Article Text

Abstract
Objectives Opioid-induced constipation (OIC) can affect up to 63% of all patients with cancer. The objectives of this study were to assess quality of life as well as efficacy and safety of naloxegol, in patients with cancer with OIC.
Methods An observational study was made of a cohort of patients with cancer and with OIC exhibiting an inadequate response to laxatives and treated with naloxegol. The sample consisted of adult outpatients with a Karnofsky performance status score ≥50. The Patient Assessment of Constipation Quality of Life Questionnaire (PAC-QOL) and the Patient Assessment of Constipation Symptoms (PAC-SYM) were applied for 3 months.
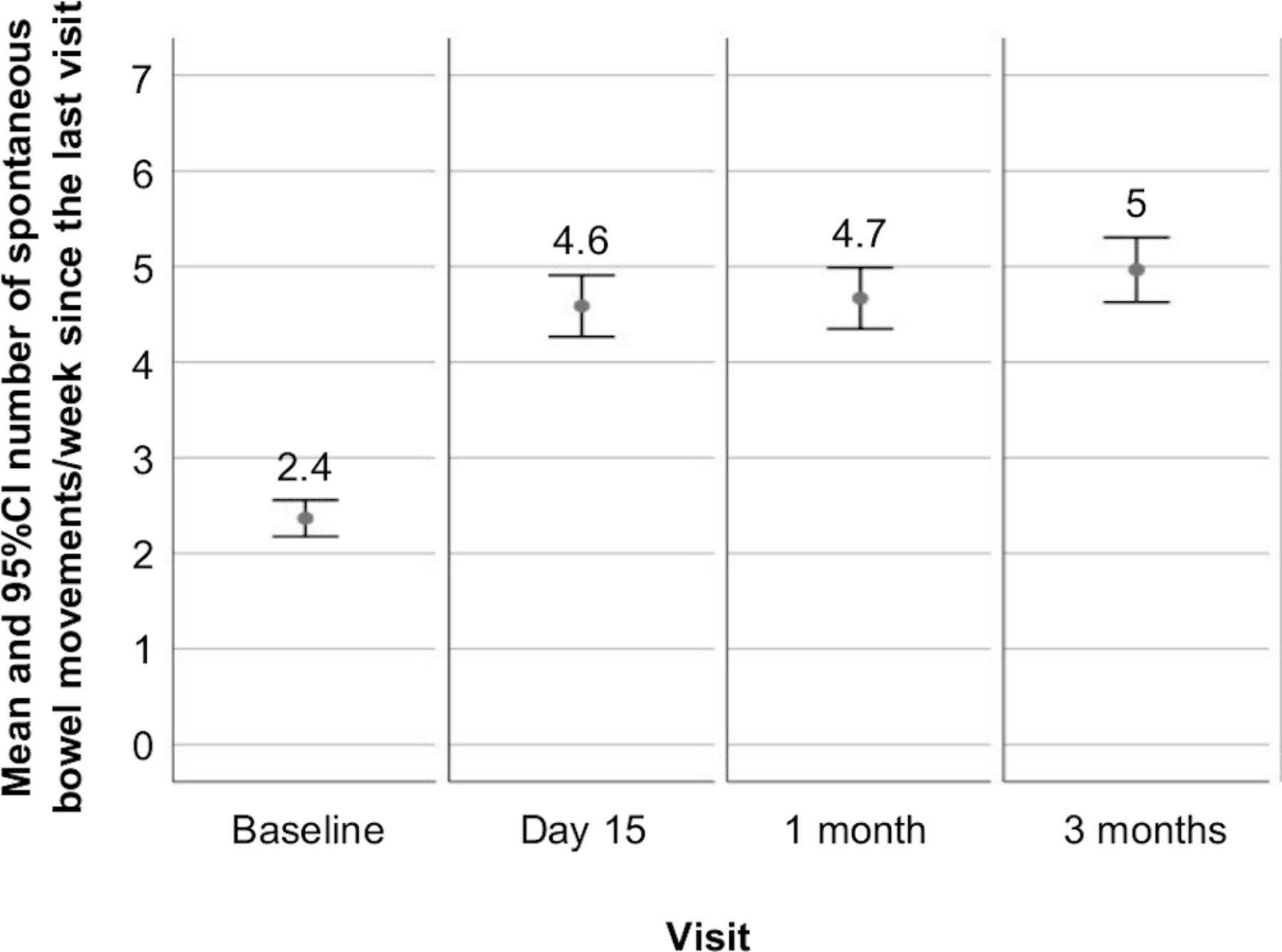
Results A total of 126 patients (58.2% males) with a mean age of 61.3 years (range 34–89) were included. Clinically relevant improvements (>0.5 points) were recorded in the PAC-QOL and PAC-SYM questionnaires (p<0.0001) from 15 days of treatment. The number of days a week with complete spontaneous bowel movements increased significantly (p<0.0001) from 2.4 to 4.6 on day 15, 4.7 after 1 month and 5 after 3 months. Pain control significantly improved (p<0.0001) during follow-up. A total of 13.5% of the patients (17/126) presented some gastrointestinal adverse reaction, mostly of mild (62.5%) or moderate intensity (25%).
Conclusions Clinically relevant improvements in OIC-related quality of life, number of bowel movements and constipation-related symptoms were recorded as early as after 15 days of treatment with naloxegol in patients with cancer and OIC, with a good safety profile.
- constipation
- cancer
- pain
- quality of life
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Opioid-induced constipation (OIC) is one of the most common adverse effects of opioid use for the treatment of pain, affecting 15%–90% of all non-cancer patients and up to 63% of all patients with cancer.1–10
OIC may occur at the start of opioid use and persist throughout the treatment period, in contrast to other adverse effects of opioids such as nausea, vomiting and sedation, which disappear over time.5 Treatment based on hygiene-dietary measures and laxatives is not effective in many patients. The discontinuation of opioid therapy is the only option in such cases.11 In up to one-third of all cases, the opioid dose is reduced by the physician or by the patient in the hope that this will cause the symptom to disappear.10 However, it has been shown that the dose at which constipation usually occurs is approximately four times lower than the dose required to produce an analgesic effect; dose reduction is therefore unlikely to cause constipation to disappear.12
