Article Text

Abstract
Introduction Caregivers play a major role in providing all the support and care in daily activities for their relatives with dementia. To fully describe the influence of dementia caregiving on family caregivers’ life, we conducted a systematic review including caregivers’ perceptions about the positive and negative aspects of caring and the expressed factors.
Materials and methods We conducted a systematic review including articles from January 1998 to July 2020. Qualitative studies reporting family caregivers’ perceptions about their experiences and the effects/impact of dementia caregiving were eligible. Two authors extracted the data independently, and the analysis focused on the positive and negative aspects of dementia caregiving in caregivers’ life.
Results Eighty-one studies with 3347 participants were included in this review. The positive aspects of caregiving in caregivers’ life encompass personal accomplishment and strengthening relationships, which were enhanced by good medical counselling/formal care support and family/friends support. The negative aspects included emotional and social aspects experienced by caregivers. Other factors such as inappropriate medical/formal care support, illness progression and the costs of dementia contributed to negative appraisal.
Discussion and implications The findings provide insights into the holistic experience of caring for a person with dementia revelling the major positive and negative aspects underlying the caregiver role. The evidence emphasises the need ‘to focus on positive aspects’ and targeted interventions aimed at reducing the negative impact of caregiving, which has serious consequences on caregivers’ quality of life. A multicomplex intervention for dementia informal caregiving should be developed, committing the society to promote mental health, address these community needs and improve the quality of life of the person with dementia and their family caregivers.
- quality of life
- home care
- family management
- supportive care
- end of life care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Dementia is a clinical syndrome characterised by a cluster of symptoms manifested by difficulties in memory, disturbances in language and cognitive functions, changes in behaviours, and impairments in activities of daily living, and includes a range of neurological disorders characterised by memory loss and cognitive impairment.1 2 With the growth in ageing populations, the number of persons with dementia is increasing, with no sign of a cure for the disease. It is probably underdiagnosed, with an estimated half of primary care patients aged over 65 years not diagnosed by their primary care physicians.3 4 The most common form of dementia is Alzheimer’s disease (AD), accounting for 50%–70% of dementia cases. Prevalence has undergone a huge increase in recent years, and it has become one of the greatest healthcare challenges of the 21st century due to the high demand for medical, social and institutional care.5 6
Before institutional care, family caregivers play an important role for people with dementia, helping them in their daily activities, whose dependence increases with severity of the disease.5 7 8 Taking care of a person with dementia demands several logistic tasks, including personal care, housekeeping, administration of medication, processing financial transactions and other activities and with disease progression caregiving for the patient’s well-being becomes more important.1 9
The task of caregiving is complex and can lead to physical, mental and financial stress for caregivers. Emotions such as guilt, resentment, sadness and the effort expended, as well as the anticipated loss of the relative, emerge.9 As a result, informal caregivers suffer significantly higher levels of psychological morbidity, depression, stress and burden.10–12 The uncertainty about the future may create an ambiguous situation for family members and increase the burden on the caregiver.13 Despite these, some caregivers see their role as an opportunity to strengthen the relationship with their relatives.
Healthcare professionals have an important role in providing support to caregivers. They may refer caregivers for counselling, which has been shown to reduce caregiver distress, assist patients to stay at home longer, and inform caregivers about support organisations.5 There is evidence suggesting that caregiver needs are not being met by healthcare professionals, which leads to the decline in their physical and mental health.14 15 Caregivers’ perspectives are of high importance as these help to better describe caregivers’ role and identify potential ways to improve daily tasks, resulting in a more positive experience.
A large proportion of studies discuss the positive and negative influences of caregiving on particular aspects such as gender, nature of the relationship or caregivers’ age.7 16 17 To describe the task of caregiving, it is important to approach this as a global phenomenon, that is, understanding the caregiver’s needs and perceptions that positively or negatively contribute to their quality of life and their provision of daily support as caregivers. We conducted a systematic review of qualitative studies to understand the holistic experience of caring for a person with dementia, including not only the positive and negative aspects of caregiving through caregivers’ perspectives, but also the expressed factors that affect those experiences.
Materials and methods
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines18 and was performed to identify and summarise the impact of caring for persons with AD/dementia on family caregivers’ life through their own perceptions.
Search strategy and inclusion criteria
Two authors (PL, MR) performed electronic searches for relevant sources in OVID Medline, EMBASE, Web of Science, Scopus and PsycINFO. These databases were selected due to the high relevance of their indexed articles to this study’s topic. The results of this search were supplemented by hand-searching of the reference lists of the retrieved articles. Languages included were English, French and Spanish, with publication dates restricted to January 1998–July 2020. The start date of the review was the time when symptomatic treatment for AD was marketed, and the inclusion criteria for pivotal efficacy trials better discriminated AD from other dementias, namely vascular dementia.19 The studies published after 1998 were more consistent with our disease criteria and were therefore selected for this review.
