Article Text

Abstract
Background Palliative and end-of-life care is a core competency for doctors and is increasingly recognised as a key clinical skill for junior doctors. There is a growing international movement to embed palliative care education in medical student and junior doctor education. To date there has been no review of the literature concerning the views and experiences of junior doctors delivering this care.
Aim To review the published literature between 2000 and 2019 concerning junior doctors’ experience of palliative and end-of-life care.
Methods Systematic literature review and narrative synthesis.
Results A search of six databases identified 7191 titles; 34 papers met the inclusion criteria, with a further 5 identified from reference searching. Data were extracted into a review-specific extraction sheet and a narrative synthesis undertaken. Three key themes were identified: (1) ‘Significance of death and dying’: all papers found that junior doctors care for many patients approaching the end of life, and this often causes emotional distress and can leave persisting memories for many years afterwards; (2) ‘Thrown in at the deep end’: junior doctors feel unprepared and unsupported in providing palliative and end-of-life care; and (3) ‘Addressing the gaps’: junior doctors often experience a medical culture of disengagement towards dying patients and varying attitudes of senior doctors. Subsequently they have to learn the skills needed through seeking their own opportunities.
Conclusion Medical education needs to change in order to better prepare and support junior doctors for their role in caring for dying patients. This education needs to focus on their knowledge, skills and attitudes.
- education and training
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Acute hospital wards are the most prevalent place of death across the world: 47.4% of deaths in England and Wales in 20161 and 58% globally.2 Most hospital palliative and end-of-life care is provided by patients’ normal clinical teams rather than palliative care specialists,3 where junior doctors mainly work and are at the front line of end-of-life care provision.4
Palliative and end-of-life care has therefore been recently described as ‘a core competency’ for all doctors because of the need to have excellent skills in clinical assessment, communication, multidisciplinary teamwork and prescribing to provide this care for patients.5 Across the globe there is an increasing emphasis on embedding palliative care in the education of all medical students and doctors.5 6 However the literature suggests that medical student education in this subject area is patchy and frequently inadequate.7 There is limited understanding of how this affects recent graduates’ provision and experience of palliative and end-of-life care.
We therefore undertook a systematic review of the literature concerning junior doctors’ experience and views of providing palliative and end-of-life care. To our knowledge no such review has been previously undertaken.
Aim
The aim was to undertake a systematic review and narrative synthesis of the international literature concerning junior doctors and end-of-life care focusing on the following:
What is their experience of providing care?
What are their attitudes towards providing care?
How adequately prepared do they feel?
How supported do they feel?
Methods
Search strategy
A search strategy was devised in collaboration with a professional medical librarian (IK). An initial scoping search strategy was reviewed against the inclusion and exclusion criteria, following which the definitive search strategy was developed (figure 1).