Constipation has a negative impact on patient general condition and quality of life, often leading to temporary discontinuation of opioid treatment, resulting in inadequate pain control.10
For patients, constipation relief may be even more important than pain relief.13 14 Chronic opioid use causes constipation to also become chronic, with the resulting risk of haemorrhoids, rectal fissures, bowel obstruction that may lead to colon rupture and, in extreme cases, death.6
No medical definition of OIC had been established before presentation of the Rome IV criteria,15 16 where OIC appeared as a new category.
The management of constipation includes its prevention, the suppression of causal factors and the use of laxatives.17 In patients with cancer, the Spanish Society of Medical Oncology (Sociedad Española de Oncología Médica) guidelines recommend continued laxative use together with opioid treatment.18 The European Society for Medical Oncology has recently published a guide for the management of constipation in patients with cancer.19
The American Gastroenterological Association has also recently published guidelines for the management of OIC.20 This same year, an European experts consensus document has been published on the physiopathology and management of OIC, recommending treatment with naloxegol in patients exhibiting an inadequate response to laxatives.21
Naloxegol is a pegylated naloxone derivative that was approved by the United States Food and Drug Administration (FDA) in 2014 for the treatment of OIC in adult patients with non-cancer pain, and by the European Medicines Agency (EMA) that same year for use in patients with or without cancer. The drug is indicated for the treatment of OIC in adults with an inadequate response to laxatives.
The objective of this study was to assess the evolution of quality of life and symptoms related to OIC in patients with cancer treated with naloxegol, and to obtain data on the safety and efficacy of the drug in real-life setting.