The full search strategy and the inclusion/exclusion criteria are available in Box 1 (see additional file 1 of the online supplemental material for more details). Studies including a mix of participants (caregivers, care recipients and/or healthcare professionals) were included in the content analysis, but the perspectives of healthcare professionals and care recipients were excluded.
Supplemental material
Systematic review of literature: search terms, inclusion/exclusion criteria and information extraction
Search terms.
Alzheimer disease OR mild cognitive impairment OR cognitive dysfunction OR dement*.
Interviews OR interview* OR surveys and questionnaires OR survey* OR questionnair* OR focus groups OR geriatric assessment OR health impact assessment.
Caregivers OR caregiv* OR carer OR family OR famil* OR patient care.
Illness behaviour OR cost of illness OR activities of daily living OR quality of life OR self concept OR stress, psychological OR sick role OR outcome assessment health care OR health expenditures OR health care costs OR self-perception.
Cohort studies OR longitudinal studies OR follow-up studies OR prospective studies OR retrospective studies OR cohort OR longitudinal OR prospective OR retrospective.
1 AND 2 AND 3 AND 4 AND 5.
Limit 6 to year of publication: January 1998–July 2020.
Inclusion criteria.
Original qualitative empirical data.
Paper in English, French or Spanish.
Including family or informal caregivers of people with dementia and/or Alzheimer’s disease and/or mild cognitive impairment.
Methods including focus groups and/or survey/questionnaire and/or interviews.
Exclusion criteria.
Quantitative studies, reviews of literature, opinion-based studies and protocol studies.
Studies before 1998.
Not addressing caregivers’ perceptions.
Studies where caregivers’ perceptions were related to the results of intervention programmes.
Addressing other conditions than dementia and/or Alzheimer’s disease and/or mild cognitive impairment.
Addressing outcomes other than caregivers’ perceptions about caregiving daily life.
Information extracted from included papers.
Study description, setting and population.
Sampling criteria, number of participants and response scores (when presented).
Study methodologies and limitations, and methods of data analysis.
Outcome measures.
Key findings/themes/results and main conclusions.
Implications for policy and practice and suggested future research.
Bibliographic details.
We downloaded all articles into Mendeley and deleted the duplicates. The abstracts and full-text copies were scrutinised by two independent reviewers (PL, MR), who applied the predefined inclusion/exclusion criteria (see box 1), with disagreements resolved through discussion or via a third reviewer (MMR), with a presumption of inclusion in cases of doubt.
Data extraction
Two authors (PL, MR) extracted the data independently from each study: information related to authors, publication year, study aims, theoretical/conceptual frameworks, sampling/sample characteristics, analytical approach, summary and outcomes. The selected studies were analysed in order to explore the positive and negative aspects experienced by caregivers while caring for their relative and the expressed factors that contributed to these positive and negative appraisals. With regard to data extraction, divergences were solved between authors, and 100% consensus regarding data extraction was reached.
Quality appraisal
Two authors (PL, MR) independently assessed the quality of each study using the Critical Appraisal Skills Programme (CASP).20 We assigned yes/no to eight questions related to the study methodology, as listed in CASP: clear statement of the study aims, appropriateness of the qualitative methodology, research design, recruitment strategy, data collection, considerations of the relationship between the researcher and the participants, ethical issues and rigour of data analysis (see box 1 in the online supplemental material). We did not exclude any study during the quality appraisal as they might generate new insights.
Data analysis
Narrative review was selected as the method for data synthesis since the included papers were qualitative studies.21 Selected papers were carefully read by the authors (PL, MR). Data findings from the primary studies were independently coded and organised (keywords, short sentences and so on) into positive or negative aspects of caregiving or the expressed factors contributing to positive or negative appraisal. Two authors independently performed the data analysis and consulted a third researcher (MMR) when required. Finally, the two authors worked together to re-examine significant statements and identify excerpts and/or original quotations from the studies that could best illustrate the themes selected for this study.
Results
Type and quality of the results
The search strategy yielded 2376 publications, of which 118 were selected for full-text review, with 81 studies finally included in this systematic review (figure 1). The studies were analysed to identify informal caregivers’ perceptions about the positive and negative aspects of caregiving and the factors that contribute to those experiences (table 1). The characteristics of the included studies are presented in the online supplemental material, table 2. With regard to methods, 52 studies used focus groups; other methods included interviews, questionnaires and mixed methods (see the online supplemental material, table 3). A total of 3347 participants were included; 82.1% were family caregivers. Qualitative methods to identify the experiences/perceptions of family caregivers were found in all studies; a few studies also presented the views of patients with mild cognitive impairment, patients with dementia and former caregivers (these perceptions were not included in this review).

