Article Text

Abstract
Objectives Evaluations of new services for palliative care in non-cancer conditions are few. OPTCARE Neuro is a multicentre trial evaluating the effectiveness of short-term integrated palliative care (SIPC) for progressive long-term neurological conditions. Here, we present survey results describing the current levels of collaboration between neurology and palliative care services and exploring the views of professionals towards the new SIPC service.
Methods Neurology and palliative care teams from six UK trial sites (London, Nottingham, Liverpool, Cardiff, Brighton and Chertsey) were approached via email to complete an online survey. The survey was launched in July 2015 and consisted of multiple choice or open comment questions with responses collected using online forms.
Results 33 neurology and 26 palliative care professionals responded. Collaborations between the two specialties were reported as being ‘good/excellent’ by 36% of neurology and by 58% of palliative care professionals. However, nearly half (45%) of neurology compared with only 12% of palliative care professionals rated current levels as being ‘poor/none’. Both professional groups felt that the new SIPC service would influence future collaborations for the better. However, they identified a number of barriers for the new SIPC service such as resources and clinician awareness.
Conclusions Our results demonstrate the opportunity to increase collaboration between neurology and palliative care services for people with progressive neurological conditions, and the acceptability of SIPC as a model to support this.
Trial registration number ISRCTN18337380; Pre-results.
- chronic conditions
- communication
- clinical decisions
- neurological conditions
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Background
Palliative care has been proposed to help meet the needs of patients with progressive non-cancer conditions such as long-term neurological conditions (LTNCs).1 2 However, there is little or no evidence on the best ways of providing palliative care for these patients. Should it be at the ‘end of life’ or earlier such as at the point of diagnosis? Our own phase II randomised controlled trial (RCT) in patients with multiple sclerosis (MS) showed a reduction in symptoms and caregiving burden, following short-term integrated palliative care (SIPC) compared with standard care.3 More recently, a pilot RCT in Italy evaluating the impact of a new specialist palliative care service for patients with a range of LTNCs found significant improvements in quality of life and physical symptoms.4 Whether more people living with different LTNCs can benefit from SIPC and whether it can be routinely used in practice to improve care quality are of interest.
OPTCARE Neuro is a multicentre RCT evaluating the effectiveness of SIPC for progressive LTNCs (ISRCTN18337380). The SIPC service being trialled is defined as three palliative care visits over 6–8 weeks. This is a phase III RCT in patients with a range of LTNCs including: MS, motor neuron disease (MND), idiopathic Parkinson’s disease, progressive supranuclear palsy and multiple system atrophy. The overall aim of OPTCARE Neuro is to evaluate the clinical and cost-effectiveness of SIPC to optimise care for people with LTNCs. In addition to understanding the effectiveness of this service, it is also important to understand and be aware of current service provisions and the views of professionals involved in providing care for this patient group. The complexity of delivering and evaluating palliative care services requires the accumulation of knowledge from multiple sources and will depend on interprofessional behaviours.5 6 It is therefore valuable to explore clinicians’ views and opinions when shaping emerging services and informing future requirements. With that in mind, we conducted a short online survey with neurology and palliative care professionals. The main aims of the survey were to:
understand what current levels of collaboration exist between the two specialties;
explore the expectations and views of clinicians towards the SIPC service being trialled.
Methods
Research teams at six UK trial centres (London, Nottingham, Liverpool, Cardiff, Brighton and Chertsey) identified local neurology and palliative care professionals who were then approached via email by the central trial team. Professionals were informed that by completing the survey, they provided informed consent for use of their anonymised data. The surveys consisted of multiple choice or open comment questions, 13 (for neurology) or 10 (for palliative care) with responses collected using online forms. The survey was launched in July 2015 and closed April 2016. The study was approved by the National Research Ethics Service Committee London South East (REC number: 14/LO/1765).