Methods
A prospective, observational follow-up study with a total duration of 12 months was designed. This report presents the results of the interim analysis of the first 3 months of follow-up in four visits (baseline, 15 days, 1 month, 3 months).
A total of 16 investigators belonging to centres in 12 Spanish provinces participated in the study: 12 medical oncologists, 2 radiation oncologists and 2 from the Palliative Care Unit.
The first patient was enrolled on 21 September 2017 and database closure for the interim analysis on 9 April 2019.
Written informed consent was obtained from all patients included in the study.
Patient screening
The study population consisted of patients with cancer presenting a confirmed diagnosis of OIC with inadequate response to laxatives, and in which treatment with naloxegol was indicated.
OIC was defined based on the Rome IV criteria.15 16 An inadequate response to laxatives was defined as patients reporting symptoms of OIC for at least 4 days in the 2 weeks prior to the study while receiving treatment with at least one class of laxatives.
The inclusion criteria were: (1) men and women over 18 years of age; (2) a diagnosis of active oncological disease requiring treatment with opioids for pain control; (3) patients with symptoms of OIC at the time of screening (an average of <3 spontaneous bowel movements a week with associated symptoms of constipation in at least 25% of the bowel movements); (4) patients with an inadequate response to laxatives for the treatment of OIC, and with indication for naloxegol; (5) patients with a Karnofsky performance status score ≥50 at study entry; (6) outpatients at study entry; (7) patients with sufficient capacity to complete the data corresponding to the symptoms and quality of life scales; and (8) patient's signed informed consent.
The exclusion criteria were those described as contraindication in the Summary of Product Characteristics of naloxegol and patients with cognitive impairment or uncooperative.
The patients completed a diary recording the number of weekly bowel movements, the use of rescue medication, changes in pain treatments and the appearance of adverse reactions to naloxegol.
Primary endpoint
The primary endpoint was the assessment of constipation-related quality of life in the patients receiving naloxegol, using the Patient Assessment of Constipation Quality of Life Questionnaire (PAC-QOL), in its validated Spanish version.
The PAC-QOL questionnaire consists of 28 questions grouped into four subscales: worries and concerns, physical discomfort, psychosocial discomfort and satisfaction. The patients reported the severity of each symptom on a 0–4 point scale referred to the last 2 weeks. The total score and the score corresponding to each subscale were calculated by averaging the scores. Changes in the total or subscale scores of ≥0.5 points were considered clinically relevant. A higher PAC-QOL score means poorer quality of life.22
Secondary endpoints
The secondary endpoints included evaluation of the efficacy of naloxegol in treating OIC over follow-up, defined as the proportion of responders: patients with three or more bowel movements a week, and one or more bowel movements a week additional to the number of bowel movements at baseline.
As secondary efficacy endpoint, we evaluated the constipation symptoms using the Patient Assessment of Constipation Symptoms (PAC-SYM) in its validated Spanish version, referred to the last 2 weeks.23 This instrument consists of 12 questions with 3 subscales (stool, rectal and abdominal symptoms). The patients reported the severity of each symptom on a 0–4 point scale where 4 corresponds to greatest intensity. The total score was calculated from the average of the scores of each subscale.
The safety of naloxegol treatment was assessed based on the adverse reactions described during patient follow-up.
Control variables
Information was collected on patient age, gender, weight, height, body mass index, socioeconomic level (low: annual income in euros<25 000; middle: 25 000–45 000; high: >45 000), medical history, date of cancer diagnosis, organ affected by the cancer, presence of metastasis, history of treatments for OIC and pain control and Karnofsky performance status at study entry.
At each visit, the patients scored their pain intensity on a 10 cm Visual Analogue Scale (VAS; 0=no pain and 10=maximum pain).
