Article Text

Abstract
Objective To identify the position of formal service providers in the networks of those providing end-of-life care in the home from the perspective of the informal network.
Methods Using third-generation social network analysis, this study examined the nature and strength of relationships of informal caring networks with formal service providers through individual carer interviews, focus groups of caring networks and outer network interviews.
Results Service providers were usually highly valued for providing services, equipment, pain management and personalised care for the dying person plus support and advice to the principal carer about both caring tasks and negotiating the health system. However, formal service providers were positioned as marginal in the caring network. Analysis of the relative density of relationships within networks showed that whereas relationships among family and friends had similar density, relationships between service providers and family or friends were significantly lower.
Conclusion The results supported the Circles of Care model and mirror the perspective of formal service providers identified in previous research. The research raises questions about how formal and informal networks might be better integrated to increase their effectiveness for supporting in-home care.
- terminal care
- methodological research
- home care
- social care
- supportive care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
There has been growing interest in health promotion approaches to end-of-life (EOL) care1 proposed by Kellehear,2 3 which are defined as any set of initiatives that develop the social resources of the community to enhance quality of life at EOL. However, it is not necessarily easy to demonstrate changes due to community development, but social network analysis (SNA) has proved to be a valuable technique to illustrate the nature and growth of community caring.4 5 The advantages of SNA are that it reveals the specific people in the community who are providing the care and illustrates their relationships to the principal carer and the dying person. Thus, ‘community’ ceases to be a vague, catch-all phrase and comes to life in the actions and relationships of real people.
SNA appears to be most useful when it is coupled with qualitative methods that provide detailed descriptions of the nature of the caring work and relationships that contribute to the EOL caring. This nexus of qualitative research and SNA has been referred to as ‘third-generation SNA’.6 Previous research using the third-generation approach to analysing EOL care in the home found an increase in the size of caring networks and a strengthening of relationships among the original members of the network over time. The qualitative data revealed the important differences between inner and outer network members and the diverse ways the network members provided support. More generally, the research supported the potential for EOL caring to build social capital.4
The present research was designed to extend earlier research by examining the different positions in caring networks of family, friends and neighbours, other community members and formal service providers. Based on our earlier work, Abel et al 7 conceptualised ‘circles of care’ whereby inner and then outer networks of the informal network are surrounded by the community, then the service providers, with the government and policy makers being the very outer ring. Thus, one aim of this analysis was to examine this understanding of community care with a particular focus on the role of formal service providers.
Formal service providers are clearly important because of their often essential role in maintaining the comfort of the dying person. A formal service is any service provided by an incorporated body such as a government department or a not-for-profit organisation for the care of the dying person and family by paid staff or volunteers. They range from medical services, home care services, counsellors, religious ministers to support groups if they are auspiced by an organisation. In practice, however, both volunteers and paid staff can provide additional help8 and sometimes it is unclear if such help is given as part of the formal service, as a fellow member of the community, or as a friend or even as surrogate family.9
Previous small-scale studies have shown some of the barriers to support in the home such as lack of hospital discharge coordination, equipment and out-of-hours services,10 some enablers such as ongoing dialogue between medical services and carers,11 and also trialled some effective interventions such as the provision of a network facilitator.12 Our previous research with formal providers found that they are aware and largely supportive of the vital role informal networks play in the care of the dying at home.13 However, a number of barriers to formal and informal networks working together more effectively were identified, such as the regulations around confidentiality. Overall, the research showed that the Australian policy of health-promoting palliative care is not substantially translating to practice. This previous research also found that formal network members, on the whole, believed that combinations of formal and informal caring networks were essential to support people at EOL and their primary carers, but they themselves do little to establish, support or maintain the informal networks even when there is goodwill and scope for them to do so. There was potential for a stronger and more proactive reorientation towards health-promoting palliative care and community capacity building approaches. The present research complements these findings by examining the role of service providers from the perspective of the informal caring network.