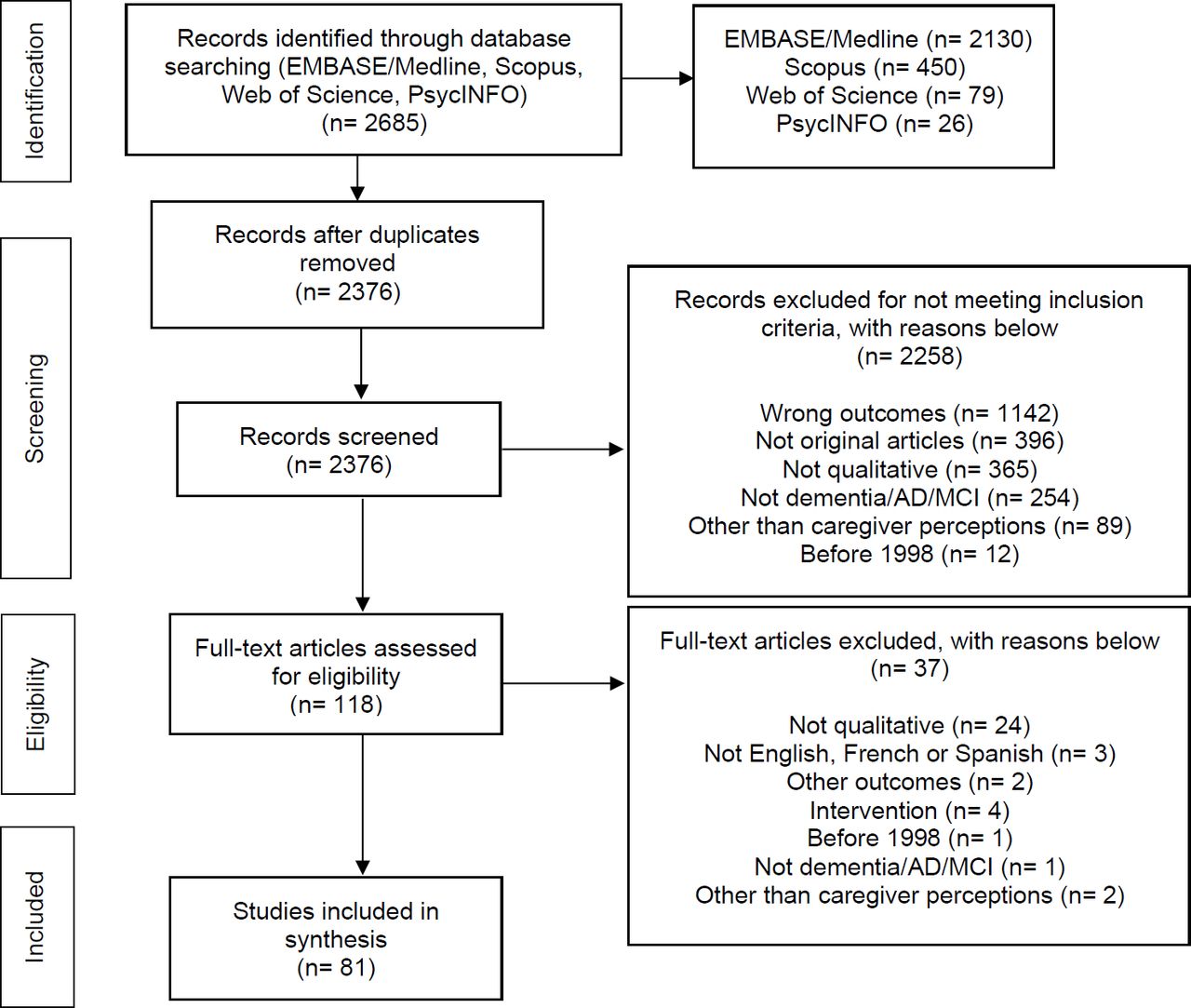{kind=link}
Study flow chart. AD, Alzheimer’s disease; MCI, mild cognitive impairment.
Examples of studies that included positive, negative or combined aspects of caregiving role (N=81)
Study quality
The quality of the included studies was assessed using CASP20 (see online supplemental material, table 1). Most studies used convenience samples, while some evaluated the representativeness of participants; however, all studies clearly reported the aims, design and sampling. Data analysis was fully described in 35 studies and partly described in 46 studies, while data collection was fully described only in 9 studies. All studies either fully or partly explicitly stated the ethical issues, but only one described the relationship between the interviewer and the participants.
