Article Text

Abstract
Background Although the effectiveness of early palliative care for patients with advanced cancer has been demonstrated in several trials, there has been no detailed published description of an early palliative care intervention.
Method In this paper, we delineate the iterative conception and systematic evaluation of a complex intervention called team-based outpatient early palliative care (TO-EPC), and describe the components of the intervention. The intervention was developed based on palliative care theory, review of previous palliative care interventions and practice guidelines. We conducted feasibility testing and piloting of TO-EPC in a phase 2 trial, followed by evaluation in a large cluster randomised trial and qualitative research with patients and caregivers. The qualitative research informed the iterative refinement of the intervention.
Results Four principles and four domains of care constitute a conceptual framework for TO-EPC. The main domains of care are: coping and support, symptom control, decision-making and future planning. The main principles are that care is flexible, attentive, patient-led and family-centred. The most prominent domain for the initial consultation is coping and support; follow-up visits focus on symptom control, decision-making to maximise quality of life and future planning according to patient readiness. Key tasks are described in relation to each domain.
Conclusion The description of our intervention may assist palliative care teams seeking to implement it, researchers wishing to replicate or build on it and oncologists hoping to adapt it for their patients.
- cancer
- palliative care
- palliative medicine
- early medical intervention
- outpatients
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The effectiveness of early palliative care for patients with advanced illness alongside disease-directed treatment has been demonstrated in trials1–6 and systematic reviews.7–9 Most of this evidence stems from trials in patients with advanced cancer, with interventions of specialised outpatient palliative care teams in tertiary care settings.8 9 In order to implement these interventions, or to replicate or build on them for use in other trials, a complete published description of the intervention is needed.10 Although previous papers have described the operational functioning of outpatient palliative care clinics11 12 and conducted qualitative analyses to assess the key content of palliative care visits,13–15 there has been no detailed published description of an early palliative care intervention.
Early palliative care is a complex intervention with several interacting components. The process of conceiving and evaluating complex interventions is described as having four phases: development (evidence base and theory), feasibility/piloting, evaluation and implementation.16 This process is iterative rather than linear, with refinement or redevelopment of the intervention occurring after piloting, evaluation or implementation. In order to standardise and deliver complex interventions outside the context in which they were developed, it is important to identify fixed, essential aspects of the intervention that are central to its functioning.10 17 These essential elements relate to the main goals that the intervention is intended to achieve. Qualitative research can help to define these key elements, show how the intervention achieves its results and detect possible barriers to its implementation.18
In this paper, we describe systematically the conception of a complex early palliative care intervention, which we have called team-based outpatient early palliative care (TO-EPC). We describe the development of this intervention and its conceptual framework, which encompasses four principles and four domains of care derived from our qualitative research. We relate these principles and domains of care to the tasks of the initial consultation and subsequent follow-up visits, and provide details regarding their delivery. This descriptive paper may assist palliative care teams seeking to implement this early palliative care intervention, researchers wishing to replicate or build on it and oncologists hoping to adapt it for their patients.
Conception and evaluation of the intervention
Development of the TO-EPC intervention
The conception and evaluation of TO-EPC are outlined in figure 1. The initial conception of the intervention was based on palliative care theory,19–22 review of previous palliative care interventions23 and practice guidelines.24 25 The central tenet was that palliative care should be directed at alleviating suffering, regardless of the patient’s stage of illness, treatment status or readiness to engage in end-of-life planning. Patients and their families are provided with timely care aimed at improving quality of life through the early identification and treatment of physical, psychosocial and existential concerns.19 These concerns are addressed through team-based, family-centred care, delivered mainly by a palliative care physician and nurse, in collaboration with other interdisciplinary team members, community healthcare providers and the referring oncology team.

Conceiving and evaluating TO-EPC. The intervention was developed and revised following the four phases described by the Medical Research Council guidance on developing and evaluating complex interventions: development (evidence base and theory), feasibility/piloting, evaluation and implementation.16 TO-EPC, team-based outpatient early palliative care.
