Article Text

Abstract
Objective To describe the nature and scope of a new Hospice at Home (H@H) service and to identify its equality of provision.
Methods Case note review of patients supported by a H@H service for 1 year from September 2012 to August 2013 (n=321). Descriptive analysis to report frequencies and proportions of quantitative data extracted from service logs, referral forms and care records; thematic analysis of qualitative data from care record free text.
Results Demand outstripped supply. Twice as many night care episodes were requested (n=1237) as were provided (n=613). Inequalities in access to the service related to underlying diagnosis and socioeconomic status. 75% of patients using the service had cancer (221/293 with documented diagnosis). Of those who died at home in the areas surrounding the hospice, 53% (163/311) of people with cancer and 11% (49/431) of those without cancer received H@H support. People who received H@H care were often more affluent than the population average for the area within which they lived. Roles of the service identified included: care planning/implementation, specialist end-of-life care assessment and advice, ‘holding’ complex patients until hospice beds become available and clinical nursing care.
Conclusion There is significant unmet need and potentially large latent demand for the H@H service. People without cancer or of lower socioeconomic status are less likely to access the service. Action is needed to ensure greater and more equitable service provision in this and similar services nationally and internationally.
- primary health care
- palliative care
- home care services
- hospice and palliative care nursing
- health inequalities
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- primary health care
- palliative care
- home care services
- hospice and palliative care nursing
- health inequalities
How this fits in
Hospice at Home services are being implemented nationally and internationally to support the growing numbers of people wishing to die at home. With considerable variation in practice, little is known about how these services function. This evaluation of one service found demand far outstripped supply and revealed inequality of access, patients with cancer being five times more likely to receive Hospice and Home care than those dying from non-malignant disease.
Introduction
UK healthcare policy has seen an increasing focus on palliative and end-of-life care over recent years, stimulated by the 2008 National Health Service (NHS) End of Life Care Strategy, that sought to ensure that people approaching the end of their lives receive the best care possible and are as involved in decisions regarding their care as they wish.1
One such decision concerns where individuals would prefer to be cared for towards the end of their lives. While for many the stated preference is to be at home, this varies across clinical conditions2–4 and may decrease with older age as people fear experiencing greater dependency due to chronic disease and are concerned about becoming a burden to family members.5–9 Recent reviews have highlighted how many studies reporting preferred place of death included high proportions of respondents with no recorded or stated preference regarding where they would like to die.10 11 In light of the most prevalent place of death in many countries being hospital,12–16 the UK hospice movement has responded with the development of ‘hospice at home’ (H@H) services. These provide more intensive nursing care in the home than is usually available17 seeking to enable patients with advanced illness considered to be approaching the end of life, to be cared for and to die at home, if that is their preference. H@H aims to reduce inpatient admissions, facilitate discharge from inpatient care, provide assistance during crises and to provide support during the final days of life at home.