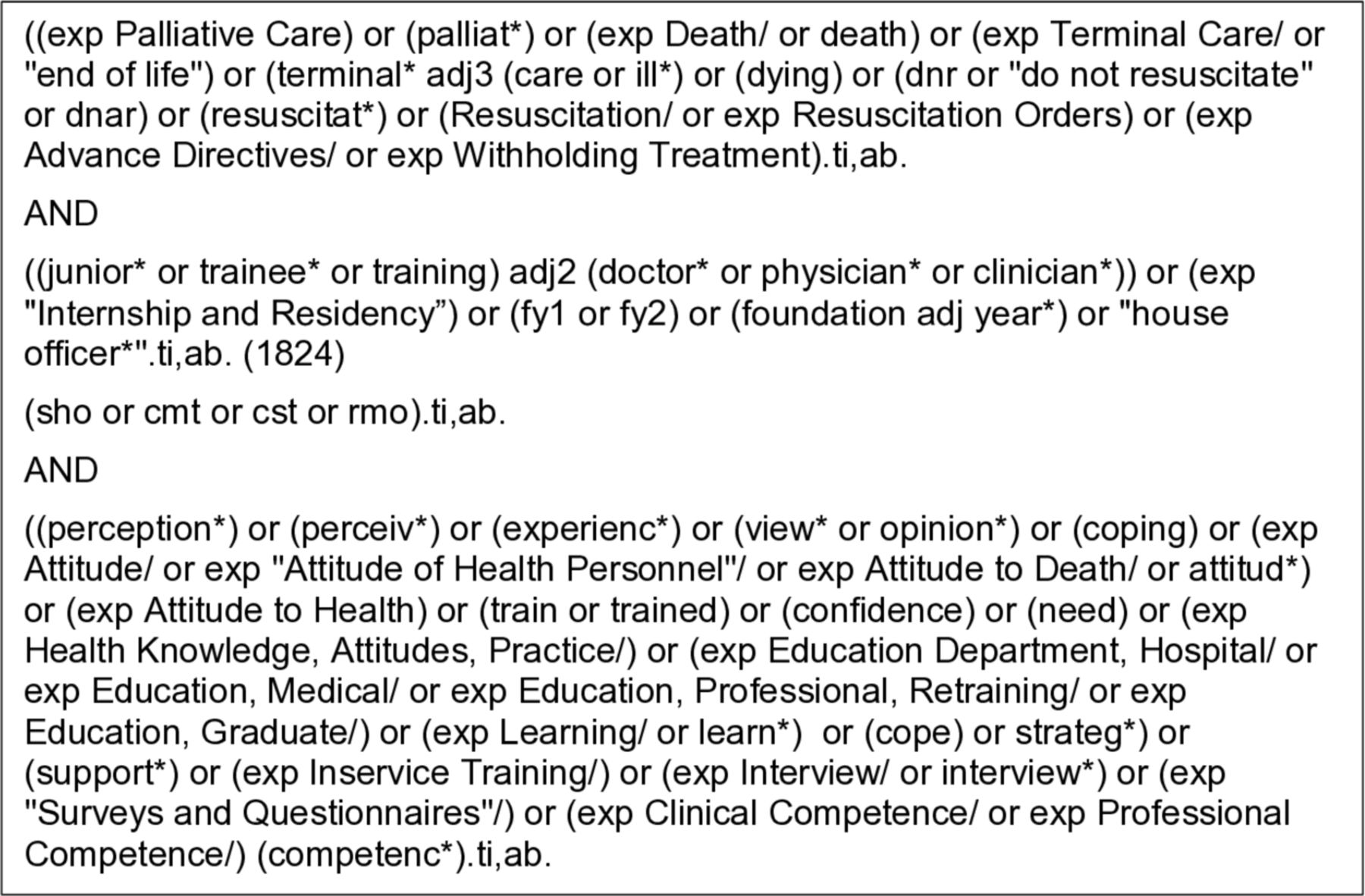
Medline search strategy.
