects to participation
While positive aspects of participating in palliative care research were described, several barriers or negative aspects to participation were also reported by participants.
Feeling overwhelmed by the situation
One identified barrier to participating in PEoLC research was that potential participants could feel overwhelmed by the situation, leaving little capacity for participating in research.
"When your mind is in shock, it is really hard to turn the emotional side off and turn the analytical research side on and say, ‘‘Yeah, this is an okay thing’”. For me, I just didn’t even want to deal with it". (Group 2; ID# 14).25
Participation not seen as relevant
For some patients, they assumed research was not relevant to them, whether that was because of their stage of disease, or in relation to symptom manifestation:
"Actually, up until a couple of months ago, a lot of the stuff that was in the book that I was given, it wasn’t even appropriate. I mean, it wasn’t necessary for me … at first I couldn’t relate to a lot of the stuff". (P17 Intervention; GI)23
Reminded of being a patient
Patients also explained that being invited to participate in research emphasised their identity as a patient and reminded them of their disease. Palliative or end of life patients are already surrounded by discussions about their disease and/or health and expressed that sometimes they just wanted to be seen as a person, rather than a patient:
"I don’t want to be a patient every day of my life". (P14, Intervention; GI)23
"And it’s a way for me to evacuate basically. And that’s what saves me a bit. (…). If we think about it, we keep talking about it, it becomes burdensome. Yes. Too burdensome. (Participant 7, palliative care, male, 71 years old)"26
Practical barriers
Practical barriers, for example, feeling too unwell, travel distance, clash with medical appointments and time required to dedicate to research were noted as reasons to deter participation in PEoLC research. Two participants in the studies considered within the scope of this review reported practical barriers including time, travel distance and being too sick.23 26
Unmet needs: disappointment for self and disappointment for others
Another overarching theme identified as a barrier or negative aspect to participation was unmet needs, which was expressed in terms of disappointment for the individual themselves and disappointment surrounding the participation of others.
For the individual, there was commonly disappointment when participants were randomised to a control group as they did not receive the intervention and the support they were expecting from the trial.23 Even individuals who were randomised to the intervention arm in one study expressed disappointment at the limited interaction with the researcher, and some were of the opinion that ‘nothing was done’ as there was no tangible change to medication or treatment.26
Participation and engagement of others were noted as disappointing for participants, with an expectation that everyone else would be as motivated to participate as themselves:
"The biggest disappointment was going into the group meetings and feeling as if … the energy wasn’t there … So, I didn’t feel like it was as helpful as it could have been". (P14 Intervention; GI.)23
Recommendations for research teams
Based on the perceived positive and negative aspects of participation in PEoLC research described by participants, recommendations for research teams have been developed to facilitate participation, enhance the positive aspects and potentially minimise the negative aspects of research participation. See table 3 for a summary of the recommendations.
Communication
Ensure that the aim and requirements of the study are discussed clearly with potential participants (many participants in the reviewed studies could not remember the aim of the research):
"But I can’t remember, I can’t remember, you can’t remove it from me. I don’t want to talk nonsense to say, because I don’t know, so, honestly. I can’t even tell you how those ladies [the nurses] were. Probably nice, but … "(Participant 10, palliative care, male, 73 years old)26
Consider the format of written information given to participants to read at a later date which includes the contact details of the research team.
Participants should be offered a summary of the research findings or have access to updates on the project and findings for example, through a website. This approach will enable support through an established feedback loop where participants, where possible, are kept up to date with the project progress until publication (those that are more research aware may be more likely to participate in future studies).
"I’m very familiar with how you do research … I’m sure if [people] were more familiar with it, they would be more prone to do it" (Group 3; ID# 21)25
Build rapport with participants—recognise participants as individuals and that data collection is only part of the interaction.