Mean stool consistency was documented using the 7-point Bristol scale.24
Sample size calculation
Changes in the primary efficacy endpoint, total PAC-QOL score, of 0.5 points from baseline or between periods were considered clinically significant.22
A sample of 126 patients was estimated to afford a statistical power of 99.9% in detecting differences of 0.5 points in the PAC-QOL, with a precision of ±0.03 points in the 95% CI of the differences between means, in paired comparisons between periods, with a two-tailed alpha significance criterion of 0.05 (Sample Power, SPSS).
Statistical analysis
A descriptive analysis was made of frequencies and percentages for the qualitative variables, with calculation of the mean, SD and 95% CI, for quantitative variables.
Comparisons between variables were made using the Fisher exact test or the χ2 test in the case of qualitative variables and using the Student’s t-test for the comparison of independent groups if quantitative variables.
Monitoring of the quantitative variables over time was based on analysis of variance for repeated measures, applying Bonferroni or Games Howell corrections according to the homogeneity of variances for the control of multiple comparisons. Statistical significance was considered for p<0.05. The IBM-SPSS V.25.0 statistical package was used throughout. The Strengthening the Reporting of Observational Studies in Epidemiology guidelines for the presentation of information from cohort studies were followed.25
Results
A total of 126 patients were included. Ninety-five patients completed the 3 months of follow-up. Three patients discontinued the study due to physician decision; 10 discontinued the study due to patient decision; 1 patient was lost to follow-up; and 17 patients had died because of their oncological disease.
Clinical history and sociodemographic data
Table 1 shows the characteristics of the patients. Seventy-seven patients (61.1%) were receiving treatment for some comorbid condition.
Sociodemographic and clinical data of the patients
The main cause of the pain was the cancer (91.6%; n=109). Opioids that potentially trigger OIC at the moment of inclusion were fentanyl in 58.7% of the patients (n=74), morphine in 26.2% (n=33), oxycodone in 11.9% (n=15) and tapentadol in 2.4% (n=3). The pain treatment had been administered for an average of 6.2 months before patient inclusion in the study (95% CI 4.9 to 7.5).
A total of 31.5% of the patients (n=34) had a prior history of constipation. The mean duration of OIC was 3.8 months (95% CI 2.5 to 5.1), with a median of 1.4 months.
Treatments
The treatments prescribed for the management of OIC from its diagnosis to inclusion in the study were: lactulose (58), macrogol (58), enema (10), bisacodyl (13), paraffin oil (8), magnesia (5), sennosides (4), fibre (2), sodium picosulfate (2), lactitol (1) and psyllium(1).
The naloxegol starting dose was 25 mg/day in 86.7% (n=85) and 12.5 mg/day in 12.2% (n=12), while one patient received 6.75 mg/day.
During the study, 63.2% of the patients (n=43) received concomitant treatment with laxatives (28 unavailable data at database closure).
At baseline, 63.2% of the patients (n=74) were receiving chemotherapy and 85.2% (n=98) were receiving treatment with other drugs that could cause constipation.
Evolution of symptoms
A statistically significant increase in the mean number of days a week with complete spontaneous bowel movements from baseline (p<0.0001) was observed over all the study visits (figure 1).

Mean number complete spontaneous bowel movements per week.
The Bristol score improved significantly over time versus baseline (p<0.0001) from 2 at baseline to 4 on day 15 and the subsequent visits.
There was a significant decrease in pain intensity between baseline and the next visits (p=0.002 on day 15 and p<0.0001 at 1 month and 3 months), with a VAS score of 4.8 at baseline, 3.6 after 15 days, 3.1 after 1 month and 3.2 after 3 months.
Response to treatment
A total of 82.5% of the patients (n=85) responded to treatment with naloxegol after 15 days, 83.2% after 1 month (n=79) and 87.7% after 3 months (n=64).