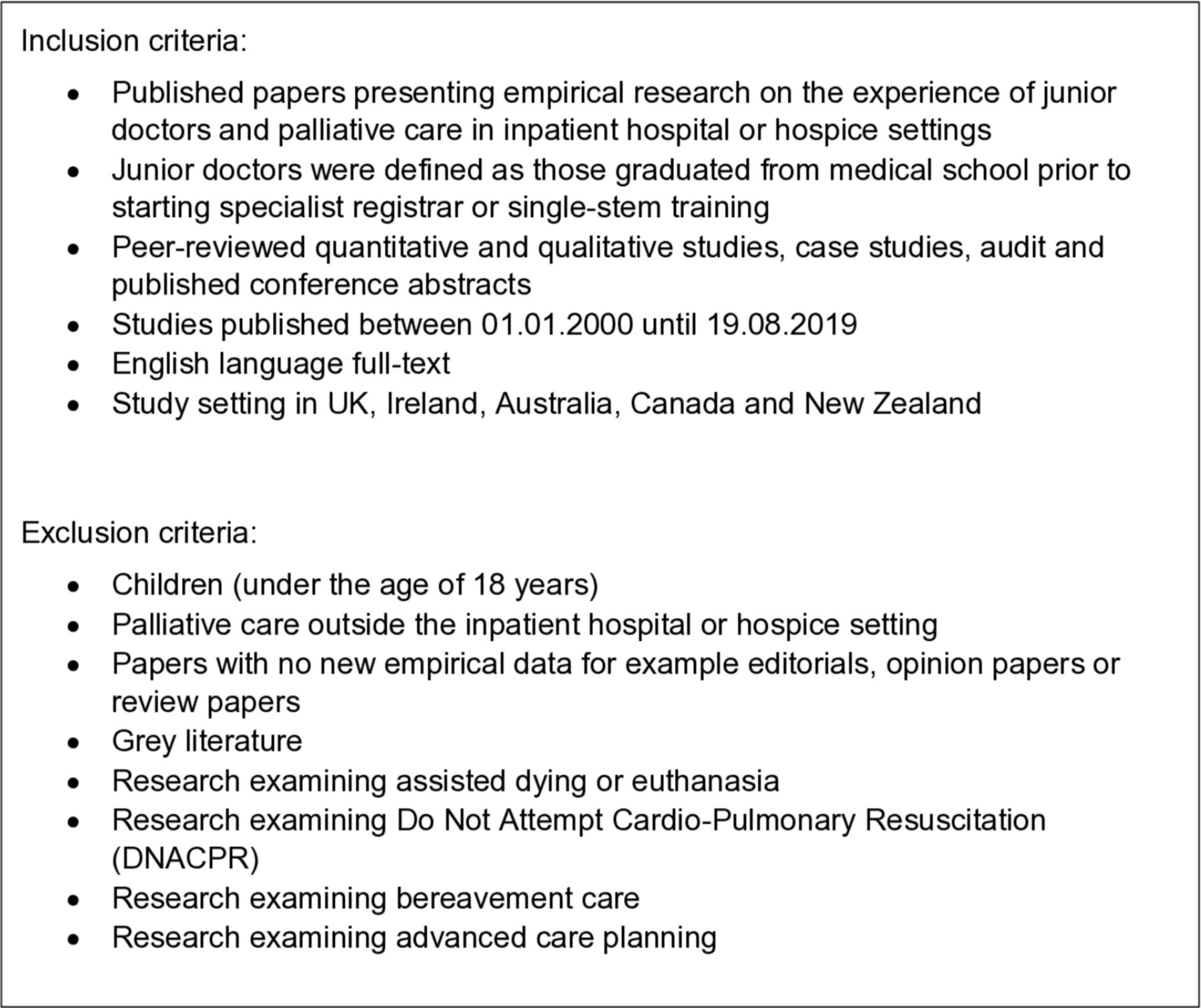
The inclusion and exclusion criteria are summarised in figure 2. Due to a review published in 2000 demonstrating widespread palliative and end-of-life care education in medical undergraduate curricula, we sought to review the effect of this undergraduate teaching on junior doctors’ experience.8 For the purpose of the review, we define ‘junior doctors’ as those who had graduated from medical school but had not yet entered a specialty training programme; for example in the UK, this would be the foundation programme, core medical or core surgical training years (previously known as junior and senior house officers). Junior doctors predominately work in adult inpatient settings during the early years of their careers; therefore, only hospital or inpatient hospice settings were included. Care of children and young people under 18 years of age as well as bereavement care were excluded as they are considered specialist areas.

Inclusion and exclusion criteria.
The literature was restricted to countries with broadly similar healthcare services, medical training programmes and cultural contexts: the USA was excluded as doctors enter specialty training very early in their careers. Opinion pieces, literature reviews and editorials were excluded unless they contained original empirical data.
Conducting the search
We searched six electronic databases (Medline, Embase, PsycINFO, Web of Science, Scopus and Cochrane) for papers published between January 2000 and August 2019. The search was initially run until January 2018 and then subsequently updated in August 2019 to ensure that any additional papers were captured within this review.