"[The researchers] were really aware [of the stressful circumstances] and acted accordingly. I think that sometimes it helps the stress to talk about why you're there and what’s going on in your life. So, I think that’s kind of a natural benefit just to get you to open up and not hold it all inside". (Group 1; ID# 17)25
Be sensitive in tone and language used (consider what else is going on for the participant) and ensure communication is personal and appropriate:
"When you are talking to the carer, your disposition and tone of voice is important, the caring tone shows genuine interest and is a good thing for the caregiver, they pick up on this. "(Intervention 605)24
Appreciating the researcher’s role from the participants’ perspective
If possible, provide information about the services available to participants and link them in (participants described seeing research as a source of local information):
"Well, the actual [study enrollment] was just maybe five minutes’ worth of time, but she spent at least another 20 minutes with me … kind of her own personal things about best time to go down to the cafeteria, when it’s not so crowded and … you know, little things like that." (Group 1; ID# 5)25
Where possible, be flexible in the timing and methods of data collection used (participants described good days and bad days):
Similarly, participants who were feeling relatively well or preferred to use denial or avoidance to cope with their illness didn’t want to feel like “… a patient every day” (P14 Intervention; GI) and preferred to have less contact with medical professionals.23
Strengthening the recommendations
Survey and focus group
To explore the acceptability of the recommendations generated, feedback was sought from a range of clinicians, researchers and people with lived experience in the field of PEoLC research in the form of a survey and focus group (see methods and online supplemental appendix 1).
See table 4 for an outline of the main feedback points from the survey respondents and focus group participants. Further detail on the results can be found in online supplemental file 1.
Summary of the key points identified from the survey and focus group
Discussion
This review has identified the benefits or positive aspects of participation in PEoLC research and barriers, or negative aspects of participation, as described by patients, family members and carers. Despite participants often reporting altruistic benefits to participation, this review identified a number of ways in which participants themselves can benefit, including gaining access to services, receiving additional support and validation of their caregiving role. This finding indicates that participants often have their own personal reasons for taking part in research and that they do not always necessarily share the ethical, concerns of clinicians and healthcare professionals. These concerns can lead to gatekeeping, and may reflect a more paternalistic style of medicine, both of which have been reported elsewhere.7 27
Despite these reported benefits in the considered studies, the review also identified barriers or negative aspects to participation in PEoLC research, which included feeling overwhelmed, practical barriers (such as feeling too unwell and travel distance) and the reminder of being a patient. This review has considered these negative aspects and developed recommendations for researchers, clinicians and wider research teams, in an attempt to negate these barriers and support and encourage participation in research.
There was a strong sense that the participants within the included research studies, wanted to be recognised as individuals, rather than another unwell person nearing the end of their lives. Participating in research has the potential to provide psychosocial benefits to participants, as ongoing interactions with healthcare professionals and researchers can help to guide participants through uncertainties faced. It has been reported that in these interactions, it is essential that participants’ personal identity is acknowledged, and their role is seen as the ‘patient as person’ rather than the ‘person as patient’.28 The survey results further support the idea that participants have personal reasons for both choosing to participate and varying barriers to participation (see online supplemental file 1).
Strengths and limitations of the review
This review used a rapid review methodology which has enabled a rapid literature search to identify studies published within the last 10 years related to the research question, providing up to date and relevant research within the field of PEoLC. However, this method does not consider all research in the field and has strict inclusion/exclusion criteria.
The review benefited from the involvement of PPI representatives as part of the research team. The representatives provided insights from their own experiences of being approached to participate in PEoLC as former carers for those at the end of life which strengthened the development of the recommendations. In addition, feedback was sought from a range of PEoLC clinicians and researchers which has resulted in the development of practical and achievable recommendations for researchers within the field.
Despite including research from OECD countries, no papers exploring the experience of participation in UK-based studies were included, as none were identified in the literature search. Those included were in the USA, Australia and Switzerland, and although parallels in research approaches can be drawn to the UK, specific UK-based studies would be an interesting avenue for future research, as there may be some cultural differences between nations as well as different health system funding models.
Three of the four included papers explored the experiences of participation in research-based in a hospital setting. The setting in which the research is conducted may influence the experience of participants. For example, participants in hospital-based studies where they are an inpatient or visit on a regular basis may be less burdensome than someone who must travel to the hospital as an outpatient for the purposes of research.
In addition, all included studies involved relatively low commitment levels, for example, completion of questionnaires, monthly nurse visits, which could be viewed as less burdensome. Further exploration of the experiences of participation in other types of studies which may involve more invasive interventions or more time commitment and potentially more barriers or negative aspects for participants, is an avenue for future research.
The quality of the included research papers was assessed using the Hawkers Risk of Bias scores. There was a variation in quality of the included studies, however, the decision was taken to include all studies and not use a score cut-off, as only four studies were eligible for inclusion. The bias scores can be seen in online supplemental table 2.
