Article Text

Abstract
Objectives To consider the type and cost of clinical services delivered for patients with lymphoedema.
Design Clinical cohort.
Setting Independent hospices in the North East of England.
Participants All those attending lymphoedema services delivered by the independent hospice sector 2017/2018.
Results 13 914 lymphoedema appointments were recorded across four independent hospices. Twelve thousand nine hundred and sixty-five were attended, which equates to an approximate cost of £1.56 million. Those with lymphoedema were predominately aged over 65 (54.5%) years with females across all age groups being more predominant (3.3:1). Where the cause was recorded, 66% of activity related to lymphoedema was not secondary to cancer.
Conclusion Independent hospices are providing a specialist lymphoedema service, which is high in volume and largely invisible. This service is delivered at not insignificant cost. In contrast to previous work, in the North East of England, lymphoedema sufferers are more likely to be female and not have the condition in association with cancer. The availability of rigorous data collection will allow the independent hospices to understand better the delivery and associated costs of lymphoedema services.
- skin care
- lymphoedema
- hospice care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of study
Large clinical cohort study.
Data collection over a wide geographical area.
An ongoing commitment from the independent hospices to continue collecting information to inform service transformation.
Increased awareness of lymphoedema services, the volumes seen, the overall costs and the routes for referral.
Introduction
Lymphoedema is a long-term, chronic condition that causes swelling in the body’s tissues. It can affect any part of the body, but usually develops in the arms or legs and occurs when the lymphatic system fails to work properly. The lymphatic system is a network of channels and glands throughout the body that helps fight infection and remove fluid. Lymphoedema can be caused by faulty genes that affect the development of the lymphatic system (primary) or by damage to the lymphatic system or problems with the movement and drainage of fluid in the lymphatic system; it can be the result of an infection, injury, cancer treatment, inflammation of the limb or a lack of limb movement.1–4
Lymphoedema is thought to affect more than 200 000 people in the UK. Primary lymphoedema is rare (affecting around 1 in every 6000 people) while secondary lymphoedema is more common affecting around 2 in 10 women with breast cancer, 50% of women with vulval cancer and a third of men with penile cancer.5 Treatment for melanoma in the lymph nodes in the groin can also lead to lymphoedema with the suggestion that approximately 20%–50% of people are affected. Because of this association with cancer and its treatment, hospices frequently provide a service for lymphoedema be it by design or one that has evolved over time.1 Studies are conflicting with some suggesting that the breakdown of cancer versus non-cancer lymphoedema is 50:50, while others suggest only 25% of lymphoedema cases were due to cancer.6
The variation in data is partly explained by different definitions that are used and different criteria that services may have for referral. Currently, the term ‘Lymphoedema’ is used for all chronic oedemas that may include true ‘primary’ lymphoedemas, those secondary to cancer and its treatment and also those secondary to other causes of oedema in which a previously abnormal lymphatic circulation is overloaded by increased capillary filtration and a secondary lymphatic failure develops.7
Guidelines recommend that if lymphoedema is suspected referral to a specialist, multidisciplinary, lymphoedema treatment centre for further assessment is advisable. Such services are rare. There is no cure for lymphoedema, but it is usually possible to control symptoms using techniques to minimise fluid build-up and stimulate the flow of fluid through the lymphatic system. These include wearing compression garments, good skin care, exercise, diet and lifestyle, and specialised massage techniques. Where lymphoedema services are provided, patients experience an improved quality of life,4 with it recognised that successful care requires a long-term collaborative approach between patient and providers.
Patients with lymphoedema have a significant risk of developing cellulitis and of incurring hospitalisation for the management of cellulitis. In a study of 228 patients with lymphoedema,6 65 patients (29%) had at least one episode of cellulitis and 16 of those required hospital admission with a mean length of stay of 12 days. A Kings Fund report confirms8 that cellulitis accounts for 7% of all emergency admissions in England and for 8% of the total costs for emergency admissions (£976 million of the total £12.2 billion). Specialist lymphoedema services help to reduce the occurrence of cellulitis and enable other cost-benefits such as improved compression garment prescription and reduced wastage and improved patient self-management, resulting in reduced utilisation of General Practitioner (GP) services.9
It is estimated that England currently spends more than £178 million on admissions due to lymphoedema, with a rise in costs of £7 million from 2013 to 2014, equating to more than 22 904 additional admissions.10 It has been estimated that for every £1 spent on lymphoedema services, the National Health Service (NHS) saves £100 in reduced hospital admissions.3
Historically, in the North East (NE) of England, lymphoedema services have developed to a large extent within the independent hospice setting, although the numbers and type of patients seen in these services have to date been largely invisible. In this study, we reviewed the prevalence and aetiology of lymphoedema delivered by the independent hospices in the NE of England.