Several H@H services embrace the fundamental paradigm of end-of-life care, with an acceptance of death as a natural end of life to be enabled at home if possible, rather than a defeat of modern medicine to be fought in hospital.18 H@H services give considerable importance to autonomy in enabling people to die at home if so wished while providing optimum comfort (beneficence) and avoiding unnecessary investigations and admissions (non-maleficence). They are believed to be more cost effective than inpatient care (justice).19
The international literature identifies several factors that are known to adversely impact on the likelihood of dying at home, including limited availability and use of home care services to support patients and their informal carers,20 non-cancer diagnosis, greater socioeconomic deprivation, older age, non-Caucasian ethnicity and female gender2 16 21–24 though the effect of some of these factors varies between countries. Fear of the dying process and among patients, their families and healthcare professionals also plays a role in preventing people from dying at home.25 Accurate prognostication and timing of palliative care service introduction is challenging for frail older people with multiple comorbid conditions.26 27
While there is some evidence that community-based palliative care teams may reduce acute care use at the end of life and hospital deaths,28 international studies of the effectiveness of H@H services are limited by the diverse models of care, which have often been developed in response to varying local needs.17 29 The small body of evidence suggests bereaved lay carers and healthcare professionals have broadly favourable opinions and experiences of H@H.30–33 Death at home with community support is associated with lower health resource costs compared with death in hospital or hospice.34 35
H@H and similar home-based palliative services continue to be developed across the UK and in other countries, yet few studies have described in any detail the care provided. This paper describes for one service:
Service recipients
Sources and appropriateness of referrals
Service supply in relation to demand
Equity of service provision
Service roles and functions
Methods
Setting and subjects
Based at the Arthur Rank Hospice in Cambridge, UK, the Cambridgeshire H@H service covers an urban and large rural area, with a population of 620 000 and low levels of ethnic diversity (84.5% White British). While the population of Cambridge city is young (mean age 35.6 years), the mean age of the rest of the county (39.5 years) more closely mirrors the age of the general population (40.0 years).36
Most episodes of H@H care are delivered by a team member staying with a patient overnight from 22:00 to 07:00. For the purposes of this evaluation, an episode of care was defined as a period of night care. Referrals are triaged by the senior nurse during the day and assigned a red, amber or green rating based on the severity of clinical need of the patient and family with care prioritised for those assessed as red priority. The level of symptom control required and the emotional welfare of the patient, family or carers is taken in to account if documented on the referral forms or during discussions with referring healthcare professionals. Those requiring a higher level of physical or psychological care are assigned to registered nurses, those with less complex needs to healthcare assistants. All team members have had advanced education in communications skills and end-of-life care. During the course of the evaluation the team expanded from 1 Clinical Nurse Specialist manager and 1 qualified nurse to 6 nurses, 2 bank nurses, 14 healthcare assistants, a complementary therapist and 2 part-time administrative assistants. The service assessed referrals to be appropriate if patients were estimated to be in the last 2 weeks of life.
Data collection
The study population comprised all patients accepted for care by the Cambridgeshire H@H service between 1 September 2012 and 30 August 2013. Individual patient level data were obtained from referral forms, clinical records and study-specific ‘night care’ documents (table 1). These data were extracted by research administrators and entered onto a study spreadsheet with a study identification number for each patient.
Sources of data
Data concerning place of death for all adults within Cambridgeshire were obtained from the local Public Health Intelligence Team. The patient’s GP practice was used to assign patients to an area of the County.
Socioeconomic status was defined using the Index of Multiple Deprivation 2010 based on patient postcodes, which were collected and held separately from the main dataset in order to maintain anonymity. Diagnosis was established from certified underlying cause of death; ‘living alone’ indicated usually lived alone with no resident carer; ‘living at home’ indicated living in own home or care home.
Analysis
Descriptive quantitative analysis of frequencies and percentages was undertaken within MS Excel 2010. Free text data extracted from the night care documents were analysed using thematic analysis, which aims to bring order and structure to data by identifying themes and assessing whether there is any relationship or variation between them.37 Qualitative data management was facilitated by NVivo10. All analysis was undertaken by JB who was a nurse researcher at the University of Cambridge.
Results
During the 12-month study period, 321 patients received care from the H@H service: 1122 episodes of night care were provided (median 2 per patient, range 0–48). Tables summarising results below report varying numbers in analysis due to missing data.
Referrals, patient characteristics and place of death
Patient characteristics are described in table 2 and referrer information in table 3. The majority of patients who received care from the H@H service were 78 years old or older, three quarters had a cancer diagnosis, just under half were women. One in five patients lived alone. Patient’s ethnicity was recorded by the clinical team in less than 15% of cases and so is not reported here. Most patients died within 1 week of referral (55%, n=152): 6% (n=17) died within 24 hours and 13% (n=37) were referred more than a month before death (range 1–204 days between referral and death). The predominant reasons for referral were psychological support for patient and family (54%, n=233) and symptom control (52%, n=118) (multiple reasons given).