The present analysis describes in detail the caring networks of people with a terminal illness who are being cared for at home and addresses the relative positioning in the network of family and friends, community and service providers. Further, it identifies changes in these caring networks that occurred over the period of caring. In keeping with third-generation SNA,6 it is located within a social constructivist paradigm where the network is defined and described by the network members rather than by the researchers.
Research questions
How are service providers positioned by informal caring networks?
Is there support for the Circles of Care depiction of community caring at EOL?
What insights into caring networks can be obtained to inform carers and palliative care service providers?
Method
Based on third-generation SNA, the research used both network mapping and qualitative data to understand the nature and role of the support networks. The SNA exercise followed a discussion of caring roles prompted by photographs taken by the participants so their memories of the caring network were primed visually and verbally.14 Details of the photo-elicitation method have been reported elsewhere.15 16
Participants
As shown in table 1, the data consisted of 36 networks of people who had cared for someone who had died at home in the past 3 years. Information obtained from a focus group of network members or an interview with an individual carer supplemented with data from an outer network interviews (ie, people who assisted on the margins of the caring network but were not involved directly in caring). Carers were recruited through letters distributed by a cancer support organisation, a motor neuron disease organisation and through newspaper articles. The primary carers then identified the caring network invitees for the focus group. Potential outer network interviewees were identified from the interviews and focus groups, and carers were asked to pass on details of the study and participation invitations to them.
Participants and networks by method and location
Network mapping approach
The map making was designed to enable participants to provide the first level of analysis. The advantages of the mapping approach are that (1) the participants see the results and can give interpretive feedback which becomes qualitative data and (2) focus group participants are able to remind each other of relationships and time lines in situ.
First, the principal carer completed two name generation tables of all people in the caring network for Time 1: when caring began and Time 2: after caring. Copies of these lists were made for all participants (focus group members and outer network interviewees) for that network. Then:
Participants in focus groups and outer network interviews added more names (if needed) to the carer’s lists.
All participants indicated the nature their own relationship (eg, friend, pharmacist) and the strength of their own relationship (0 no relationship to three strong) to each person on the list.
Participants then translated this information into Time 1 and Time 2 network maps. The names on the list were written around the edge of a large piece of paper and all participants indicated with coloured pens (yellow/weak, blue/medium, red/strong) the strength of their connections with the people listed. The final part of the process was to ‘bring the map to life’ prompted by questions such as: What do you notice about the two maps? What does that mean to you? This discussion was recorded and transcribed.
Analysis
The first level of data analysis took place in the focus groups where participants were asked to give meaning to the network maps. This was in order to gain the stories of participants and to understand what was important to them, in terms of caring and the development of networks at this time. The second level of analysis was a qualitative analysis of the discussions and the quantitative analysis of the network mapping exercise. For the qualitative analysis, data were classified into core concepts and categories derived from the research questions using NVivo10, then themes were developed around these categories. The third level of analysis was the comparison of qualitative and quantitative data to show if, and how, the quantitative analysis illuminated further understandings of the caring networks.
For the quantitative analysis, information from the 17 outer network interviewees was joined to the original networks to which they belonged. The network maps were transcribed into an adjacency matrix. NetDraw V.2.117 within UCInet17 was used to turn the network adjacency matrices into computerised network maps with the thickness of the lines indicating the strength of the ties and shapes to distinguish the different types of network members (family, friends, community, service providers). Density is the number of ties divided by the number of possible ties. An increase in density indicates people are developing more connections and stronger relationships. In this study, the density takes into account the strength of the ties that ranged from 0 to 3; thus, density can range from 0 to 3. UCInet was used to measure the density for four types of relationships to the principal carer: family, friends, community and service providers. Paired t-tests were then conducted to see if there were differences in the average density across relationship types.