Methods
The nine independent hospices across the NE have formed a collaborative (HNE) and are working together to develop a common data set in order to enable a collective description of the type and volume of services which are provided by the hospices, and the patients and their families served. The analysis and interpretation of the information provided within the data set aim to enable the pattern of hospice service delivery and service users to be compared in detail across the region. The data presented here is part of the ongoing development of data capture in HNE.
Data collection: HNE local data set
A data entry form template was developed for each hospice service containing the agreed fields in the data set, and most fields contained a drop down list of relevant data items to select from in order to make data entry easier and to limit the entries to certain data items. The templates were developed iteratively based on an initial draft local data set. Where feasible, the standard data items recommended by the Palliative Care Clinical Dataset (PCCDS) guidance10 were used as the basis for the field; however, in some cases, a local list or adjustment to the standard list was required following discussion with the hospice representatives. Each hospice was asked to complete the templates and submit these for collation and analysis by the clinical and quality measurement unit (North East Quality Observatory Service). It was agreed that the initial submission of data (baseline extraction) would relate to the financial year 2017/2018 only.
Depending on the hospice service, individual patient level or aggregate counts of activity (or both) were collected as per the original National Council for Palliative Care (NCPC) data collection.11 No patient identifiable data was shared, instead, where individual (patient) level data was submitted, a unique patient ID code (created by the hospice) was used to enable all hospice activity across different services to be identified for each patient. From an analysis perspective, the data was pseudonymised, but the hospice could use the ID code to reidentify the patients in their local system, if further investigation was required. Data sharing agreements were in place with each hospice.
Data items in the local data set
There are three different groups of data items in the HNE local data set:
Client data: information about the patient such as age on admission, gender and ethnicity. Demographic information is valuable to understand service user profiles; however, only the minimum amount of data was collected.
Spell/service data: information that is not expected to change during a spell of care in a single setting, such as referral date, reason and source of referral, registered GP practice, diagnosis and discharge method and destination.
Phase data: details that are assessed and recorded at initial assessment and then repeated each time the phase of illness changes. These include phase data collection date and phase change date, phase of illness, patient status (functional, pain, breathlessness, at peace, anxiety/distress and information needs) and carer support. There are multiple phases within a spell of care. Further details and definitions relating to the recording of this are available in the Guidance and Definitions document relating to the PCCDS.12
Data analysis and interpretation
The data analysis reported relates to activity reported by hospices for the financial year 2017/2018 only. The data is presented at either patient level or activity level, depending on which was most appropriate for each reported field.
Data submission details
Four hospices within Hospices North East (HNE) submitted data relating to lymphoedema outpatients.
There is variation between hospices in terms of the completeness of the data reported, with some hospices submitting only activity where the patient attended and other hospices submitting activity including where the patient did not attend. The analysis of data in this report is based only on activity where the patient attended and where this is recorded in the lymphoedema outpatients data collection within the ‘attendance status’ field.
Costs for lymphoedema services
The costs for delivery of lymphoedema services were calculated using the British Lymphoedema Society national 2018/2019 tariff,13 which estimates a new and review appointment for lymphoedema to have comparable costs of approximately £120. We believe that this is a conservative assessment of costs, as we did not consider the much higher costs associated with home visits or complex assessments (£329) or medical assessments (£234).
Results
There were 13 914 lymphoedema appointments recorded within 2017/2018 across the four hospices, of which 12 965 were attended at a tariff cost of approximately £120 per appointment. This equates to a conservative estimate of total costs of £1.56 million. The real costs of delivering the service were provided by three hospices and totalled £2 322 353.
Client identifiers were only submitted by three of the hospices and one of these reported only one attendance per patient. At patient level, the number of appointments per patient (where data was available) ranged from 1 to 109. Due to the variations in how this data has been submitted, at this stage it is not possible to accurately report the average number or median number of appointments per patient. However, table 1 suggests that at the largest hospice in our region, the average number of attendances per patient is approximately five equating to a minimum of £600 per patient.
Lymphoedema activity by hospice
Demographics
The age profile (based on age at attendance) of those accessing lymphoedema services (based on all attendances) shows that over 36% of activity relates to those aged 45–64 years and 54.5% relates to those aged 65 years and over (figure 1). It is possible for patients to be counted in more than one age group; however, it is not possible to determine the extent of this in this specific data set due to the absence of a patient identifier in records from one hospice.