Practical barriers were identified but to a lesser extent than was expected, being reported in only two studies. This suggests that participants in PEoLC research may not be deterred by practical barriers such as travel distance, and time commitments. However, this may also have been influenced by the type of study and participation requirements of included studies, . Therefore, these studies may not be representative of studies which require more time commitment or need for additional travel. Further exploration of the impact of practical barriers on research participation would be of interest, particularly given the necessary and rapid uptake of digital solutions due to the COVID-19 pandemic as face-to-face interactions have been either limited or impossible.
Furthermore, the authors were unable to explore other characteristics of participants which may influence their experience of participation, their perceived levels of social support, their living arrangements or the presence or absence of a carer. This would be particularly interesting in those who reported that participation benefited them in terms of emotional insight and support, making them feel more reassured, and whether this was confined to those who were missing emotional support outside of their interactions with the researcher(s).
Within the recommendations, the development of an established feedback loop to provide participants with ongoing updates until the point of publication of the research findings has been suggested. It is acknowledged there is some potential difficulty in applying this practically within PEoLC research. It is not uncommon for patients to die during the study or shortly after due to the prognosis of terminal diseases. Combined with this, it can often take many months or years for a publication to be released, however, we suggest that it may still be possible for the carers or family members of the participant to be offered the opportunity to be informed of the research findings, should they wish to.
The survey and focus group provided an opportunity to gain feedback on the relevance of the recommendations from professionals within the field. However, small sample sizes were limited.
In addition, the authors acknowledge that the research considered within this review explores the experiences of those who can consent for themselves and does not specifically address those participants who have lost or diminished capacity for example. However, the recommendations put forward in this report provide useful learning for all l participant groups, including carers if they are involved in proxy consent.
Avenues for future research
There is a need for further research into the particular experiences of participation within UK-based research studies. It is noted that all the included papers explore the participants’ experience of research retrospectively and this has its limitations, including recollecting the experience accurately. Participants may exhibit recall bias dependent on their perceived experience and only report either the good or the bad aspects of participation. It would also be interesting to explore the impact of the setting and methodologies used by researchers on likely uptake of the recommendations.
When considering the demographic features of participants in the included studies, it was clear that there was very limited evidence exploring the experiences of participants from diverse backgrounds and marginalised groups. This is an important area for future research as the benefits and barriers to participation in PEoLC research are likely to be culturally sensitive.
Qualitative studies exploring the participant experience embedded within trials may be better able to capture patient experience alongside the impact or outcomes of interventions. This would enable a more rounded assessment of the interventions being assessed which could be useful for future development and implementation.
Further consideration of the specific terminal condition being experienced and the relevance of these benefits, barriers and recommendations would also be useful. Patients, carers and family members are likely to have very different needs depending on the condition or disease and this may also affect their ability or willingness to participate.
Further evaluation of the recommendations in practice is required.
Recommendations for practice
Overall, areas have been identified within research and research delivery that can be improved to encourage participation or improve experiences of participants in PEoLC research. These recommendations are practical and achievable and could be implemented by research teams in the field relatively easily. Moreover, these recommendations align with those identified in a project undertaken by versus Arthritis.29 Similarly, they found that, within their community, individuals need to understand and feel connected to research to enable a high-quality experience, and to increase the likelihood of participation in the future. This shows that while the recommendations in this review are aimed at PEoLC researchers specifically, the underlying principles of improving communication and empathising with the patient role and journey are more universal and are paramount in research in other areas.
Researchers are encouraged to adopt these recommendations, as they have been developed from the experiences of participants within the included studies and in collaboration with members of Marie Curie Research Voices Patient and Public Involvement group, who are former carers and have had experience participating in PEoLC research. These recommendations can be implemented for general best practice within research.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to acknowledge the Motor Neuron Disease Association for allowing Dr Kirsten Kelly to work on this review alongside Marie Curie. The authors would also like to acknowledge the contributions of Diana Robinson, Marie Curie Research Voices member.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @brionyhudson
Collaborators NA.
Contributors BFH, LEC, CH and KK conducted the literature screening and selection, data analysis and interpretation, drafting and revision of the article. MB and SP contributed to the development of the qualitative themes, data analysis and interpretation and reviewing article drafts. All authors were involved in final approval of the version of the publication.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. BFH, LEC and CH’s posts were funded by Marie Curie. KK’s post was funded by the Motor Neurone Disease Association.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.