The response after 3 months was analysed according to whether the patients received concomitant laxative therapy, and the dose of naloxegol administered. In those patients who did not receive laxatives during the study, the 3-month response rate was 88% (n=22): 75% (n=3) with the 12.5 mg naloxegol dose and 90.5% (n=19) with the 25 mg dose. In those patients who received laxatives in combination with naloxegol, the 3-month response rate was 88.4% (n=38): 83.3% (n=5) with the 12.5 mg naloxegol dose and 89.2% (n=33) with the 25 mg dose. There were no differences in response to treatment according to the organ affected by the cancer.
Constipation-related quality of life, evolution of the PAC-QOL score
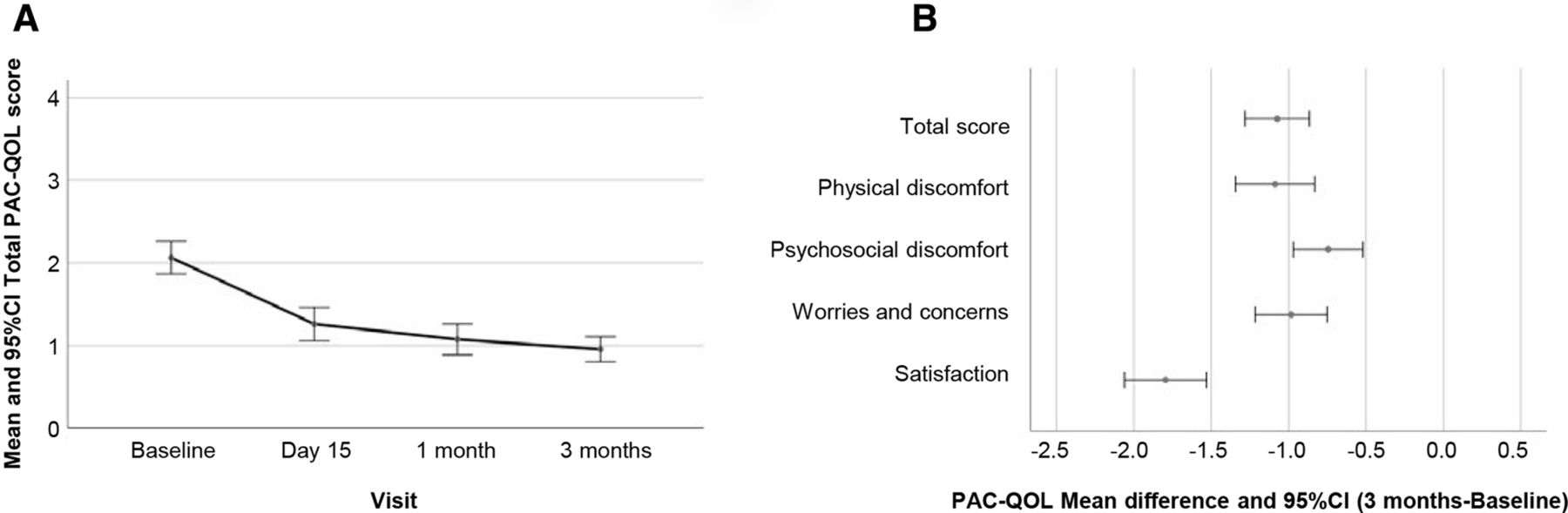
Clinically and statistically significant improvement (p<0.001) was observed in the PAC-QOL scores from baseline and between all the subsequent visits (n=58; figure 2). The proportion of patients with clinically relevant improvement in the total PAC-QOL score was 63% (n=58) after 15 days, 72.9% (n=62) after 1 month and 75.8% (n=47) after 3 months.

(A) Evolution of total Patient Assessment of Constipation Quality of Life Questionnaire (PAC-QOL) score from baseline to 3 months of follow-up (p<0.0001). (B) Mean differences (3 months- baseline) in total score and in the scores of each subscale of the PAC-QOL. Differences>0.5 points are considered clinically relevant.