Results
Formal service providers
Of the 36 caring networks, there were only four focus groups and one carer who did not identify formal service providers as part of the caring network in either the transcripts or the network diagrams. However, eight carers talked about formal service providers in their interviews, mostly in glowing terms, but did not put them on their network maps. Generally, only one or two service providers were mentioned for each network (time 1 mean=1.6; time 2 mean=1.3) but two carers (C4 and C9) mentioned numerous medical staff and had 10 and 15 service providers listed. C4 was relatively new to the area and had few friends, so the formal service provision might have been more salient. C9 was the wife of a man with motor neuron disease who had formed many relationships with formal providers over the long course of his illness. Aside from C4 and C9, most service providers included in support networks were those who came to the home such as palliative care nurses (14), community nurses (12) and home carers (12). Another nine listed their general practitioner. Four carers listed eight hospital staff and four carers listed people who had provided them with personal advice such as the Life Circle mentor, counsellor, patient advocate and a cancer support organisation.
Value of formal service providers
The formal service providers helped the carers to attend to the needs of the dying person through providing services and equipment, help with pain management and personalised care for the dying person, for instance adjusting procedures so they could be completed at home. Through formal service providers, carers could bridge to services that they did not previously know existed. They helped the principal carers by training them in medical procedures, such as how to administer injections. There were numerous examples of service providers lining up a range of equipment and services, mainly for the dying person but sometimes for the principal carer as well.
They (palliative care team) gave us a hospital bed, a commode, a chair—one of these recliner chairs—a wheelchair. They organised for somebody to come in and put handrails in the shower and put a new thing into the shower so that I could shower him in a chair. Everything! They provided all of those things and they organised it. (Carer 13)
Carers particularly appreciated having access to telephone advice around the clock. Even if that service was rarely used, it was a great comfort to know there was somebody to ring in case of unexpected problems. Some service providers also provided emotional support to the carer. It was appreciated when they were honest about the dying person’s condition and sometimes it was easier for the service providers to talk to the dying person. It was a relief to carers when the formal service providers validated their work so they knew that they were adequately managing the practical side of caring. Overall, people felt very satisfied when service providers were attentive and respectful to their needs and connected them to useful support services.
Working the system
Relationships between the carers and the formal service providers were not always straightforward. Carers found they needed to understand the system and preferably have some inside contacts in order to get the help they needed. In particular, they felt that being known personally by the service providers greatly increased the quality and flexibility of services. People who had worked in caring services or had a relative in the health field, or simply had built up a network through years of caring all felt they had an advantage in lining up the services they needed.
(A psychologist in the family) organised this family doctor because he dealt with her professionally and he knew she was a good doctor … she teed up Palliative Care for us and Home Care. (Carer 20)
Sometimes the carers had to actively resist the control of the medical services and get the services they needed, and it helped if they had a health professional supporting them.
Don’t go home without an ACAT because it’ll be much harder to get it at home. … No matter how they bully you, just refuse to leave. (Carer 8)
Disruptions to relationships
The relationships between carers and formal service providers could be weakened or disrupted by poor or inappropriate services, or insensitivity of service providers; the mental health of the dying person could also make relationships challenging. There could be conflict between the personal approach of the informal network and the professional approach of the formal service providers:
Professionals are supposed to not get involved but we cared for the man and the nursing service is a business. So there was this real divide between us and them and it just got worse and worse. (Outer Network 16).
Even good relationships during the caring period usually ended abruptly when the person died and some carers reported feeling deserted or struggling with daily tasks because the services were only provided for the dying person.
Relationships with formal services providers as revealed in the network diagrams
In almost all cases, service providers were at the periphery of the maps indicating the weaker and fewer ties to service providers than to family, friends or community. This effect is reflected in the differences in density (table 2). There were no significant differences between the density of networks within family and those between family and friends, indicating that relationships among family and friends were equally strong in this sample, but of course differences might be significant with a larger sample. There were, however, differences between the density of ties within family versus ties from family to community with the latter being significantly weaker. The difference in density between ties within family and those between family and service providers was particularly marked.