Patient demographics
Referrer characteristics (n=287)
Of those with a recorded preferred place of death (n=283) 91% (n=259) died in their preferred place, see table 4.
Preferred and actual place of death of patients cared for by H@H service (n=283)*
Supply and demand for H@H service
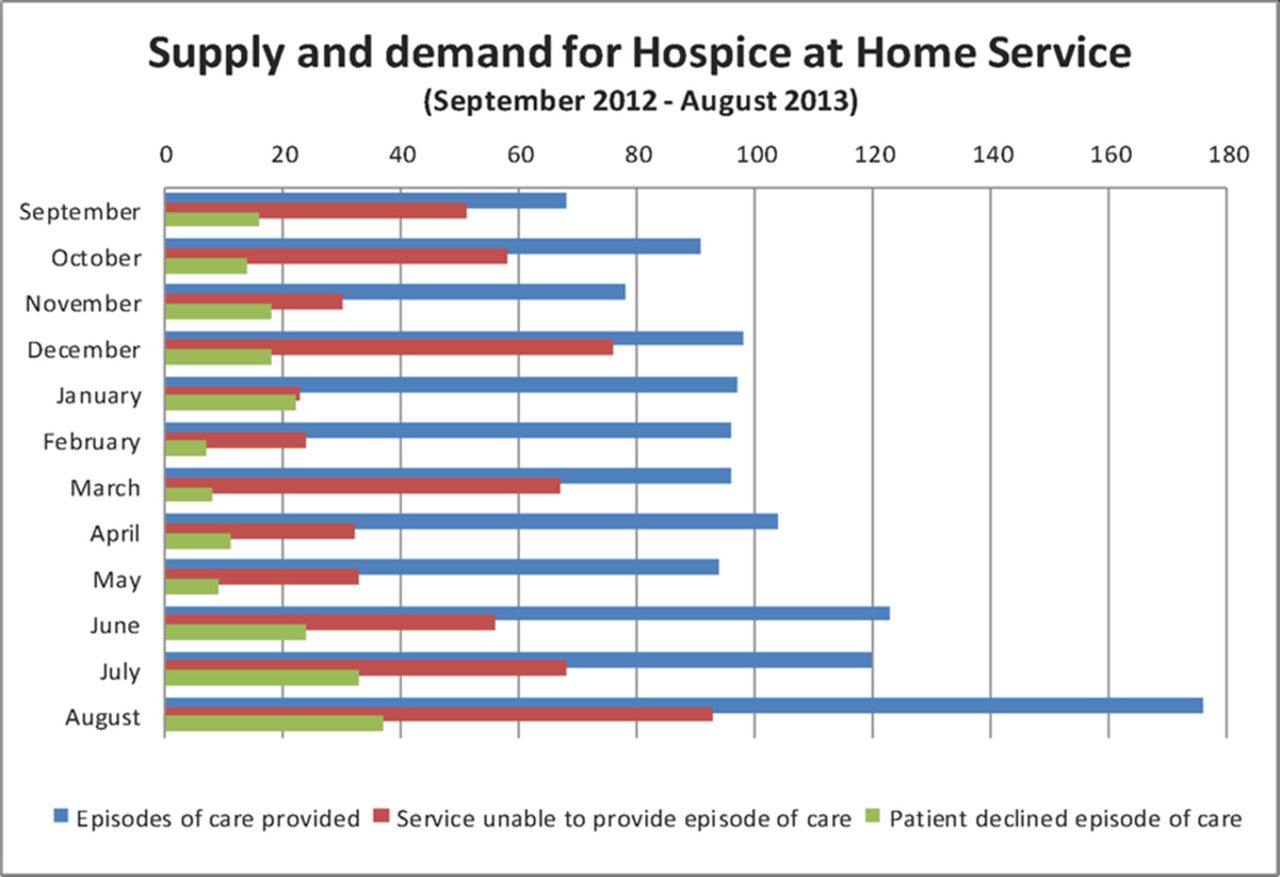
Both supply (episodes of care provided) and demand (episodes of care requested) rose steadily throughout the evaluation (figure 1). Supply rose almost threefold over the 12 months, a time when the service was expanding considerably, with 178 episodes of care provided in August 2013 compared with 64 in September 2012. Unmet need, based on episodes of care requested but not provided, also rose during the study period, with some fluctuation. H@H provided at least one episode of care for 27% (200/742) of all deaths at home in the three areas closest to the hospice.