Constipation-related symptoms, evolution of the PAC-SYM score
Clinically and statistically significant improvement (p<0.001) was observed in the PAC-SYM scores from baseline and between all the subsequent visits (n=58; figure 3). The proportion of patients with clinically relevant improvement in the total PAC-SYM score was 64.5% (n=60) after 15 days, 76.5% (n=65) after 1 month and 84.1% (n=53) after 3 months.

{kind=link}
{kind=link}
{kind=link}
(A) Evolution of total Patient Assessment of Constipation Symptoms (PAC-SYM) score from baseline to 3 months of follow-up (p<0.0001). (B) Mean differences (3 months—baseline) in total score and in the scores of each subscale of the PAC-SYM. Differences>0.5 points are considered clinically relevant.
Adverse reactions to naloxegol
Seventeen patients (13.5%) experienced some adverse reaction to naloxegol, mostly of a gastrointestinal nature. Table 2 describes the 24 adverse reactions observed. A total of 62.5% (n=15) were mild, 25% (n=6) moderate and 8.3% (n=2) severe. Six patients required treatment discontinuation and withdrawal from the study due to two severe, four moderate and two mild adverse reactions. During the first 3 months of follow-up, 17 patients died from causes related to their malignant disease.
Adverse reactions to naloxegol observed during the study
Discussion
The present study evaluates patient quality of life and the efficacy and safety of the treatment of OIC with naloxegol under real-life conditions. This is the first study in patients with cancer and OIC treated with naloxegol, since to date only data from case reports have been available.26–28 We observed statistically significant improvement of OIC-related quality of life assessed using the specific PAC-QOL questionnaire, and such improvement was noted from as early as 15 days after the start of treatment (p<0.001) and persisted during the 3 months of follow-up.
Improvement was clinically relevant in 63% of the patients after 15 days and in 75.4% after 3 months of follow-up. This significant improvement in OIC-related quality of life was evidenced in all the subscales of the PAC-QOL and in its total score. Improvement in patient satisfaction was also notorious, being threefold greater than improvement in the other subscales (figure 2).
Clinical symptoms efficacy assessed by the PAC-SYM questionnaire also yielded statistically significant findings (p<0.001) referred to both the total score and the scores of the three subscales (figure 3). The proportion of patients with clinically relevant improvement being 64.5% after 15 days and 84.1% after 3 months. In addition, the mean number of days a week with complete spontaneous bowel movements increased over follow-up and proved significant from as early as day 15 of treatment (figure 1). Stool consistency as rated by the Bristol score also improved. The treatment response rate was very high from 15 days (82.5%) and increased to 87.7% at the end of the 3-month follow-up period. This response could be observed before day 15 in most patients, but no visits were scheduled between baseline and day 15 of treatment, so no firm conclusions therefore can be drawn. The treatment afforded rapid improvement of patient quality of life and probably resulted in fewer physician and emergency room visits. And, although there are not enough data to conclude that the reduction is associated with naloxegol treatment, it was observed that pain was significantly reduced throughout follow-up, thus suggesting a possible relation. With this, naloxegol offers a solution to OIC, one of the main problems associated with opioid therapy. Regarding this, naloxegol demonstrated in previous studies, similar efficacy in treating OIC independently of maintenance opioid type, dose or duration of opioid use at baseline, although these data have not been explored in our analysis.29–31
The efficacy of naloxegol was evaluated in two pivotal phase III trials (Kodiac 4 and Kodiac 5), both of which were double-blind, placebo-controlled, two-parallel group multicentre studies with two naloxegol doses (12.5 mg and 25 mg). Concomitant laxative use was not permitted during naloxegol treatment. A total of 1325 patients with non-cancer pain and OIC were included. The duration of the treatment period was 12 weeks in both studies. In the pooled analysis of these trials, patients without an inadequate response to laxatives represented 54%. It was observed a significantly higher responder rate among the patients with an inadequate response to laxatives than in the placebo group (p<0.01), with both drug doses. The response rate after 12 weeks was 42.5% for the 12.5 mg dose (n=240) and 47.7% (n=241) for the patients receiving 25 mg of naloxegol.31 32
In our study, the treatment response rate was 75% (n=3) among the patients receiving 12.5 mg and 90.5% (n=19) in those administered 25 mg of naloxegol, in the absence of concomitant laxative treatment, the latter being a study inclusion criterion in clinical trials.31 32 Our results should be interpreted with caution, since the reported data are per protocol, the number of patients particularly in the lower naloxegol dose group was small and no patient control group was included. The findings therefore may be overestimated.