Comparisons of density among family members with density of ties family to friends, community and service providers
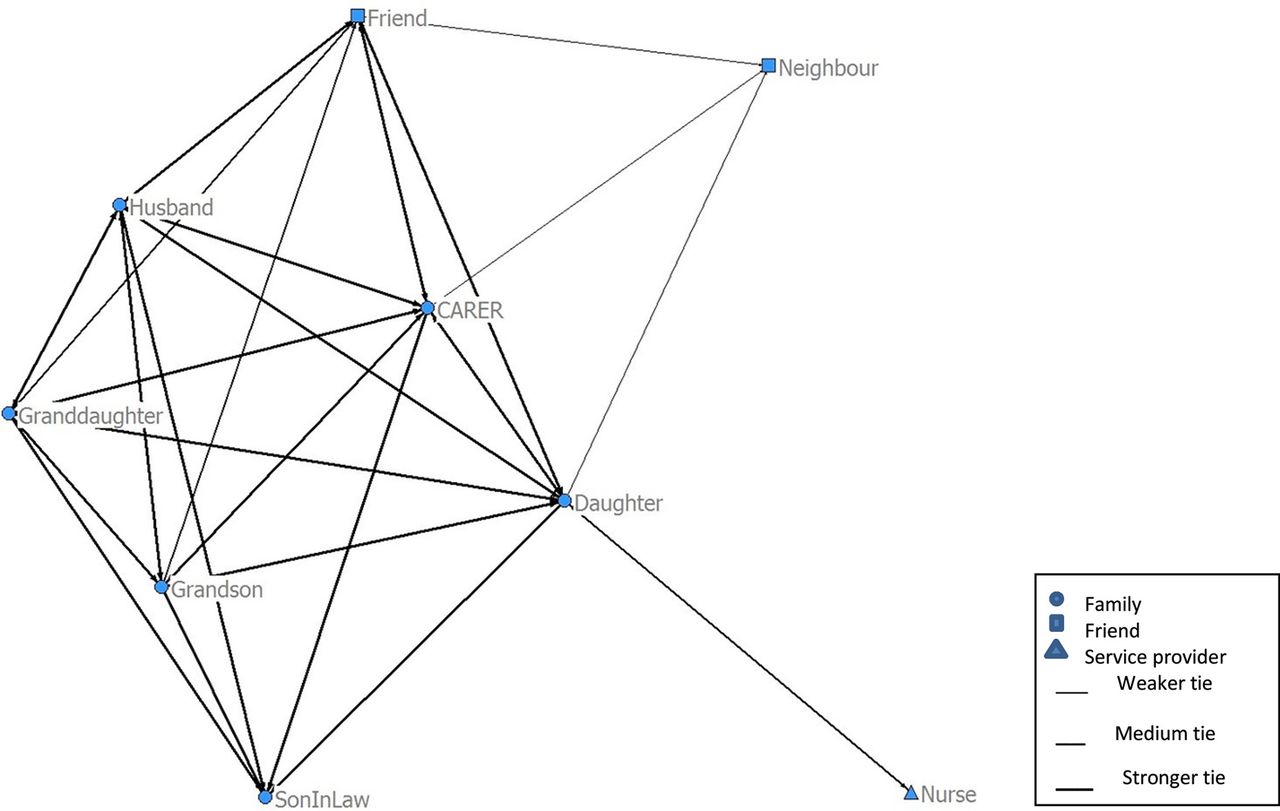
Focus Group 8 is a clear example of the separate worlds of the informal network and formal service providers (figure 1). When the community nurse was interviewed as an outer network member, she identified three formal service providers (a palliative care nurse and two doctors) as additional contacts. These contacts were known to the carer but were not identified as part of the network.

Focus Group 8 with outer network at time 2.