Results
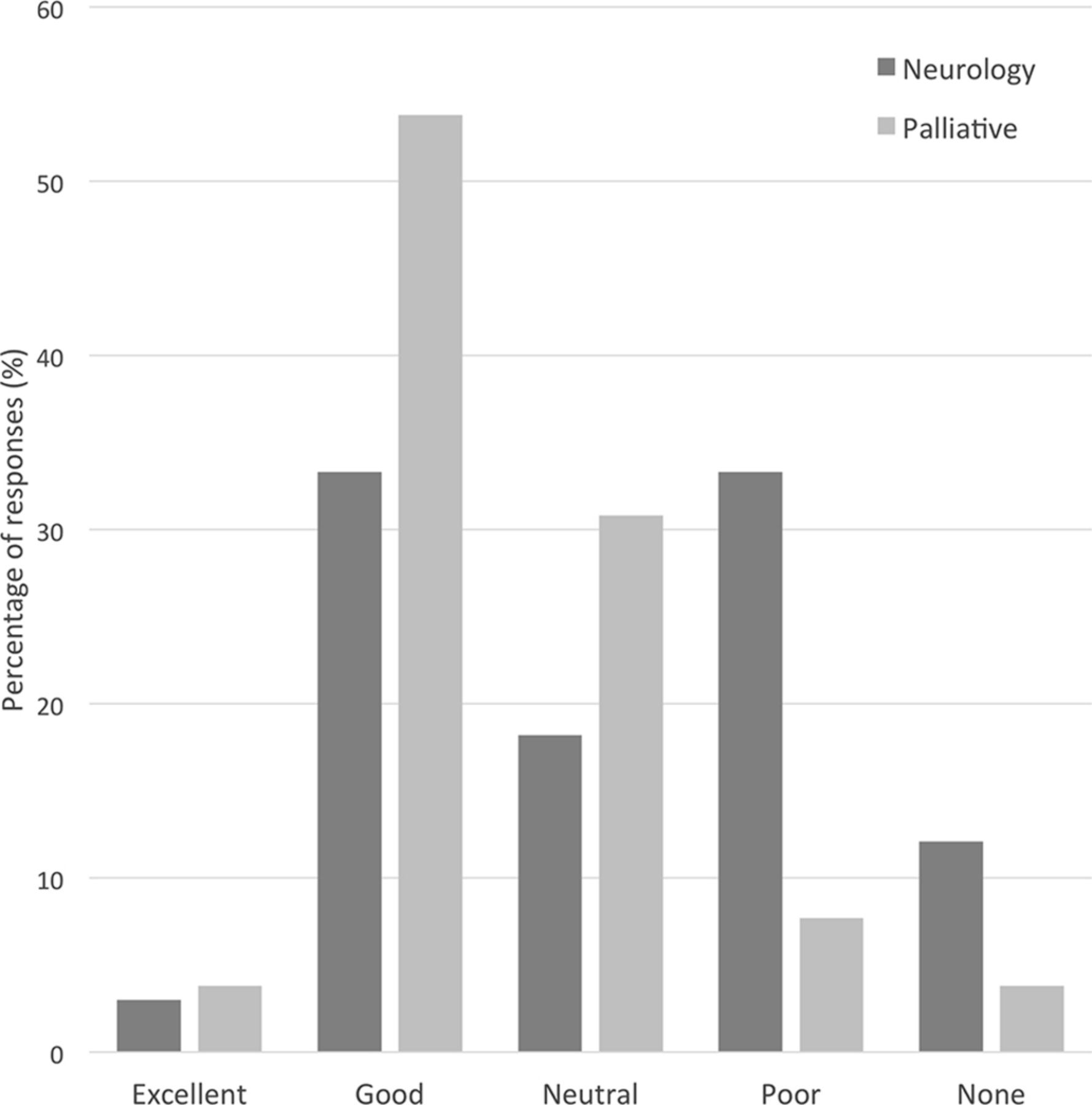
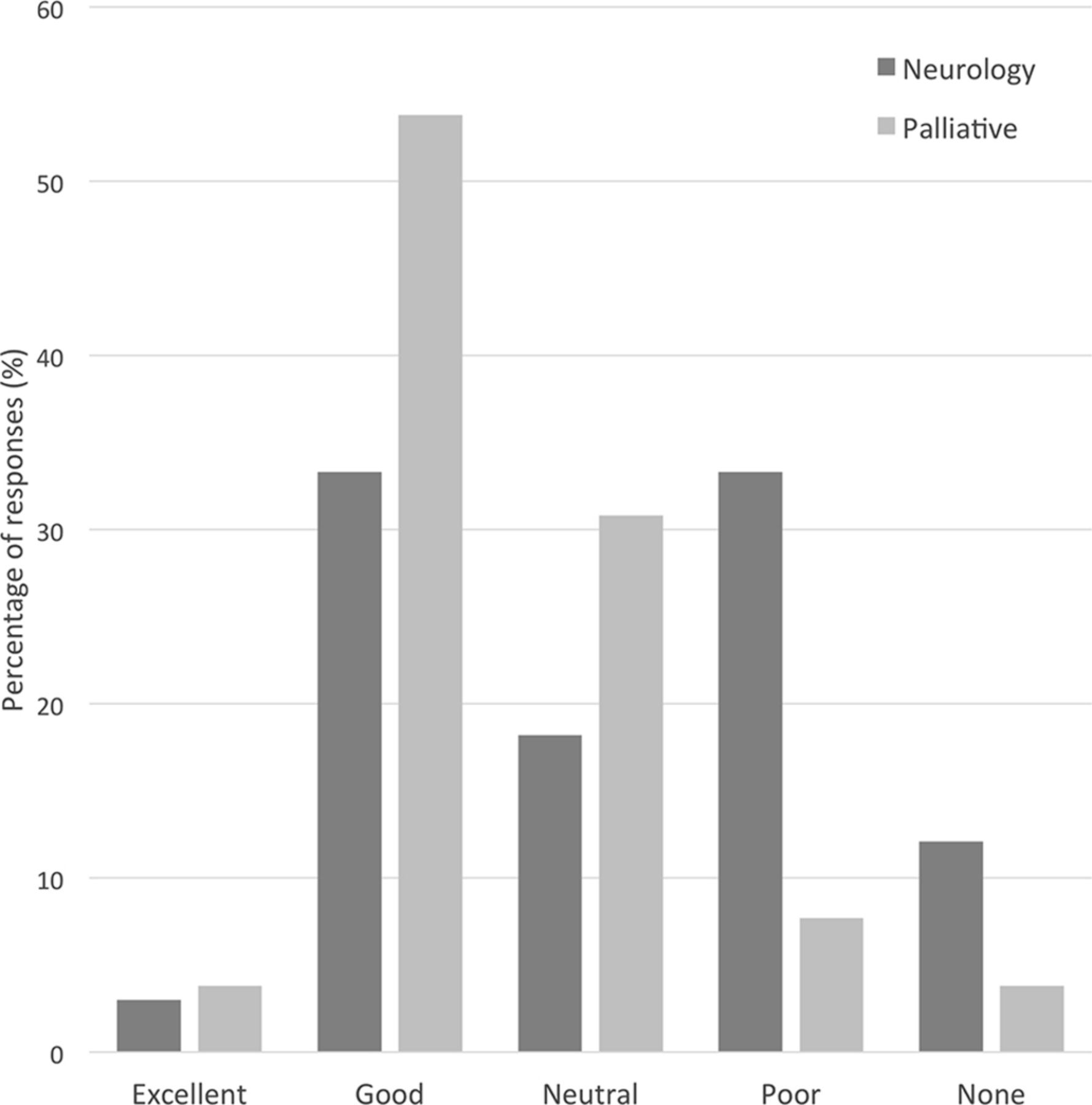
The survey received responses from 33 neurology and 26 palliative care professionals (20% response rate). Two-thirds of respondents in both groups had over 10 years of experience in their respective fields. Current levels of collaboration between the two specialties were reported as being ‘good/excellent’ by 36% of neurology professionals and by 58% of palliative care professionals. However, nearly half (45%) of neurology compared with only 12% of palliative care professionals rated current levels as being ‘poor/none’ (see figure 1). When asked if there were any particular disease areas where links were better, both groups reported stronger links for MND. In addition, both professional groups felt that the new SIPC service being trialled would influence future collaborations for the better (65%–70% in both groups).