With these principles of care in mind, we developed an outpatient palliative care clinic and acute palliative care unit, which together provide the structural basis for TO-EPC.12 The outpatient clinic initially began once weekly in a borrowed space, and gradually expanded to other locations as it outgrew its space. While the clinic is now housed in its own freestanding space, the overall longitudinal structure of early palliative care provided in the clinic has remained constant, and is further described below (see section ‘Longitudinal structure of TO-EPC’).
Feasibility testing and piloting
We conducted a phase 2 trial, in which we evaluated the efficacy of TO-EPC.26 There was a significant improvement of physical and psychological symptoms, and satisfaction with care, 1 week and 1 month after a single visit to the outpatient palliative care clinic. Based on these results, we planned a larger phase 3 trial of the intervention, for which we extended the follow-up period to 4 months, and included two comprehensive measures of quality of life.4 The latter decision was made based on the central aim of palliative care to improve quality of life through the early identification and treatment of symptoms and other problems.19
Quantitative and qualitative evaluation
Our evaluation of TO-EPC included the phase 3 trial mentioned above,4 as well as qualitative research with patients and caregivers.15 27 28 The cluster randomised controlled trial included 461 patients with advanced cancer who were randomised to TO-EPC or standard oncology care. There were significant differences favouring the intervention group in quality of life and symptom control for patients, and satisfaction with care in both patients and caregivers.4 29 A subset of 71 trial participants completed qualitative interviews for a grounded theory substudy.15 27 28 The results of this qualitative research informed the theoretical framework for the intervention.
In qualitative interviews following completion of the cluster randomised trial, patients and caregivers described differences in the delivery and focus of care in the palliative care clinic compared with standard oncology care.27 From the point of view of patients and their caregivers, the main differences in the delivery of care were: open-ended, patient-led visits versus structured, physician-led visits; a personalised versus traditional medical relationship; flexible versus time-constrained visits and being actively listened to versus needing to be assertive. The main differences in the focus of care were: an emphasis on symptoms rather than managing cancer; providing holistic care versus directing cancer treatment; attending to the person versus focusing on the disease and including the family versus care limited to the patient. Specifically, patients and caregivers who received early palliative care described the care they received in four domains: prompt, personalised symptom management; holistic support for patients and caregivers; guidance in decision-making and preparation for the future.15
In addition to describing these positive aspects of the intervention, patients and caregivers also described apprehension related to palliative care and its association with death.28 This stigma surrounding the name ‘palliative’ was conceptualised as a potential barrier to early palliative care that needed to be addressed more explicitly within the intervention.
Implementation
Based on the positive results of the phase 3 trial and increased demand for early palliative care at our centre, we received funding for a freestanding 12-room palliative care clinic. This clinic became a hub for early palliative care intervention, as well as for academic activities, including research and education. Internationally, systematic reviews confirmed the association of early palliative care on positive outcomes for patients and caregivers,7–9 and early palliative care was recommended in clinical practice guidelines.30 Locally, the results of the randomised controlled trial affirmed the efficacy of the intervention, while the qualitative research iteratively informed the further development of TO-EPC and its conceptual framework.
Iterative redevelopment of TO-EPC
In order to ensure fidelity of the intervention, we had previously created a checklist of tasks to be completed by physicians, based on addressing physical, social, emotional and spiritual elements of quality of life.4 However, these tasks lacked a formal conceptual framework. Based on our qualitative research, we have created a conceptual framework outlining four principles (answering the question: How should care be provided?) and four domains of care (answering the question: What core elements of care should be provided?) (figure 2). We have mapped the tasks to be completed during the initial consultation and follow-up visits on to the principles and domains and revised this model based on input from palliative care team members. This exercise ensured that tasks were described fully rather than being taken for granted, remained centred on needs expressed by the patient and family, and were clinically relevant. The resulting model, which is detailed in the sections that follow, provides a structure that facilitates consistent implementation of the intervention.

Outline of conceptual framework for TO-EPC. TO-EPC, team-based outpatient early palliative care.