Caregivers’ perceptions of the effects of caring for a person with dementia
Caregiving was described as a big life change: “It effectively changes your life. Your priorities change. Your lifestyle changes. Your attitude to the person you are giving care to changes. Your role changes.”22 Analysis of the included studies revealed positive remarks about the caregiving role, which were present in a small number of studies (18 studies), while negative aspects were present in 76 studies, including studies that combined both aspects. Examples of each and combined aspects are presented in table 1 (for all studies that encompass positive and negative aspects of caregiving, see online supplemental material, table 2).
The positive aspects found were presented as personal aspects experienced by caregivers that can be enhanced by good medical counselling and formal care support and family/friends support. Negative aspects were particularly related to emotional and social aspects of caregiving, and factors such as inappropriate medical and care support, illness progression and costs related to dementia (eg, formal care costs, medications costs and so on) enhanced negative appraisal (see table 2).
Main positive and negative aspects and related factors influencing caregivers’ role (N=81)
Positive aspects and the expressed related factors of caregiving according to caregivers’ perceptions
Providing support for the relative and having “made a difference” to their family’s life were considered to have positive effects on caregivers’ life and were a relief for caregivers, as they were able to fulfil their obligations as son/wife/daughter or others:
(…) What I am looking to do is just staying home and watch my husband. That’s what I have to do. And if that’s what I have to do, I don’t mind doing that.
It gives me great joy to give back to my mom and…I tease her…uh…on a good day, and I say “Aren’t you glad you took good care of me, because you set that example?” And she’ll laugh and I’ll laugh and…and it gives me great joy, because she…uh…was/is a great mother. And uh…and…and now, it’s my turn to be a great daughter.23–26
For some family caregivers, the chance of doing meaningful activities together and be able to return the favour to their parents/family members was indicated as being grateful: “I enjoy the time with my mother…I love to hear her laugh…We talk all the time in the car; we pray together, watch TV.”26 27 Respect for the individuality of the person with dementia was reported as crucial to caregivers, who were grateful to know that the individuality of their family members was being respected in the nursing home:
I think their individuality and their dignity is vital.
They have all got their own (personal) things (in the nursing home).28
By having their own things, patient well-being and dignity appears to guarantee to turn initialization into a more personal experience.
The main expressed factors that contributed to the positive aspects of caregiving were related to good medical counselling and formal care support, as well as family and friends support (table 2). Access to useful information about the disease and its evolution was considered essential to caregivers. Acquiring knowledge helps caregivers to better assume caregiving role and prepare them to prevent and deal with specific situations: “I would like to know. I mean I am worried about the future…Because I don’t know anything!”29
Appropriate medical counselling, formal support and healthcare professionals support for patients were found to be good resources to overcome caregiving challenges and decision-making processes that rely on caregivers: “Well, for me, what would improve my quality of life mostly is to have better support from healthcare professionals, (…) just keeping him clean is extremely challenging (…).”30 Caregivers considered good aspects of formal care when the staff “have the knowledge and techniques on how to handle the residents and their behaviours” and “That it was good to see their relatives in a safe, secure and loving environment.”31 Caregivers also benefit from medical and psychological support where the disease can be acknowledged and where they can be understood: “The regular visits to the psychologist were very helpful. It is really important you have someone to talk to during the dementia process who understands you.”32
The need for an early diagnosis of dementia was quite evident, mainly due to the bad experiences and endless diagnostic procedures previously experienced, but also due to the relief felt after the diagnosis: “I felt very relieved when we finally got the diagnosis…I just felt validated that finally someone knew what we knew.”33 Through caregivers’ perception, early diagnosis has the positive effects of relief and care improvement, thus allowing for a more effective caring process for their families afterwards:
Well, if I had known that the man was sick, first of all, he wouldn’t have been left alone as long as he was. Second of all, I wouldn’t have blamed him for his actions. I would have known it was the disease. We did a lot of damage emotionally to him as well as to ourselves, and there’s a lot of guilt associated with what we had done, so I think diagnosis as early on as possible is the best possible thing that can happen.33
Family and friend support was another factor that positively enhanced the experience of caring. The value of old friendships that remains after diagnosis helped reduce caregivers’ feeling of loneliness: “(…) Many of our friends, if anything, they’ve stepped up and they helped us.”34 35 Family support is particularly important when it provides free time for the principal caregiver to do his own activities: “She would stay with my sister for approximately three months.”36 This aspect was regarded by caregivers as very positive to their quality of life. Unfortunately, most admitted to be single caregivers for their relative and have no spare time for themselves or other activities besides caring.34 35
Negative aspects and expressed related factors of caregiving according to caregivers’ perceptions
Caregivers’ perceptions about the negative aspects of caregiving comprise emotional and social aspects, such as fear, worry, stress, sadness, social isolation and problems accepting their relatives’ diagnosis. Additionally, caregivers experienced concerns about the future since they do not know what to expect and for how long they can ensure the emotional and economic support for themselves and their relatives’ well-being.