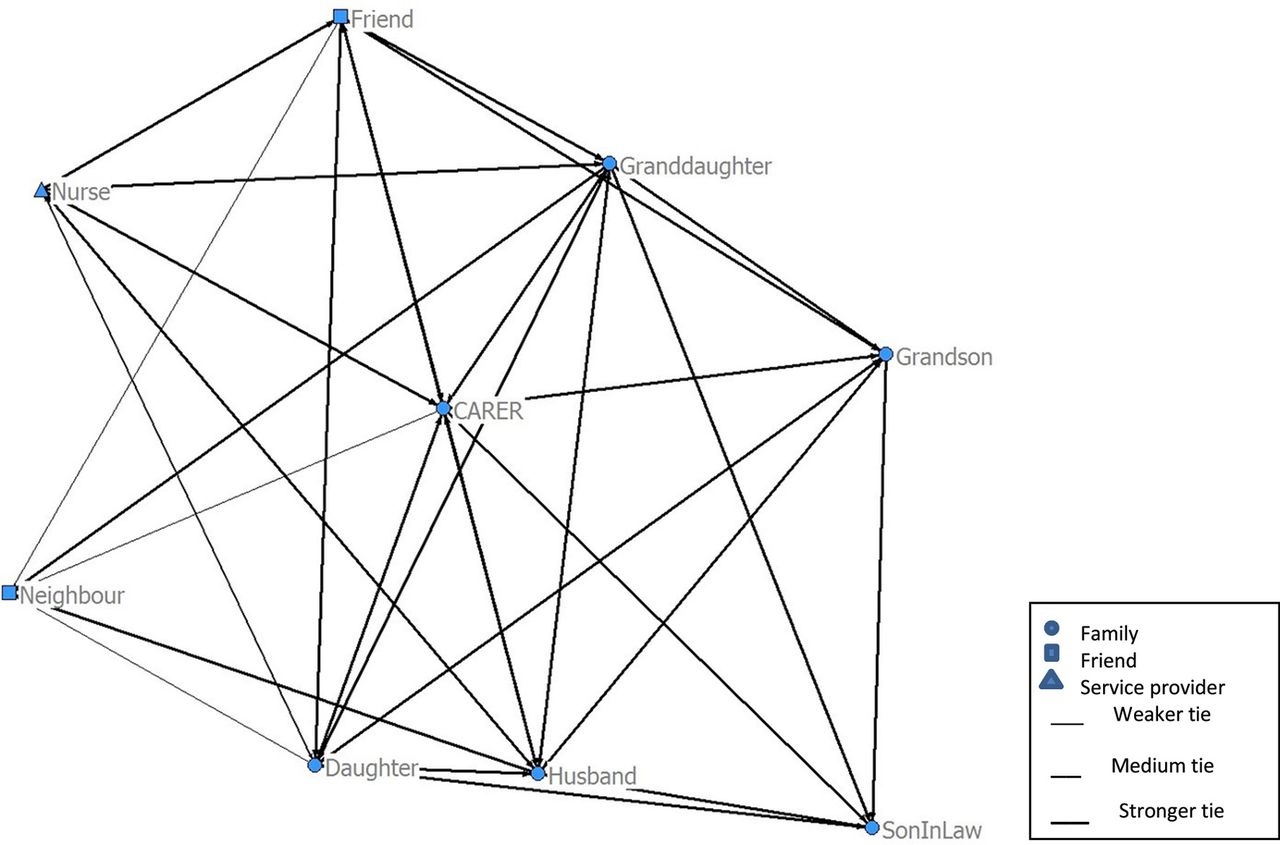
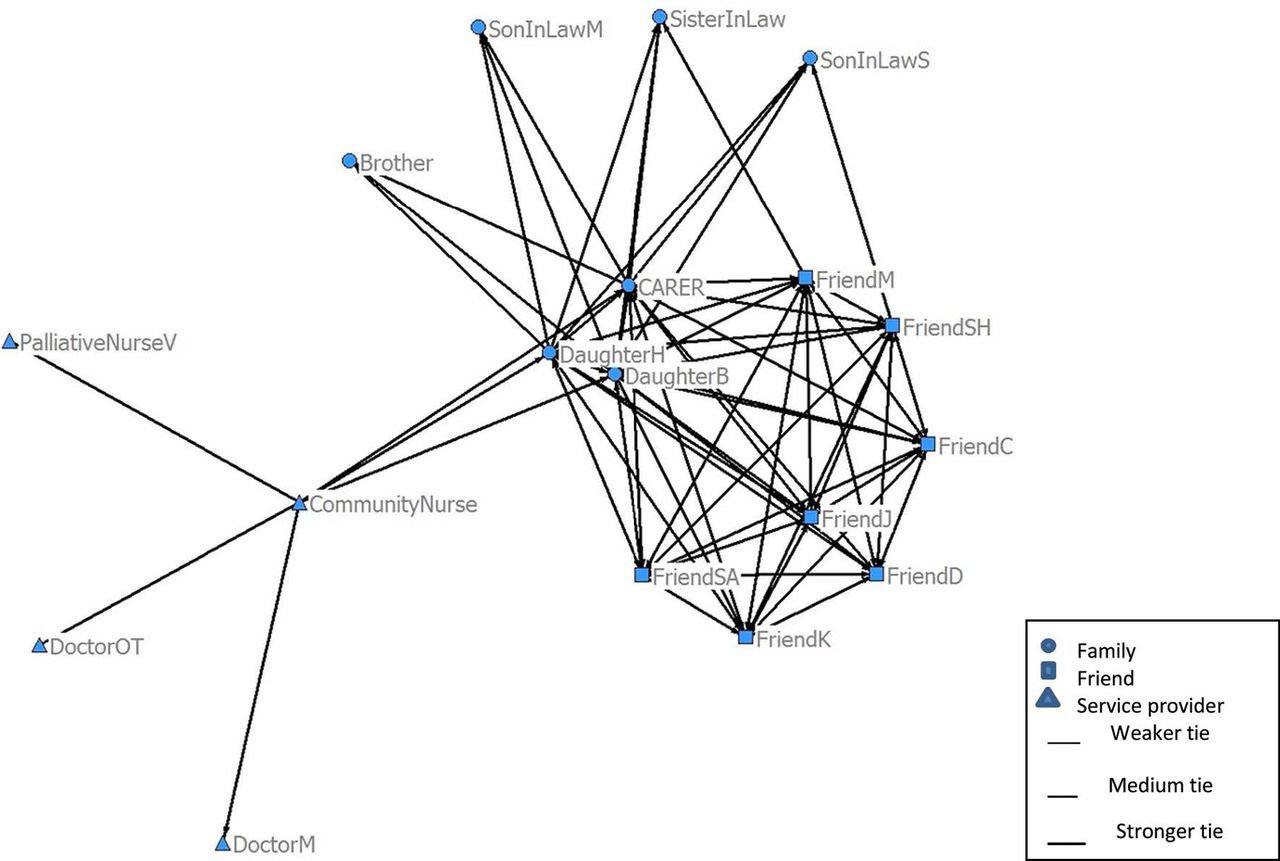
Out of the 36 networks studied, there were only eight examples where the strength or number of ties with service providers increased from time 1 to time 2. When ties strengthened, it was generally with the community and palliative care nurses (eg, Figures 2 and 3). In one case, a friend became a formal service provider, which seemed to have the effect of drawing other formal service providers more closely into the network. They also felt stronger ties to those service providers who supported and empowered them and helped them work the system.
Focus Group 5 time 1.
{kind=link}
{kind=link}
{kind=link}
Focus Group 5 time 2.
Discussion
We found support for the circles of care model7 in which the service providers are outside the community who are outside the outer network; however, the boundaries were more blurred than presented in the model. Especially in rural areas, service providers were also members of the local community, sharing the same schools, shops and other facilities. The community members included in this study were the ones who had become part of the outer network by the time of the research.
The relative marginalisation of the service providers in the caring network as perceived by the informal carers mirrored the perspective of the service providers themselves as revealed in our previous research.13 Although most formal service providers recognised the value of informal networks, they did not establish, support or maintain them; indeed, they had very little contact as usually their sole focus was the dying person and the principal carer. So it is perhaps not surprising that they were perceived as marginal by the caring network.