The search results were downloaded into EndNote and duplicates were removed. All titles, abstracts and full-text papers were screened by the first reviewer (AB), with a sample of abstracts and full-text papers screened by the second reviewer (TM). Any disagreements were resolved by review team discussion (AB, TM and SB).
Data analysis
A narrative thematic analysis was used to synthesise the heterogeneous literature, which enabled an empirical ‘data-driven’ approach to identify themes.9 Included papers were weighted by AB, with a sample independently weighted by TM, for their contribution towards answering the review questions, using the Gough’s weight of evidence framework, which measures each paper against rigour of study design, appropriateness to the review question and relevance to answering the question.10
Results
Search results are summarised in the adapted Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart (figure 3). Thirty-four papers were included from the database search, with a further five from reference searching of included papers. Of these 39 papers, 23 were from the UK and 7 from Canada, with 9 from across the globe; 17 used quantitative methods, 18 qualitative methods and 4 mixed methods. The quality of the papers varied on the Gough’s weight of evidence: 11 weighted high, 16 medium and 12 low quality (7 of which were conference abstracts). The included papers are summarised in online supplementary file 1.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
PRISMA diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
All the papers provided evidence that the majority of junior doctors provide palliative and end-of-life care for many patients early in their careers.11–49 An average of 40% (range: 36%–46%) of junior doctors cared for 1–10 patients, while 51% (range: 40%–61%) of junior doctors cared for more than 10 patients.16 26 38 44
Three major themes were identified: (1) ‘Significance of death and dying’; (2) ‘Thrown in at the deep end’; and (3) ‘Addressing the gap’.
Significance of death and dying
Providing palliative and end-of-life care has a significant effect on junior doctors’ emotional well-being and professional attitudes. Their first few patient deaths are memorable and powerful experiences.13 17 24 26–30 36 Junior doctors report an emotional impact, describing themselves to feel ‘sad’ and ‘depressed’,13 23 26 44 ‘anxious’ and ‘stressed’,12 15 16 28 39 and ‘guilty’, ‘dread’, ‘helplessness’ and a ‘sense of failure’.14 26 44 45 Two studies revealed that 12% of junior doctors are scoring for identifiable post-traumatic stress disorder and 25% for psychological distress from caring for dying patients, as per the Post-Traumatic Stress Disorder Checklist-Civilian Version (PCL-C) scale and the 12item General Health Questionnaire (GHQ-12) measure, respectively.26 28 There was one exception, with a low Gough’s weight of evidence study, which reported working in an inpatient hospice was not emotionally draining.20 Overall early career experiences of death and dying are significant and memorable for doctors throughout their careers.29 36 39
Junior doctors’ personal attitudes towards palliative and end-of-life care varied. Many report a belief in the importance of palliation,14 17 20 21 24 34 37 41 44 45 47 48 some describing it as a privilege to care for patients at the end of their life.30 45 Some view palliative care as similar to other aspects of medicine, describing it as problem-solving patients’ symptoms.25 39 45 Junior doctors describe a ‘taboo hospital culture’ towards patients approaching the end of their lives13 30 and a professional disengagement towards palliative management,22 25 29 30 42 where doctors maintain a distance from their patients29 42 45 and inform more junior colleagues, including students, to do the same13 19 as well as prioritise other clinical tasks.25 One paper reported that junior doctors who have observed such practice subsequently questioned their careers.13
Thrown in at the deep end
Junior doctors feel unprepared and out of their depth when caring for patients approaching and at the end of their lives.12–15 18 22 26 29 30 38 40 46 47 Two studies, both with medium Gough’s weight of evidence, had contrasting results: in one, 80% of junior doctors reported they ‘felt comfortable’ caring for dying patients, although only 54% ‘felt comfortable’ alleviating suffering48; in another, 65% of junior doctors reported they were ‘well prepared’ for palliative and end-of-life care, although this was inversely correlated with their knowledge score in the area.49 Palliative and end-of-life care is more challenging for junior doctors out of hours,26–28 41 42 due to frequent lack of clarity or delays in deciding about goals of care, patients being unfamiliar and having to make independent decisions.