Mental, emotional and physical efforts are seen as requirements to deal with patient sleep disorders—“I can’t handle this anymore; I’m absolutely buggered from no sleep at all night”37—and behavioural changes (which in some cases lead to physical/verbal aggressions), with some caregivers declaring their own need for therapy:
In fact, I do need therapy, too. I mean if there are not two or three people to care for the patients, you are psychologically affected. I am a prisoner at home.
For a couple of times I cried. They say boys do not cry, but I did….
I sometimes have nervousness, anger and crying attacks. (…) I used to be full of life; I used to like visiting and having holidays. I can say that I cannot bear this situation anymore.38
The caregiver role demands too many hours for care, with no time for personal life, which is reflected in caregivers’ difficulties in maintaining their professional and social life, and their responsibilities as parents:
I can’t leave him. For 24/7 I’m with John.39
I would say if you’re going to be a caregiver it’s a full-time job. You don’t have time to do anything else if you’re going to do it right.40
(…) I think that there’s such isolation for the caregiver because you often don’t have someone to talk to unless you have a large family. I tend to not have friends that, they don’t want to hear anything that you are doing this.41
I live a little way away and I’ve got four children; and that’s hard in itself. I have to look after her as well. Some days, I might be having a crisis before I have even seen her.42
For caregivers, there was a permanent concern about their relatives’ well-being and the capacity to provide safe and effective care which could prevent the possibility of serious injuries to occur, particularly fractures due to falls. The comorbidities that persons with dementia usually have, also increase the need for adaptation of care required, including special food intake.:
(…) He cannot swallow and coughs each time he swallows and it blocks his throat.
My mom was a diabetic for 40 years. If she didn’t eat in the morning, hypoglycemia was inevitable. Whenever my mother would refuse eating breakfast, I would become angry and mom would also fight and insist on not eating.38 43
Food was an important aspect for some caregivers, since the high level of calories needed to support their relatives has consequences on their own weight and health. Also, for many of the male caregivers, the concern with the process of feeding their relatives was new, leaving the need to learn new things, besides their relatives’ condition.44
For some caregivers, the time of diagnosis brought great frustration due to inexistent communication with health services, constant change in formal care providers and lack of information: “I don’t think that any of the doctors that we were involved with ever offered any help as far as what to do next.”33 45 46 The process of dealing with health and social care services for the person with dementia was described as a “battle” or “fight”.47 After the diagnosis, the uncertainty about the future and the inability to accept their relatives’ condition led to stress, frustration and sadness.35 48 49 For caregivers, it was difficult to deal with the fact that they were not recognised by their relative with dementia: “And I think that the dementia would then progress rapidly to a stage where she no longer recognises anybody.”24 Some caregivers admitted to start grieving the loss during the course of the disease:
I have been grieving losses over the whole period of illness; there was a loss of person before a loss of body.50
I started grieving years ago when mother didn’t recognize us…That’s when I lost my mother…When she physically died I felt like I lost my baby.51
It may be a bad thing to say but I’m hoping before she starts really seriously deteriorating she’ll pass on.35 50
The social isolation due to the loss of old friendships and the lack of family support seem to have a huge negative impact on caregivers’ personal and social life.52 Over time, caregivers tried to adapt to the circumstances and sought professional help, aiming to deal with their exhaustion and emotional problems:
I am having emotional problems from the stress and sadness of seeing such a low quality of life in my mother.
Dementia is an emotional process which you enter together. Eventually you reach your limit (…).32
I did not get enough emotional support.
I needed more emotional support from friends and community.36
For some participants, caregiving was considered an obligation that results in a higher emotional impact: “I hardly cry, I have almost never cried. I got distressed and felt ill. I tried to manage it by myself. I was obliged to accept it when nobody gave me a hand.”38
The inappropriate medical and formal care support, the daily perception of disease progression, and the high costs of illness were the main expressed factors that contributed to the negative aspects of caregiving (table 2).