Description of the intervention
Longitudinal structure of TO-EPC
We have previously described the overall longitudinal structure of early palliative care.12 26 The core outpatient palliative care team consists of a specialist palliative care physician and a registered nurse with palliative care certification. Oncologists pre-emptively refer patients to the palliative care team early in the course of advanced disease, to ensure integrated, collaborative, team-based care. The patient is followed by both teams, who remain in close communication with each other as well as with the patient’s family physician and with nurses from community care services. Advance care planning is initiated, and a transfer of care eventually occurs to the home or inpatient palliative care setting, in keeping with the preferences and needs of the patient and family (figure 3). The formal intervention includes care at least once monthly for 4 months,4 but care is generally continued until the end of life or transfer to a different care setting. Visits may need to be more frequent depending on patient need; extra visits for urgent concerns are often necessary.
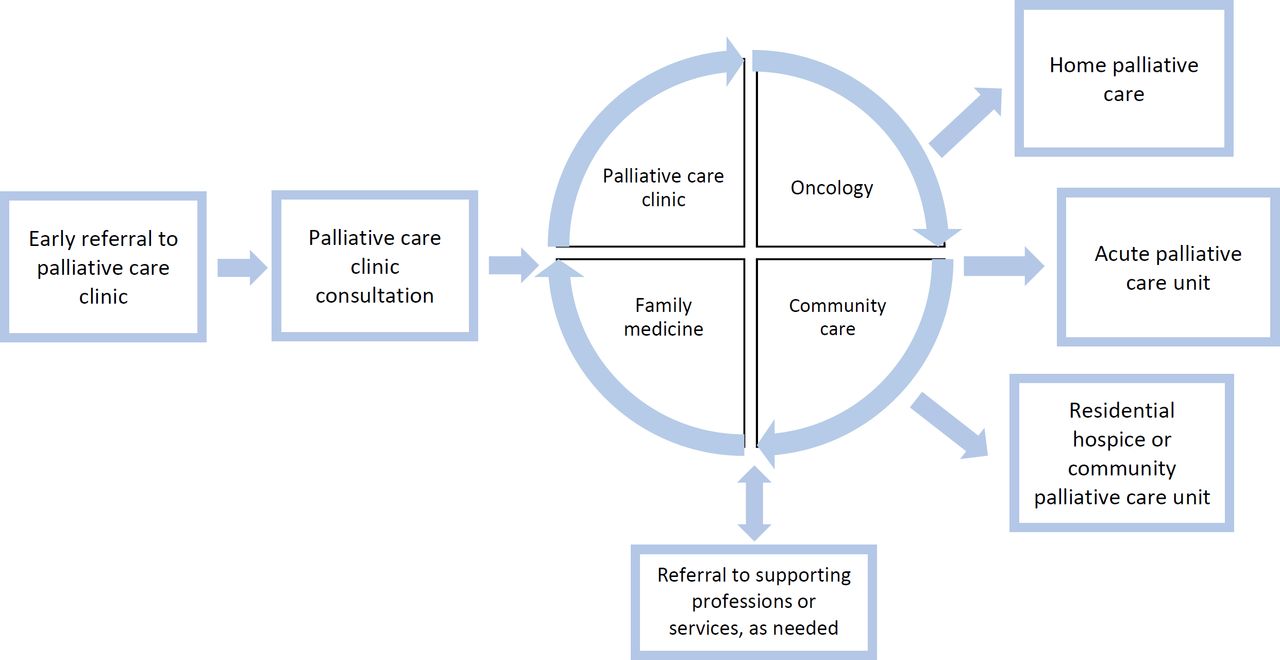
Longitudinal structure of TO-EPC. Patients are referred to the palliative care clinic by their oncologist or family physician, and receive longitudinal collaborative care in the clinic collaboratively with oncology, their family physician and the community care team. Referral to supporting professions or services occurs as needed and may include medical specialists (eg, radiation oncology, anaesthesiology, interventional radiology and ophthalmology) or interdisciplinary supportive care services (eg, psychologist, dietician, wound care specialist and spiritual counsellor). TO-EPC, team-based outpatient early palliative care.