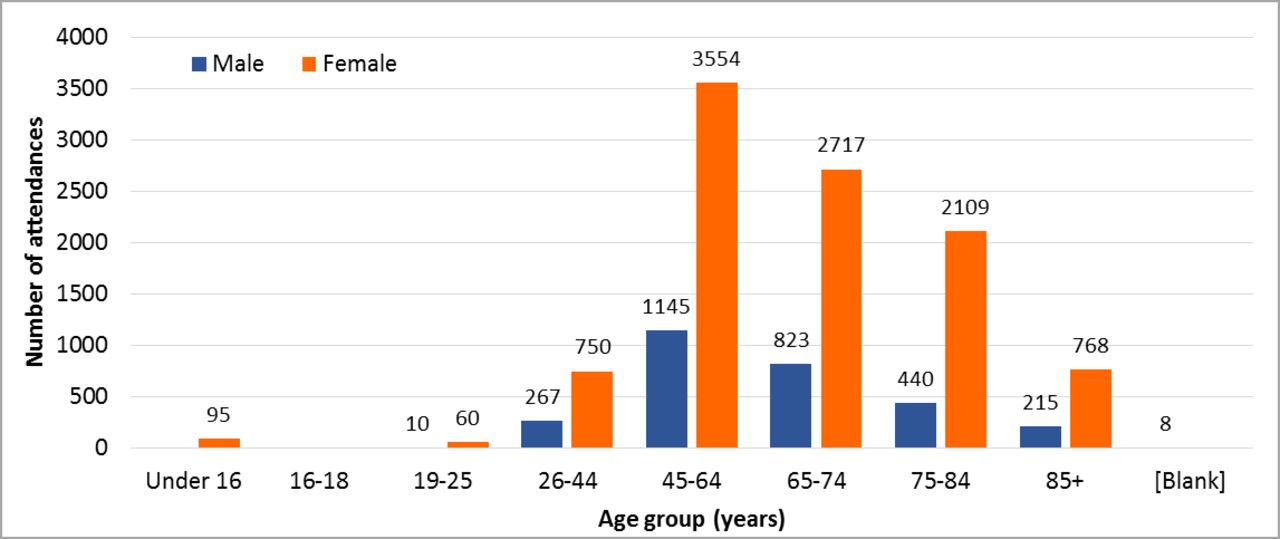
Lymphoedema outpatient activity by age and gender.
In contrast to what is described in the Best Practise Guidelines,1 the age at attendance and gender of service users across the four hospices based on all lymphoedema outpatient activity (figure 1) indicate that for all age groups the proportion of activity for female patients is higher than males. Further analysis of the data demonstrates that multiple appointments per patient have been recorded for both genders; however, the ratio of activity for females to males (at patient level) is approximately 3.3:1 (based on patient-level data available from three hospices).
The age profile of those accessing lymphoedema outpatient services is very similar for all four hospices (figure 2). St Oswald’s has a small proportion of activity for those aged 18 years and under.

Lymphoedema outpatient activity by age and hospice.
Ethnicity profile
Almost 55% of lymphoedema activity related to patients whose ethnic category was white. In over 41% of records, no ethnic group was recorded (table 2).
Ethnic profile of lymphoedema activity
Geographical profile
The registered GP practice of each patient was recorded in the data set, and this was mapped to clinical commissioning group (CCG) in order to understand the geographical profile of the activity (table 3). As there is substantial variation in CCG population size across the NE area, the activity rate per 1000 CCG population was included based on weighted CCG populations.
Lymphoedema outpatient activity by CCG
Newcastle Gateshead CCG and North Tyneside CCG have the highest rates of lymphoedema outpatient attendances (due to St Oswald’s). From a data quality perspective, 25% of the activity did not contain a GP practice code. The GP practice code was not known for activity reported by Teesside hospice.
Lymphoedema service data
The source of referral was recorded in the data set, based on a locally generated (non-standard) list of options, and this is therefore open to interpretation. As only one source of referral is reported per patient, irrespective of the number of lymphoedema appointments booked, a summary of the sources of referral is reported at patient level (n=2174) where feasible, that is, for three of the hospices (no data available for Teesside), and shown in figure 3A. The most common source of referral to lymphoedema services is the GP.

(A) Lymphoedema appointment source of referral; (B) Hospice level.
The findings at hospice level for the remaining three hospices are shown in figure 3B and indicate that the proportion of referrals from a GP varies from 96% to just under 57%.