Junior doctors commonly report being unsupported by their hospital teams in managing palliative and end-of-life care,13 14 17 18 22 26 27 40 42 45 apart from one paper in which 90% reported being able to discuss these patients with their team.36 Support is sought and received from other junior doctors as well as senior medical colleagues.35 42 Senior support is variable and specialty-dependent,12 17 22 38 42 with most support being practical advice rather than emotional.17 Senior support is particularly lacking when senior doctors had limited experience of caring for frail older patients or greater experience in medical or surgical interventions.37 38 40 41
Junior doctors report receiving support outside the medical team, from nursing colleagues,22 27 35 40 41 47 palliative care specialists,12 18 22 25 40 friends and family,17 39 and online advice.35
Addressing the gap
Junior doctors perceive that palliative and end-of-life care is not optimally provided in inpatient hospital settings,14 27 38 41 47 and frequently express strong requests for further training in the area.12 14 15 22 25 26 28 32 34 38 40 41 45 46 48 Junior doctors consider active participation and experiential learning as the most effective way to bridge their knowledge gap in palliative and end-of-life care.12 15 17 20–22 25 29 31 37 40 41 Palliative care rotations, at postgraduate or undergraduate level, are seen as the best way to achieve this12 15 20–22 25 28 because the rotations or placements are valued as opportunities to address the unmet needs from medical school, which included specific and transferable skills in symptom control, professionalism, teamwork, communication, reflective practice17 20 21 25 37 44 and in ethical-legal framework.17 There was one exception where junior doctors reported hospice placements as medically deskilling experiences, but this had a low weight of evidence.20
Other learning methods valued by junior doctors include observation of senior colleagues14 17 21 31 37 40 43 49 and reflection in clinical contexts14 17 24 40 41 or social settings.17 39 There is a preference for practical and case-based teaching12 15 22 40 41 46 49 particularly addressing symptom control,15 32 38 40 44 46 48 prescribing21 the dying process12 20 21 and role-playing difficult conversations.21 25 31 48 Written material and guidance were also valued as ways to support junior doctors’ prescribing21 33 40 and handover out of hours.41 It was reported that undergraduate and postgraduate assessments were a way to increase the curriculum priority of palliative and end-of-life care, for both educators and junior doctors.
Discussion
The literature reveals that junior doctors are caring for a high number of patients needing palliative and end-of-life care. Providing such care has a significant emotional demand on them, leaving memories that persist for many years. Junior doctors feel ill-prepared and inadequately supported in this role and frequently request further training. Attitudes towards palliative and end-of-life care varied: some view it as a privilege, while others associate it with a culture of disengagement that stigmatises dying patients.
This is the first review to systematically review and synthesise the international literature concerning junior doctors’ experience in providing palliative and end-of-life care, which reflects a varied weight of evidence and quality of the literature, with a range of research methods employed. It provides a timely and contemporary review of training and identifies development needs in the area, which has been rising in public interest following the Liverpool Care Pathway for the Dying Patient withdrawal and subsequent independent report.50 The report highlighted that there were multifaceted reasons for the poor care that some patients in hospitals received towards the end of their life, one of which being lack of appropriate training and support.
Limitations
We recognise that the use of the term junior doctors varies between countries, with the transition into a single-stem specialty training occurring at different time points in junior doctors’ careers. The review is limited to the UK, Ireland, Canada, New Zealand and Australia, where there is greater commonality in postgraduate medical training and healthcare systems, permitting synthesis of the data. However all the themes were identified from studies in all of these countries, suggesting they are of generalisable relevance. The grey literature was not searched and publications were limited to the English language. The database search was augmented by reference searching to minimise the risk of relevant information being omitted; that this only identified a further five papers suggests that the database searches were robust.