{kind=link}
Neurology and palliative care professionals’ ratings of their current levels of collaboration with the other specialty.
Participants were also asked what they thought would be the main barriers for the new SIPC service (see table 1). The most commonly identified barriers by neurologists were resources, clinician awareness of services offered, continuing collaborations and communication between teams beyond the trial and geographical limitations. Similarly, palliative care professionals also identified resources and clinician awareness (and, importantly, the appropriateness of referrals they may receive) as barriers. However, the key barrier they identified was that there may be a possible need for longer-term care beyond that offered by the SIPC service. They also drew attention to patient perceptions of palliative care as a potential barrier.
Barriers identified by professionals
Discussion
Our results demonstrate that collaborations can be improved and both specialties are positive about the impact the new SIPC service will make. However, the barriers identified highlight areas for consideration and further exploration. Patient perceptions of palliative care was identified as a potential barrier to the successful integration of neurology and palliative care services. It is equally important for neurology professionals to have the right understanding of palliative care and to recognise the potential benefit of palliative care for their patients. Indeed, previous studies have demonstrated that the topic of palliative care can still often lead to anxiety in patients, caregivers as well as healthcare professionals.7 8 There is an emphasis on the need for integrated working along with improved education and awareness in order to make palliative care more recognised and more accessible for non-cancer conditions such as LTNCs.9 10 As reported by both specialties, resources must be carefully considered and systems developed for calling on palliative care specialists when truly necessary. The small number of respondents highlights the challenges of conducting research among busy health professionals; however, the geographical variation is an advantage of the survey.
Conclusions
Our results demonstrate the opportunity to increase collaboration between neurology and palliative care services for people with progressive neurological conditions, and the acceptability of SIPC as a model to support this. This survey will be repeated at the end of the trial to understand how collaborations and views have changed, whether the SIPC service has affected the care process and to identify areas for improvement. These survey results will be integrated with the qualitative trial findings to provide a wider context about the effects of SIPC on the processes of care, and the ways in which it might be working effectively.
Acknowledgments
The authors thank the research teams in the six UK sites for facilitating this work and the neurology and palliative care professionals who took the time to complete the survey. The authors also thank the OPTCARE Neuro PPI committee, in particular Dr Cynthia Benz, for their comments and support in the preparation of this report.
Footnotes
Contributors NH was responsible for the data collection, data analysis and for the initial draft and subsequent versions of this manuscript. WG, CJE, DJ, LMW, AB, VC, KEG, FL and IJH all contributed to the conception and design of the work, commented on the initial draft and approved the final version of the manuscript.
Funding WG, CJE, DJ, AB, VC and IJH had financial support from the National Institute for Health Research (NIHR), Health Services & Delivery Research programme (HS & DR) (12/130/47) for the submitted work. WG and IJH also had financial support from the NIHR Collaboration for Leadership in Applied Health Research & Care (CLAHRC), South London. In addition, CJE is funded by an Health Education England/NIHR Senior Clinical Lectureship and IJH holds an NIHR Emeritus Senior Investigator award.
Disclaimer The views expressed are those of the authors and not necessarily those of the National Health Service, NIHR or Department of Health.
Competing interests None declared.
Ethics approval National Research Ethics Service Committee London South East.
Provenance and peer review Not commissioned; externally peer reviewed.