The initial consultation
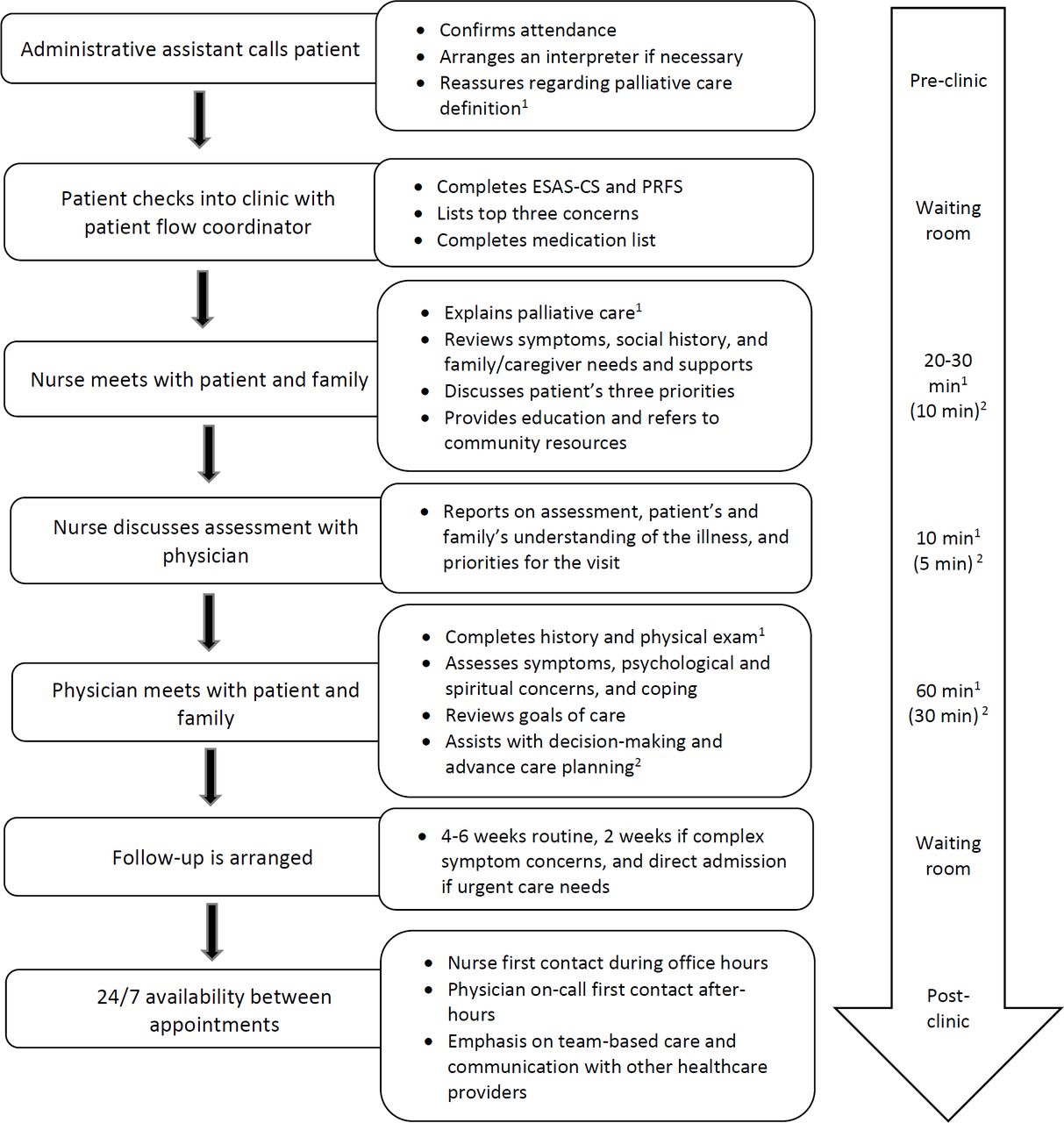
The initial consultation is a thorough assessment that lasts between 1 and 2 hours. The overall process for this consultation has been described previously12 and is shown in figure 4. Key tasks are described in table 1, with reference to principles and domains of care shown in figure 2. The main domain for this first visit is ‘coping and support’; the main tasks are to explain palliative care, initiate the therapeutic relationship and assess supports and coping. Symptoms are also addressed but are often minimal at this early stage; decision-making and future planning are explored according to patient readiness, and are generally deferred to future visits.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Flow diagram of consultation process in the palliative care clinic. The process of care is similar for the initial consultation and follow-up visits; however, some elements of care tend to be the focus of 1the initial consultation or 2follow-up visits, and total time tends to be longer for the initial visit. Care is team-based and interdisciplinary, with flexibility among tasks of the nurse and physician. ESAS-CS, Edmonton Symptom Assessment System including Constipation and Sleep; PRFS, Patient-Reported Functional Status.