{kind=link}
Supply and demand for Hospice at Home Service
Equity of service provision
In the two areas most often served by H@H (South Cambridgeshire and Cambridge City), there was a trend for those receiving the service to be less socially deprived than the populations within which they lived (table 5). Very few patients in Fenland, the most rural and deprived area in the county, received the service.
Index of multiple deprivation scores (n=253)
H@H provided care for 11% (49/431) of those who died at home with conditions other than cancer and 53% (163/311) of those who died at home with cancer in the three areas closest to the hospice (Cambridge City, South Cambs. and East Cambs., data not available for Huntingdonshire and Fenland).
Roles and functions
Data from 736 night care documents (65% completion rate) and 1519 telephone call records involving H@H team members revealed a wide range of roles performed by the H@H team (table 6). At times staff reported having ‘gone in cold’ to a patient’s home with little information: this was particularly challenging when they encountered a home environment that was unsuited for end-of-life care.
Night time nursing roles of Hospice at Home team
Organisational and specialist roles
The H@H service played an important role in communication between care professionals regarding the planning and delivery of care, as documented in telephone call data. Most calls were from H@H to family and carers (35%, n=531) or healthcare professionals (35%, n=526). Many conversations were with the community nurses responsible for care during the day, including reports on the patient’s clinical condition, discussion of syringe driver drugs or anticipatory medication. Twenty-one per cent (n=312) of calls were from healthcare professionals to H@H, while 7% (n=105) were from family and carers. The H@H service was at times used to support patients overnight who were awaiting hospice admission.
The team’s palliative care Clinical Nurse Specialists also visited patients at home during the day to assess care needs and provided specialist advice for healthcare professionals concerning symptom management and clinical care issues.
Discussion
Summary
This study examined the role of one H@H service in one area of the UK. Care planning and coordination of care across services during the day and at night was a key element, along with overnight nursing care provision, providing complex clinical care in sometimes challenging home situations. People who died from cancer at home were five times more likely to be supported by H@H than those with non-cancer diagnoses: this may be due to patterns of referral to the service, the referral criterion that people should be within 2 weeks of death or other reasons. In addition, the most deprived and rural area of the county was poorly served by H@H: only 11 people there received the service. Action to ensure that H@H is available for patients with conditions other than cancer and in more deprived areas is urgently needed.
Strengths and limitations
While limited to a single H@H service, the paper provides adds to the currently limited knowledge-base available for other service development. We are unable to determine the effectiveness of H@H within the descriptive study design. We were also unable to quantify or examine the day time assessment visits. Our data do not allow us to determine the number of deaths in care homes which were supported, as ‘home’ was defined as the usual place of residence, which included private domestic dwellings as well as care homes. Despite it being a mandatory requirement to record patient’s ethnicity in patient’s medical records in UK, this data item was rarely completed in the routine clinical documents accessed as part of this evaluation. The lack of available data regarding patients’ ethnicity is a notable limitation, as being from an ethnic minority is a known barrier to accessing specialise end-of-life care38 39
Comparison with existing literature
H@H services vary widely across the UK, from daytime-only services provided by Clinical Nurse Specialists and Palliative Care doctors to 24 hours services staffed by healthcare assistants. Some also provide postbereavement and lymphoedema care.40–43 Few studies have investigated the roles that H@H services fulfil.44
In 1971 Julian Tudor Hart wrote of the ‘Inverse Care Law’, an observation that ‘the availability of good medical care tends to vary inversely with the need for the population served’,45 contrary to the principle of equity which is at the heart of the National Health Service. Subsequent research has repeatedly confirmed that those living in areas of higher social deprivation, with greater healthcare needs, have poorer services which they have greater difficulty accessing46–48 and are further disadvantaged by greater multimorbidity at an earlier age.49 The present study is consistent with this literature and with a study of a previous form of the Cambridgeshire H@H which found patients with cancer in lower socioeconomic areas were less likely to be referred.21 50 The Manchester H@H service has reported lower referral rates for those with greater social deprivation.22 The inverse care law is still in operation in the 21st century.