Formal care services were largely associated with patient isolation and superficial or poor care:
In an ideal world one would not allow the patients to sleep all day.28
We had home care [for mother] until they [home care staff] got accused of stealing, got fired, got thrown out….53
The lack of formal support made caregivers feel they are left alone: “I just don’t understand why they [home care staff] are so unhelpful…I think something needs to be done, because we don’t seem to get any help really from anywhere. You’re just a bit left on your own.”54 Inappropriate medical care was also reported by caregivers: “I was kind of astonished that the doctors were unsupportive, not only unsupportive, really very negative…this is a doctor and he’s telling me not to treat my father….”55 Diagnosis commonly triggered search for better medical counselling:
I didn’t get any help at all. He just said that my husband had depression. In the finish and because I kept going back…and anyway it wasn’t…and I ended up having to pay for a specialist to get him referred to try and get him a diagnosis…We didn’t get any help at all. I didn’t get sent anywhere….56
The decision-making process is typically the responsibility of caregivers, leading to an impact on their own feelings and well-being. For example, placing the feeding tube, resuscitating and even choosing permanent formal care, such as a residence or nursing home, are very difficult decisions to make and bring feelings of sadness and guilt:
I promised faithfully that he would never go to a residence, and I still feel guilty.57
I mean it’s totally on my shoulders too. And sometimes the amount of guilt is there, I mean it just weighs me down so much. But then I have to split myself, I still have kids at home, and I have to split myself there too.40
Resuscitation was the biggest decision…I consulted with my children and my wife’s sisters and they were all in agreement…she has gone through enough.58
Another negative factor that contributes to increased burden in the caregiver is the constant loss of patient competences, losing their ability to do daily activities such as walking, dressing, going to the bathroom, bathing, driving or cooking in an independent way, overloading the caregiver:
I’ve had to do it all.
I bathe him because he is afraid. He does not finish it and leaves. He does not completely shave. For example: he cuts the right side of the moustache and leaves the other side. He eats but does it in a mess.23 26 38 44 59 60
Witnessing the daily progressive health decline of their relatives, especially in the later stages of the disease, is a process that has significant impact on caregivers: “In the later stages it’s so difficult for them to indicate what their needs are.”24 28 31 61 With the patient’s loss of abilities, caregivers try to adapt to the circumstances and might consider getting professional help at this point.35 54 59 62 Another negative aspect that has a major impact is behavioural change, which in some cases leads to physical or verbal aggressions:
He’s very much reliant on me (…) He’s suddenly becoming aggressive, and gets angry really with no reason at all….63
She also gets quite aggressive when it comes to her kind of personal care really. You know she doesn’t like having a shower, having her hair washed….64
It is very hard for me to handle her behaviour (…) I know that you shouldn’t mention it and/or joke about it. But I’ve noticed that I still do it. I’m still having a hard time accepting how much my mother has changed (…).65
On top of the above-mentioned negative aspects, the cost of the illness had a huge negative impact on caregivers’ daily living and well-being. Without a job in some cases, keeping up finances with the high cost of bills and home care is also a constant worry and is seen as a barrier to accessing formal care:
I can’t afford a decent one (home care service).
Cost is a barrier for lots of people. You know, there’s a limit to how much home care they use because of the cost.48 66
Another concern of caregivers is the duration of the disease:
I knew we had money if mom lived for one to two years, but if she lived for 20…it was a big worry and a burden.
I don’t have an unlimited amount of money for my mom. I am trying to sell her properties and get her settled. I am continually worried about resources.51 59
Thus, financial guidance/support for this community is of great relevance not only to guarantee daily basic support of food, bills and medications, but also the need for institutionalisation and all other support that patients may require during their lives.