Key tasks and domains of care for the initial consultation
Explaining palliative care, establishing a therapeutic relationship and exploring goals of care
Patients and families may be frightened by the word ‘palliative’, associating it with end-of-life care, and may question its relevance in their situation.28 It is important to state explicitly that the palliative care team works collaboratively with the patient’s oncology team and family physician, to provide integrated, collaborative, interprofessional care at all stages of the illness. It is explained that the palliative care team can help with symptom control, support for the patient and family, decision-making and planning for the future. Involvement at an early stage allows for the proactive prevention of problems and enables the development of a supportive therapeutic relationship.
The emphasis during the initial consultation is on support and enquiry, rather than direction. The aim is to establish a trusting clinician–patient relationship, which can be achieved only after understanding the patient’s background, values and goals. For most patients with advanced cancer, these goals include a desire to prolong life while optimising quality of life; many patients still hope for a cure of their disease.31 It is, therefore, important to explore understanding and expectations, and to explain that a focus on quality of life and symptom control is complementary to the goal of treating the cancer.32
Assessment of symptoms and psychosocial, spiritual and practical concerns
The patient’s cancer history, comorbidities, previous treatments, complications and treatment toxicities are reviewed thoroughly. Although symptoms may not be prominent early in the disease course, they should be assessed systematically. We use a modified version of the Edmonton Symptom Assessment System, the ESAS-CS, which assesses the severity of constipation and sleep, as well as pain, dyspnoea, nausea, depression, anxiety, well-being, fatigue, drowsiness and appetite, over the past 24 hours.33 In addition to rating each symptom from 0 to 10, patients are asked to identify three priorities for the visit34 and to rate their performance status.35 Each symptom rated as 4 or higher, or identified by the patient as problematic, is assessed in detail using validated symptom management guidelines.24 25 Medications (including complementary therapies and supplements) are assessed and deprescribed or continued, as appropriate.
For psychological symptoms, such as depression and anxiety, an ESAS level as low as 2/10 may be clinically significant, and patients may be reluctant to initiate a dialogue about emotional issues.36 Therefore, a psychosocial assessment should be conducted for every patient. This should include assessing coping of both patients and family members (eg, caregivers, partners and children), and should address existential, spiritual and social concerns.
Practical support is addressed by the palliative care nurse and may include the need for assistive devices, a home safety assessment or a hospice volunteer to help with groceries or other daily needs. Although these services may not be required, patients and caregivers appreciate knowing what is available to them. Caregivers are considered part of the unit of care, and their needs and concerns are acknowledged and attended to.37
Review, referrals and follow-up plan
The palliative care physician and nurse review the plan of care with the patient and family, establish a plan of follow-up (4-6 weeks routine and 2 weeks for complex symptom concerns) and explain the availability of the palliative care team during and after office hours (see section ‘Telephone follow-up’). Where relevant, other interdisciplinary team members are consulted to provide additional input (eg, social worker, spiritual care worker, occupational therapist, physiotherapist, dietician, wound care specialist, pharmacist, psychiatrist, etc), either immediately during the consultation or on a scheduled basis at a future appointment.
Documentation is completed immediately after the consultation, with copies sent to the referring physician, family physician and any other relevant members of the clinical team. Important information is relayed to the referring physician by direct contact.