In the clinical trials with naloxegol, significant differences were only found in the PAC-QOL patient satisfaction subscale compared with placebo at 12 weeks versus baseline. There were no significant differences in the other subscales.32 No control group was available in our observational study to compare the improvements, which proved significant for all the questionnaire subscales.
The safety of naloxegol was mainly evaluated in four phase III trials, one of which lasted 52 weeks.33 The duration of the placebo-controlled trials was 12 weeks—this being a requirement of the EMA for studies of constipation.34 A higher incidence of adverse effects was reported in the group administered the 25 mg dose—the most common problems being gastrointestinal disorders, with a frequency of >5% (abdominal pain, diarrhoea, nausea, flatulence). These adverse effects occurred mainly in the first 7 days of treatment. The safety profile observed in our study is consistent with the safety description of the drug.
Our study has limitations inherent to its observational design under conditions of standard clinical practice. There was no control group, and the reported data were evaluated per protocol and are the result of an interim analysis. The findings therefore may be overestimated. It is also important to notice that, based in the general clinical practice, most patients were receiving fentanyl (58.7%) for pain treatment at baseline. However, it has been shown that the efficacy of naloxegol is not dependent on the type of opioid used,29–31 suggesting that these results could be extrapolated to other opioid treatments and administration routes. The subjects included in the study were patients with cancer, of which 63.2% were receiving chemotherapy and 85.2% were being treated with other drugs that could cause constipation. The clinical trials with naloxegol were conducted in patients without cancer, and the inclusion of patients with treatments that could cause constipation was limited. In this regard, a poorer response to treatment than seen in the clinical trials could have been expected, but this was not the case.
Based on the results obtained, it can be concluded that naloxegol as treatment for OIC in patients with cancer with an inadequate response to laxatives was more effective than expected. These findings should be confirmed in the context of a randomised clinical trial.
Acknowledgments
Thanks are due to the patients and to the Ethics Committees of the participating centres for their collaboration in this study.
References
Footnotes
Contributors MCD, CBZ, LCG, AJJL, IHG and ASY participated in the design and coordination of the study. BSL completed the design, monitoring and statistical analysis of the study, and for preparation of the manuscript for publication. RCS, MIBL-B, FGN, JLFP, GSB, PTT, IDM, AGM, ALO, APL, PSM, OHG and DMM reviewed and approved the final manuscript. AJJL, IHG, ASY and BSL are responsible for the overall content.
Funding This study was sponsored by Kyowa Kirin Farmacéutica S.L.U, Spain. The funders participated in the design of the study and the drafting of the manuscript.
Competing interests MCD, CBZ and LCG received payment from Kyowa Kirin Farmacéutica, S.L.U. for their participation in the design and coordination of the study. AJJL, IHG and ASY are employees of Kyowa Kirin Farmacéutica, S.L.U. BSL was contracted by Kyowa Kirin Farmacéutica, S.L.U. for the design, monitoring and statistical analysis of the study, and for preparation of the manuscript for publication.
Patient consent for publication Not required.
Ethics approval The study was approved by the Ethics Committee of Hospital Universitario Puerta de Hierro (Majadahonda-Madrid, Spain) on 22 May 2017 (no. 10.17). The study was carried out in abidance with the ethical principles of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data that support the findings of this study are available from the corresponding author, upon reasonable request.