Discussion and implications
The current review focused on the perceptions of informal caregivers with regard to the holistic experience of caring for a person with dementia, including the positive and negative aspects. The included studies reviewed the diverse feelings and emotions that caring brings to caregivers. The diagnosis of dementia seems to generate positive consequences in the relationship between the caregiver and their relatives, contributing to a stronger relationship than before.17 This strengthening of family ties has also been reported in other diseases such as cancer.67 This fact may be related to the family companionship that is needed to face the disease and is probably related to the type of disease. Chronic diseases and/or a poor prognosis are seen to cause a very high burden to the patient, but can be reduced with the family being closer together. As described by Gitlin et al,68 most of the caregivers found in caregiving a chance to “return the favour” to their relatives and the opportunity to do activities together, reducing both caregiver burden and behavioural symptoms of dementia, which is in agreement with our findings. Findings from Elnasseh et al69 are consistent with past literature showing that the quality of previous familiar relationship is relevant when a family member becomes a caregiver. In families with healthier dynamics, caregivers are more likely to have greater personal strengths, while families with poor affinity are more likely to experience increased caregiver burden.43
Finding good medical counselling and formal care support, as well as the the opportunity to enhance family cohesion, and the presence of friendships, especially old friends who remain after the diagnosis, were factors that contributed to positive appraisal. As previously demonstrated by Vellone et al,70 all kinds of help and support are welcomed by caregivers, as these give them free time for themselves. Sharing caregiving tasks is a concrete way to reduce caregiver stress, with the free time being used by caregivers for activities such as going to the gym, taking a walk, going out with friends or just taking a nap. After relaxation, the caregiver would be much more ready to better take care of their relatives. The availability of formal care support, in addition to positive experiences with formal care, and good home care/day care services are important to caregivers, once they have perceived the knowledge, security and dignity needed to care for a person with dementia. Furthermore, good formal care can support caregivers in their role, reducing the burden and the negative impact of their daily routine. A recent review by Yu et al describes the positive influences of caregiving related to caregivers’ personal issues, highlighting feelings such as gratification and meaning in life, which is in accordance with our findings.71 Additionally, we identified other factors that contributed to positive and negative experiences in caregivers’ daily life. This knowledge is crucial to the development of measures/programmes targeted at caregivers, which should consider caregiver concerns, but also empower them by highlighting the positive aspects and providing support (good formal care services, family support and so on). The result will broaden the spectrum of action of these types of programmes and improve the caregiving experience on several levels.
The imbalance of the negative over the positive aspects of caregiving has been shown in previous studies, with implications for both mental and physical health effects in caring.14 15 A study of Pinquart and Sörensen72 suggests that caregiving of individuals with dementia is more stressful than caring for individuals with other diseases. This phenomenon is probably related to the increased amount of time that caregiving for a person with dementia may involve, resulting in loss of spare time and consequent social isolation.9 Most of the caregivers sacrifice their activities and hobbies, restrict their time with friends and family, and give up employment or reduce time at work. Therefore, caregivers tend to lose their meaning in life, or set it aside, leaving an opportunity for mental health problems to emerge, which can worsen in the future as a result of the emotional burden they are exposed to.73 74 Anticipated loss is common in caregivers, and as previously described in the literature grieving over the whole period of illness increases the possibility of having a postdeath complicated grief.75
The health of the caregiver has been studied by Widera et al,76 who suggested that caregivers are less likely to engage in preventive health measures, leading to increased risk of mortality. One factor that may be contributing to this situation is the financial burden associated with caring for a person with dementia. Moreover, the daily overload, the patient’s dependence and the decision to stop working in order to care for their loved ones lead to postponement of medical examinations among caregivers, negatively impacting their health status.76 77 Usually, caring for their relatives becomes a priority; however, this process is often done alone, resulting in the tendency of caregivers to forget to take care of themselves. Healthcare professionals have a central role in improving access and quality of health services to caregivers (which have been shown to reduce caregiver distress and assist patients to stay at home longer). However, little has been done with regard to the promotion of a healthier life for caregivers, who are known to be in need of good health support and monitoring.5 76 Little is known about caregivers’ health and quality of life, and this is an important issue that requires more studies that better describe the general health status of caregivers and provide directions to improve their health condition. The general health of caregivers deserves a great deal of attention as negative health outcomes contribute to the risk of future serious health problems, compromising not only the caregiver’s health but also the care that is being provided to the patient.78
Previous studies have reported that the patient’s dependence on activities of daily living is described by caregivers as one of the hardest things to deal with, which is due to the amount of care that needs to be provided. This is in accordance with the findings found in the studies included in this review.79 80 Throughout the progression of the disease, the patient’s behavioural symptoms (agitation, sleep disturbance, wandering and apathy) and psychological symptoms (anxiety, depression, delusions and hallucinations) have a significant impact on caregivers, proving the negative experiences of caregivers.
Moreover, the effects of night agitation and sleep disturbances experienced during caregiving lead to poorer subjective sleep quality and higher rates of daytime sleepiness among caregivers of persons with dementia compared with non-caregivers. These factors, combined with daily routine, disease progression and the patient’s dependence, can lead to caregiver exhaustion.81
The cost of the illness had a huge impact on caregivers’ routine, with the increased cost of formal care and medication becoming a concern. Cost is probably the reason caregivers resort to formal care as the disease becomes more severe, resulting in behaviour problems and more disabilities.82 83 Supporting a person with dementia in their own home costs less than bringing them to a care home. As previous literature suggests, the transition from informal to formal care occurs mainly in the later stages of dementia and is considered as supplement to care since the caregiver remains present in all processes.84 Additionally, caregivers attribute the change from informal to formal care as a failure of their responsibilities or make them feel they are bad family members.85 86 The long waiting lists and the costs were further barriers that delay access to these services.