Follow-up after the initial consultation
Ongoing follow-up is essential for the prompt management of symptoms and other problems; to avoid unnecessary visits to the clinic or the emergency department, follow-up occurs by telephone as well as in person. The overall process of care for follow-up visits is similar to the initial consultation (figure 4), although there are some differences in the content of care. The tasks of follow-up visits and telephone calls are outlined in table 2, with reference to principles and domains of care shown in figure 2. The main domains earlier in the trajectory of care tend to be symptom control (as symptoms become more prominent) and decision-making; future planning is gradually introduced as the therapeutic relationship develops. Sufficient time is scheduled for appointments so that complex symptoms and planning may be addressed. In general, follow-up appointments last 30–45 min.
Key tasks and domains of care for follow-up visits and telephone conversations
Telephone follow-up
Telephone contact is often necessary between appointments. Contact may be initiated by the patient, a family member or the palliative care team. Palliative care nurses are generally the first point of contact during working hours, while physicians participate in an after-hours on-call schedule. Patients are encouraged to call if they have uncontrolled symptoms, side effects or other problems. These are largely managed with telephone advice, preventing unnecessary visits to the emergency department; patients may also be admitted directly to the acute palliative care unit if necessary.38 Patients are given clear written information at the initial appointment regarding contact information during the workday and after-hours.
Follow-up in clinic: symptom control, decision-making and consolidating the therapeutic relationship
The ESAS-CS is completed at each clinic visit to evaluate treatment response and to assess new symptoms. Specific enquiry is made about side effects of the medications prescribed at previous appointments. Each symptom is treated according to symptom management guidelines, as during the initial consultation.24 25
Prior to each return visit, the palliative care physician reviews the patient’s chart to identify changes in the disease course or treatment plan. This information is discussed with the patient to clarify illness understanding, identify any new side effects of disease-directed treatment and address supportive care needs. Patients and caregivers may seek guidance in decision-making regarding cancer treatment, taking complementary therapies or participation in clinical trials. The role of the palliative care team is to act as a ‘sounding board’15: listening to the concerns of the patient; helping them to articulate their goals of care; taking into consideration beliefs and preferences; and discussing whether the treatment they are currently receiving or considering is consistent with these goals.
Maintaining a supportive therapeutic atmosphere and building on the rapport established at previous visits are crucial. Continuity of care is prioritised, with the patient meeting the same nurse and physician at return clinic appointments, whenever possible. This has been shown to be highly valued by patients, with lack of continuity cited as a common barrier to communication and rapport building in oncology follow-up.39
Follow-up in clinic: coping, community supports and advance care planning
The needs of patients with advanced cancer may change quickly. The progression of illness may result in difficulty coping and existential distress for both the patient and their caregivers; coping should be assessed at every visit, with provision of supportive counselling by palliative care nurses and physicians; referral to spiritual care, psychology or psychiatry, is offered as appropriate.24 Central in the counselling process is the fostering of a “double awareness” that death may be imminent but that life can nonetheless be meaningful.40 Enquiry regarding the need for home-based supports should also take place at each appointment, with appropriate referral to community services.
Advance care planning is introduced in a straightforward manner when the patient and family have developed a close therapeutic relationship with the palliative care team. Patients generally understand the importance of assigning a power-of-attorney for medical care, and making a will; online resources are available for the latter two tasks, avoiding costly legal fees.41 42 Discussions regarding preferences for end-of-life care and resuscitation status generally occur over time. Patients are encouraged to bring family members to appointments to take part in these discussions, which also require input from the oncology team and the primary care provider.43 Once a decision has been made not to have cardiopulmonary resuscitation, or another directive has been completed, this is documented clearly so that it is readily accessible to all care providers. Patients are provided with a paper copy of their do-not-resuscitate directive to prevent ambiguity outside the hospital setting.