The great majority of patients supported by H@H had cancer. While this compares favourably with a H@H service piloted in North West England in which 92% of patients had cancer,51 our finding that only 11% of people who died at home with conditions other than cancer received H@H support, while 54% of people who died at home with cancer were cared for by H@H, is continuing evidence of diagnostic inequality of H@H provision.52–54 General practitioners in Scotland have been found to identify palliative care needs for 75% of people who died from cancer but only 20% of those who died from other conditions.55 A study in Wales found that 46.2% of people who died of cancer had recorded palliative care needs or had received specialist palliative care, compared with only 5.3% of people who died from other causes.56
In part this may be due to greater prognostic uncertainty concerning illness trajectories in conditions other than cancer.57 It may also be due to organisational and institutional cultures which traditionally have had a cancer focus in palliative and end-of-life care. It is widely acknowledged that it is of urgent importance to redress this inequality in access palliative care services such as H@H: end-of-life care for those without cancer is of lower quality, a deficit that might be mitigated by a H@H service.58
Implications for research and practice
In a society where death has become increasingly hidden and medicalised, many people who wish to support loved ones to die at home may be doing so with little or no prior experience of death and dying to draw on.59 With ageing populations and rising multimorbidity later in life, the need for palliative care is increasing.60 61 As the trend towards fewer people dying in hospital continues in many, though not all countries,61–64 services such as H@H, which exist to support carers and patients emotionally and physically to enable a natural acceptance and dignified end of life, are becoming an increasingly vital resource to allow people to die at home.
This study has identified the important roles that a H@H service plays in the care of people approaching the end of life and in a detail that has not been reported before. It has also highlighted a dismaying gap between demand for such a service and the available supply. Robust research into alternative models of care is a priority to ensure equity of access for all people and families who would benefit from palliative care services such as H@H, particularly those from less advantaged backgrounds and with non-cancer diagnoses. We would urge services to measure and demonstrate their effectiveness and equality of care provision.
Acknowledgments
We would like to acknowledge the contributions of Dr Zoe Morris to the study design, Katie York, Andrea Newman and Andy Cowan to data collection and entry and Dr Jane Fleming for very helpful comments on the final draft of this paper.
References
Footnotes
Contributors LMot, LMor, LW and SB conceived the study. All authors contributed to the study planning and design. JB contributed to data collection. JB analysed and interpreted the data with input from SB. JB wrote the manuscript with input and feedback from SB, LMot, LMor and LW.
Funding The study was jointly funded by the Arthur Rank Hospice Charity and the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care Cambridgeshire and Peterborough (CLAHRC CP) Programme, which was recommissioned as NIHR CLAHRC East of England in 2014.
Disclaimer The opinions expressed are those of the authors and not those of the NHS, the NIHR or Department of Health.
Competing interests This study was undertaken by the Palliative and End of Life Care Research Group of the University of Cambridge. It was part-funded by the Arthur Rank House Hospice Charity who part-fund the H@H service. LW, Mot and LMor are employed by the Arthur Rank Hospice Charity.
Ethics approval This study was approved by the Chair of a Local Research Ethics Committee (LREC) to be service evaluation and not to require LREC approval. The research team followed standard procedures for the ethical conduct of research involving the use of patient-identifiable information.
Provenance and peer review Not commissioned; externally peer reviewed.