The evidence for the position of service providers came from both the SNA and from the qualitative analysis. In SNA graphs, people are presented as marginal if they have ties to relatively few other people and/or those ties are weak. In most cases, service provider relationships were restricted to the principal carer and the qualitative data revealed that they were focused on practical care and were sometimes quite tense. As a corollary, service providers would become more central if they have more contacts within the network or they can strengthen their relationships.
The qualitative data suggest that the distinction between ‘care as service provision’ and ‘care as relationship building’ was significant with the latter being necessary for the creation of social networks.18 Using the concepts of agency and communion,19 20 the respondents perceived that the ties with service providers were mainly about agency, that is, about getting things done. Hence, their main priorities were equipment, medical treatment, medical advice and training for the carer to help the dying person. Consistent with research showing the lack of pathways to bereavement care,21 participants reported that help was withdrawn immediately after the death. The relationship between EOL service providers and communities appears to keep the expert–recipient dyad predominant in Australia and elsewhere,13 22–24 and it is a challenge for health professionals to identify the support needs of carers without replacing the carers’ role.25 Further, the concept of care mainly as service provision holds within it the danger of alienation from the kinds of human interaction and collective processes that sustain individuals and communities confronting life’s final journey. In contrast, for the informal caring network, participants described relationships as the priority and the conducting of caring tasks was understood as part of those relationships.18
The relationships that support the carer and dying person can be understood as the mobilisation of social capital,18 26 and the development of social capital requires a mutually enhancing relationship between the agency and communion.20 This is not to suggest that formal service providers should be providing the very personal connections that an informal network can provide but rather that the two networks communicate and assist each other with formal services. Further relationships could also be strengthened by the provision of strong support and advocacy within the system, which empowers patients and carers. Thus, we would argue that for EOL care to create the social capital necessary for compassionate communities, agency and communion need to be integrated across caring networks that include both formal service providers and informal support, with each person learning from the others.
Third-generation SNA demonstrated the potential to identify the differing positions and roles of members of the caring network. We recognise, however, that three important limitations of the study are (1) the possibility of a social desirability effect, which would inflate tie strength in focus groups, although the procedure required participants to first indicate privately the strength of their ties; such procedures have been shown to decrease social desirability effects27; (2) the reliance on memory for the time 1 maps, which might exclude some weak ties; however, having the group discussion of the photographs beforehand did stimulate memories of that time; and (3) the network ties among people who were not present are underestimated.
Conclusion
The results of our analysis revealed the relatively marginal positioning of formal service providers as perceived by informal networks. Despite these perceptions, opportunities arose in EOL caring to build networks of support among family, friends, community and service providers. However, when palliative care practice focuses on actions for the physical comfort of the dying person and possibly their principal carers, and informal networks are preoccupied with relationships, there is a separation of agency and communion that is detrimental to the growth of social capital. The effective implementation of health-promoting palliative care (HPPC) policy would encourage a mutually enhancing relationship between agency and communion for anyone involved in EOL care. Although HPPC is prescribed throughout state and national palliative care policies in Australia, the findings of this study confirm previous work with service providers showing HPPC is not widely practised.13 However, we also found that formal service providers would like to engage with the HPPC approach. On this basis, we recommend interventions be designed and evaluated for building stronger networks between formal and informal networks to relieve stress on the principal carer and improve the experiences of the dying person.
References
Footnotes
Contributors RL: the first author has the expertise in SNA. She designed the SNA data collection conducted the analysis and led the write-up of the study. DH leads the research project and was involved in the design, data collection, qualitative analysis and writing up of the study. KN instigated the research and was involved in the design, data collection, qualitative analysis and writing up of the study. JR provided expertise on service providers and was involved in the data collection, qualitative analysis and writing up of this study.
Funding This project was funded by the Australian Research Council, the Cancer Council of NSW, the Western Sydney University and the CSIRO.
Competing interests None declared.
Ethics approval Approval for the project was obtained from the University of Western Sydney Human Research Ethics Committee (Approval No. H9255).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Because this is an in-depth relatively small-scale, largely qualitative study, the ethics approval does not allow data sharing.