Interpretation of the findings
The wider literature identifies that junior doctors worldwide feel unprepared for many areas of clinical practice, lack senior support which increases their stress in the workplace and that this experience is worse out of hours.51 The review has identified that junior doctors face these same challenges when caring for palliative and end-of-life care patients, which reflects the broader pressures junior doctors face.
However, the additional impact of palliative and end-of-life care is that there is only one chance to get it right and the significance of the associated emotional burden. Therefore greater attention is needed to junior doctors’ well-being, since caring for these patients is a significant source of stress for them.13 39 This review reveals that such support is commonly not forthcoming, and instead the ‘taboo culture’ of a death in a hospital52 continues to prevail, with senior doctors distancing and avoiding dying patients and thus contributing to poor palliative and end-of-life care.
Implications for future practice
This review has identified a pressing need for further development of medical education in palliative and end-of-life care; this will improve the quality of patient care, equip doctors with transferrable skills, and provide them with support and resilience to deal with an emotionally demanding aspect of medicine.
The recommendations that arise are highlighted under Bloom et al’s53 domains of knowledge, skills and attitudes.
Knowledge
Despite recent increases in undergraduate palliative and end-of-life care education,8 junior doctors remain frequently unprepared to care for these patients. They perceive palliative care as receiving a lower curricular priority than other aspects of medicine at both undergraduate and postgraduate levels, with specific knowledge gaps identified in symptom control, communication and the dying process. A greater focus on palliative and end-of-life care is urgently needed.
Skills
Palliative and end-of-life care is holistic and needs doctors to use a wide range of skills. Junior doctors learn and gain skills in palliative care through their personal experience and active participation. They express strong requests for further experiential learning through palliative care attachments, apprenticeship and shadowing, approaches known to improve preparedness for medical practice more generally.8 51
Attitudes
Palliative and end-of-life care places a particular emotional demand on healthcare professionals, which for some junior doctors makes palliative care unique and special, while others find it a negative emotional experience. Junior doctors need to be supported in understanding their experiences and emotional reactions when caring for the dying. Junior doctors benefit from reflection with their professional or personal colleagues; this only frequently occurs in unstructured and ad-hoc ways. Balint groups and similar structured reflection could be an effective way for junior doctors to receive emotional support,54 facilitating confidential and safe spaces to share experiences.19 The roles of senior doctors as mentors and supervisors may greatly influence their junior colleagues’ attitudes towards patients who are towards the end of life.
Conclusion
The review has demonstrated that junior doctors frequently feel unprepared and unsupported to provide palliative and end-of-life care, with greater emotional demands than other areas of medicine. There is a pressing need for changes in undergraduate and postgraduate medical education to focus on the development of knowledge, skills and attitudes of junior doctors in this area of patient care. This can be achieved through increased curriculum content, experiential learning opportunities, and supportive and reflective practice. This will go a long way to enable future generations of junior doctors to be empowered and able to care for palliative and end-of-life care patients.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ilk21
Correction notice This article has been updated since it was first published. The article type has been changed to Systematic review.
Contributors AB designed and had the concept of the work. AB and SB planned the study. AB and IK designed the literature search terms, with AB conducting the literature search from January 2000 to January 2018 and IK conducting the database search from January 2018 to August 2019. AB screened the titles, abstracts and full texts, and weighted the papers, with TM completing a sample selection at each stage. AB, TM and SB achieved consensus on any discrepancies in screening decisions. AB, SB and TM analysed and identified the themes. AB wrote the draft of the article. AB, SB and BW contributed to interpretation and critical revision of the article. All the authors approved the final version. AB is guarantor of the paper.
Funding SB is supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRC) East of England at Cambridgeshire and Peterborough NHS Foundation Trust. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. AB was supported by the Academic Foundation Programme through NIHR funding through the Health Education England East of England Deanery.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.