Reason for referral
The standard list of data items to define reason for referral (detailed in the PCCDS guidance10 was recommended for use for this local data set; however, hospices have also included a number of other reasons for referral relevant to the patient). Although there is only one reason for referral given for multiple attendances for each patient, as the patient identifier is not present for data from one hospice, activity relating to reason for referral has been reported here based on all activity (table 4). The main reason for referral reported in the data set was for lymphoedema, followed by pain and symptom control.
Lymphoedema appointments by reason for referral
As these are palliative care services, some of the patients seen by the lymphoedema service will have been referred into the hospices initially for other ‘palliative care’ reasons (eg, pain and symptom management or complementary therapies) and that during the assessment or delivery of care, problems with lymphoedema will have been identified, which were then managed by the lymphoedema service. Hence, the reason for referral may be recorded as something other than ‘Lymphoedema’.
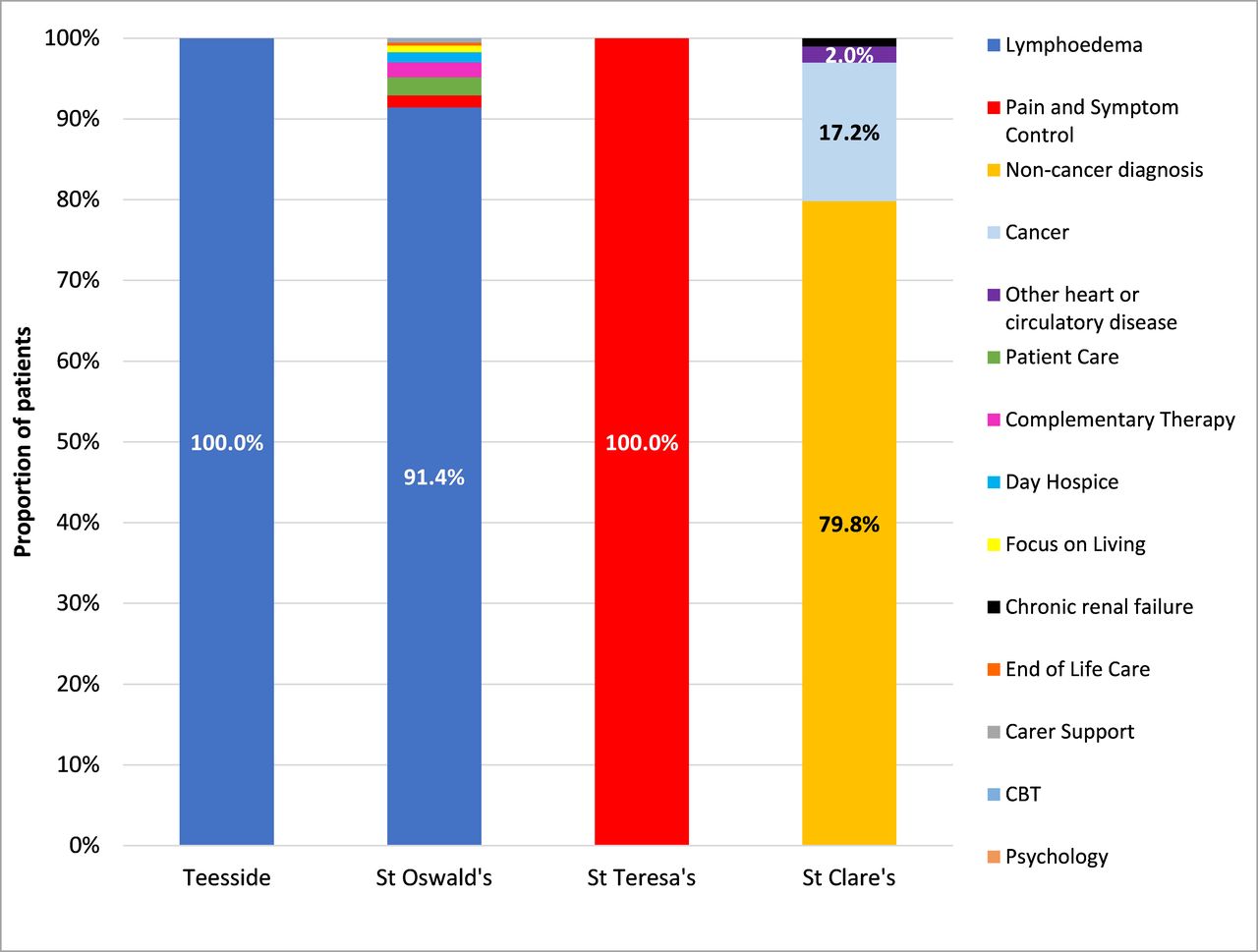
The findings at hospice level are shown in figure 4 and demonstrate that there is substantial variation between the hospices with regard to this field, which may be in part due to differences in how the data is recorded locally.