Discussions about the preferred place of death may provoke anxiety, especially if opinions differ among patients and family members. A home death requires caregivers who are willing and able to provide care at home, and a support system that enables caregivers.44 Often the best approach is to acknowledge that a home death will be ‘Plan A’, but it is important to have a ‘Plan B’ of admission to a hospice or palliative care unit, in the event that a home death is not possible. Preferences around place of death may change over time and should be revisited at intervals.45
Team-based care: communication with other healthcare providers
Following a diagnosis of advanced cancer, there are often multiple physicians involved in the patient’s care, including the family physician, oncologist, palliative care physician and subspecialists treating comorbid illnesses.46 It is, therefore, imperative to establish who will assume responsibility for various aspects of supportive care, and to communicate clearly and openly with other treating clinicians as well as with the patient and family. Such communication is especially important during transitional points in the patient’s disease trajectory (such as the discontinuation of active treatment or following a discussion about end-of-life preferences). This ensures a consistent approach and allows the patient and family to understand who is responsible for each aspect of care.
Transition of care: involvement of home-based palliative care or hospice services
Involvement of home-based services is initiated while patients are still attending the palliative care clinic. Ultimately, home becomes the sole setting of care (unless there is transfer to an inpatient setting) and a transfer of care is required from outpatient care to home-based care. This often coincides with the discontinuation of disease-directed treatment, when routine oncology follow-ups cease. An ECOG performance status of ≥3 (ie, spending more than half of the day in a chair or bed) or Palliative Performance Status of ≤5047 is generally a reasonable point for the transfer of care from hospital-based to community-based palliative care services. Sometimes it is appropriate to initiate community-based care earlier, especially for patients who live far from the cancer centre or have difficulty travelling. Transfer of care should be seamless, with direct communication between palliative care clinic staff and the community-based service.
Conclusions
We have described the essential principles and domains of care, as well as key tasks, of an early team-based outpatient palliative care intervention for patients with advanced cancer. This model ensures that palliative care is accessible early in the course of disease, provided longitudinally in collaboration with other treating healthcare teams, and based on the needs of the patient and family, rather than on prognosis. This proactive approach to care is consistent with the contemporary definition of palliative care, which is to improve quality of life by prevention as well as relief of symptoms and other problems.19
This intervention was developed at a comprehensive cancer centre, and its structures and personnel may not be available in other settings. However, the essential elements of TO-EPC are consistent with those described in qualitative substudies of other early palliative care trials,13 14 48 including analyses of chart notes,13 patient interviews14 and interviews with palliative care physicians participating in the intervention.48 These key elements—the principles, domains and tasks outlined in this paper—should be retained to maintain the intervention’s integrity, while the manner in which these tasks are achieved can be adapted to be suitable for local contexts. Thus, if components of the intervention are difficult to enact in a particular setting, they may be replaced with others that fulfil a similar function.17
Early palliative care is of increasing relevance for patients with advanced cancer and other diseases, for whom prolonging and improving quality of life are simultaneous goals. The description of our intervention may assist researchers wishing to replicate or build on it for use in other trials. In addition, this intervention may serve as a template for palliative care teams to develop outpatient services, provide education and standardise care. Lastly, oncologists and family physicians may find this information useful to inform their own practice when treating patients with advanced cancer and their families.
Acknowledgments
We are grateful to the specialised oncology palliative care nurses who have provided input into the care model and comments for this paper: Catherine Purcell, RN, Malka Berman, RN, and Christine Cameron, BScN, MN. Many thanks as well to Nadia Swami, BSc, and Ashley Pope, BSc, clinical trial coordinators, who have also provided input into the structure of the intervention and comments for the paper.
References
Footnotes
Contributors All the authors contributed to the conception or design of the work. CZ drafted the work, and all the authors revised it critically for important intellectual content. All the authors approved the final version, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This research was funded by the Canadian Cancer Society (grant #700862; CZ), the Canadian Institutes of Health Research (grant #152996; CZ) and the Ontario Ministry of Health and Long-Term Care. CZ is supported by the Rose Family Chair in Supportive Care, Faculty of Medicine, University of Toronto.
Disclaimer The sponsors had no role in the design; in the collection, analysis and interpretation of data informing the paper; in the writing of the report or in the decision to submit the paper for publication.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.