The economic environment of caregivers is never too comfortable since they are caring for their relatives and not being paid for this full-time job. As informal care is unpaid, it is viewed as a costless substitute to formal care. However, informal caregiving is not free of costs, which makes it relevant to estimate the value of the hours that caregivers spend on caring for their relatives in order to better know the monetary costs of informal caregiving and develop better financial support to these specific cases. Timely access to dementia care services and fairer costs are crucial to reducing informal caregiver burden and to increasing the quality of life of patients and caregivers.87
Although it may be thought that the caregiver’s role is less important with the patient’s admission to a care facility, the caregiver remains involved in terms of important legal, financial and healthcare decisions.88 89 The decision-making process becomes tougher with the associated ethical and emotional responsibilities. Family, friends and medical support is critical as this allows caregivers to better decide and deal with the feelings associated with the decision.90
Due to the increasing complexity of caregivers’ responsibilities, training programmes are important to help caregivers understand and manage care recipients’ behaviour problems and thus reduce negative experiences.91 However, despite the several interventions developed with the goal of alleviating caregiver burden, the experience continues to be very negative for caregivers. Why are these programmes/interventions not having the expected results of decreasing burden among informal caregivers? Caregivers are mostly women and elderly. Are these interventions well set to the target population? Do these programmes really fulfil the needs of families on an individual basis? It is suggested that personalised and multicomponent interventions, including a diversity of services (directed at the patient and the caregiver), will decrease burden, improve quality of life and enable home care for longer periods prior to institutionalisation.92 The transition to formal services is postponed by family caregivers who, despite all the negative aspects of caregiving, chose to care for their relatives and provide them the best care they can. Interventions should demystify institutionalisation as a failure of the caregiver and should focus on facilitating a healthier transition to warrant patients and caregivers a sustained well-being for as long as possible. Also, it is important to provide interventions not only to caregivers, but also to former caregivers (who are usually neglected). There is evidence that the grieving process can be very stressful and can lead to depression.
The number of people suffering from dementia is expected to increase in the coming decades, and there is a need to strengthen informal caregiving to meet not only the care recipient’s needs, but also the caregiver’s needs. Adequate knowledge on the aspects that caregivers describe as positive and negative in caregiving experience and providing tools to level these aspects are urgently needed. Overall, a multicomplex intervention for dementia caregiving should be developed, with the entire society being invited to promote mental health, address caregivers’ needs and improve the quality of life for the person with dementia and their family caregivers.
Strengths and limitations
The strength of this systematic review is its description of the phenomenon of caregiving for a person with dementia, through the views of informal caregivers, encompassing both positive and negative experiences. The use of CASP for quality appraisal by two independent researchers strengthened the results. However, some studies presented methodological limitations that may impact the level of evidence, as some of the studies did not use appropriate theoretical frameworks, which is a limitation of qualitative research. The comprehensiveness of caregiver experiences might be limited because most studies did not primarily examine caregivers’ positive and negative experiences. The focus of the individuals included was on specific issues such as caregivers’ perceptions in formal care, family support, time of diagnosis and so on, and consequently reported limited aspects about the entire experience of caregiving.
Only qualitative studies have been included, and the results of quantitative studies were excluded. In addition, including only informal caregivers’ perceptions resulted in the exclusion of views of persons with dementia and formal caregivers. It is also important to consider other aspects of caregiving. Additionally, care recipient and caregiver characteristics such as demographics, relationship, gender and so on, which might influence caregiver experience, were not considered.
The study findings have important implications for the development of interventions that comprehensively address caregivers’ individual needs based on their experiences, and demonstrate there is a need for more rigorous qualitative studies that explore the perceived positive and negative aspects of caregiving. Altogether, these studies may generate new insights into the planning and design of more robust and flexible intervention programmes.
Ethics statements
Patient consent for publication
Acknowledgments
The authors acknowledge 'Fundação para a Ciência e Tecnologia (FCT)' Portugal and Merck Sharp & Dohme Portugal.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been updated since it was first published. The article type has been changed to Systematic review.
Contributors PL and MR were responsible for study conception, design and drafting of the manuscript. JC created and tested the research strategy. MG and MMR reviewed and made critical revisions to the paper. MMR supervised the study.
Funding This review was funded by the 'Fundação para a Ciência e Tecnologia (FCT)' Portugal and Merck Sharp & Dohme Portugal (grant number PDE/BDE/120498/2016).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.