Lymphoedema appointments by reason for referral (hospice level).
Care type
This was a locally developed field used to describe the type of appointments offered within the lymphoedema service. A number of care type options were offered within the original service template, and hospices had the opportunity to report additional appointment types where relevant. The table below (table 5) shows the number of appointments for each care type. It is possible that further grouping of these categories could take place in future.
Lymphoedema activity by care type and delivery type (*number is <6)
Care delivery type
This was recorded based on a local list with only two options. For two hospices, all activities were reported as being delivered on a one-to-one basis and in St Oswald’s hospice 7.9% of activity was delivered in patient groups.
Diagnosis
Hospices were advised to use the International Classification of Diseases version 10 (ICD-10) code chapter (A-BB) from the PCCDS guidance11 to record the diagnosis relating to each lymphoedema outpatient appointment; however, the submitted data also contained other information (including ICD-10 subchapter codes). As a result, for the initial analysis the hospice level data has been presented as cancer or non-cancer and by condition category, although in future this could be disaggregated further.
Almost 27% of lymphoedema service activity in 2017/2018 was in relation to cancer, with a further 53.1% of activity recorded as non-cancer. For 2601 records (20.1%), the diagnosis was unknown. The breakdown relating to all admissions by diagnosis is shown in table 6, and the variation in diagnosis group for lymphoedema activity is shown in figure 5 at hospice level.
Lymphoedema activity by diagnosis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lymphoedema appointments by diagnosis group (cancer/non-cancer).
Discussion
This study draws on data from a regional initiative in the NE of England. The independent hospices have come together to consider their activity and where there may be opportunities to work collaboratively. As part of this, hospices NE have considered the delivery of lymphoedema services by the independent hospice sector in our region. It is clear that there is some variability and a need for greater consistency in terms of recording of activity and the collaborative is looking to collect data using the lymphoedema national minimum data set, as part of a UK wide benchmarking of lymphoedema services.14 15
This collective review has confirmed that less than half of those seen in the services provided by the independent hospice sector have a cancer diagnosis to account for their lymphoedema. This is in keeping with reports from some reports but different from others.16 In the first instance, this seems surprising considering the services are based in a hospice setting. However, it reflects the skill set of the teams delivering the service and how services have evolved over time. There are excellent resources available to underpin management of cancer-related lymphoedema, and more evidence for the benefits of generic approaches is needed in a non-cancer setting.17 18 The variability across different CCG areas, however, suggests that awareness of the service and ability to refer are inconsistent and accessibility variable. Also, in contrast with previous reports, those seen in the hospices NE collaborative are predominantly female at all ages.
It is clear that independent hospices are providing a specialist lymphoedema service for the NE, which is likely to be improving the quality of life of those seen and reducing admissions.1 This quality service however is associated with significant cost, at a conservative estimate >£1.6 million, which is met only in part by commissioning. The real costs of the service equate to >£2.3 million, suggesting a shortfall in funding above the available tariff of at least £0.7 million costs, which are presumably being met from other funding sources. If the clinical and cost benefits of multidisciplinary lymphoedema services are to be realised, it is important that they are commissioned appropriately and that there are adequate levels of investment to ensure development of the services together with improving our understanding of this complex and increasingly prevalent condition.
This study has a number of limitations. There is variation between hospices in terms of the completeness of the data reported, with some hospices submitting only activity where the patient attended, and other hospices submitting activity including where the patient did not attend. The analysis of data in this report is based only on activity where the patient attended and where this is recorded in the lymphoedema outpatients data collection within the ‘attendance status’ field. It is important that a consistent data capture system is implemented across the independent hospice sector in the NE and elsewhere if we are to ensure that the volume of patients with lymphoedema is recognised and good practise identified and disseminated. Currently, many of the services for lymphoedema patients particularly those delivered outwith the NHS are arguably invisible.
It is clear that the service offered to lymphoedema patients in the NE is valued by them and clinicians who refer to the services. However, for it to be sustainable, it is important that its long-term funding is secured by the NHS and not dependent on the unpredictable funding regimes seen in the hospice sector.
Footnotes
Contributors CN conceived the project, developed the dataset and oversaw data collection. AB and AF refined the data set, analysed the data and produced the first draft of the report. JN conceived the project, developed the dataset, analysed the data and drafted the paper. SG, AH, AE and JE oversaw the project and interpreted the data. All authors reviewed and approved the manuscript.
Funding The data collection was supported by a grant from the James Knott Trust and from the Academic Health Science Network NENC.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.