Article Text

Abstract
Objectives Achieving congruence between preferred and actual place of death is increasingly being used as a quantifiable indicator of the effectiveness of palliative care services. Current secular trends indicate a reversal of the institutionalisation of death, but this has been more pronounced in patients with malignant disease. As such, this study was conducted to evaluate whether the preservation of autonomy has been addressed equitably for cancer and non-cancer populations.
Methods A systematic review and meta-analysis was performed in line with recommendations from Preferred Reporting Items for Systematic Reviews and Meta-Analyses and the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines. A comprehensive computerised search of 14 databases, supplemented by a manual review of the literature was performed for all peer-reviewed publications, from 1980 to the present, identifying rates of incongruence for cancer and/or non-cancer cohorts. Aggregation of outcomes was performed using a random effects model.
Results A total of 26 articles were identified that met the search and inclusion criteria. A non-cancer diagnosis was found to significantly increase the incidence of incongruence with a weighted risk ratio of 1.23 (95% CI 1.01 to 1.49, p=0.04) and this disparity appears to have increased since 2004. A moderate degree of heterogeneity was noted (I2=62%).
Conclusions These findings pose a significant challenge, as a ‘good’ death has been closely matched to achieving patients’ wishes, including preferred place of death. Despite increasing awareness that those dying from chronic non-malignant diseases have extensive palliative care needs, much is still to be done to preserve their autonomy and reduce powerlessness in the face of death.
Statistics from Altmetric.com
Introduction
Debates relating to what constitutes a ‘good death’ often place particular emphasis on being pain free, peaceful and dignified.1 Since 2004, achievement of preferred place of death for terminally ill individuals has also increasingly been used as a quantifiable indicator of the effectiveness of palliative care services.2
To date, despite enormous efforts to resolve deficiencies in fulfilling the wishes of terminally ill individuals, suggestions of low levels of congruence, defined as the ‘agreement between a patient's stated preferred place of death and actual place of death’ remain.3 While population studies have indicated that the majority of people prefer to die at home, secular trends towards an institutionalised death have been reported in many countries.4
Encouragingly, evidence of a reversal of this trend has been demonstrated in the UK, largely due to the commitment and dedication of the palliative movement.4 However, palliative care services have traditionally concentrated on the needs of a minority of people with advanced incurable disease, typically cancer patients5 and unfortunately, this reversal has been noted to be significantly more pronounced in cancer than in non-cancer deaths.4
Although home represents the preferred place of death for the majority of terminally ill individuals,3 this wish is certainly not shared by all. Inconsistent trend reversal alone, therefore, is unable to confirm whether autonomy and choice is being addressed inequitably for cancer and non-cancer groups.
Current observations do, however, seem to imply lack of choice at end-of-life,3 especially for patients with non-malignant disease, yet evidence of an association between disease process and incidence of incongruence, has not been systematically compared across studies to date. As such, this multinational systematic review and meta-analysis was conducted to evaluate whether those who die of malignancy are being disproportionately ‘singled out for deluxe dying’6 in locations of their choice.
Methods
Literature search
A comprehensive literature review was conducted between April and October 2012. All available electronic databases including the BNI, CINAHL, Cochrane Library, EMBASE, AMED, HMIC, PsycINFO, Intute: Health & Life Sciences, MEDLINE, PubMed, BIOSIS Previews, ISI Web of Knowledge, ISI Web of Science and IgentaConnect, were systematically searched, between 1980 to the present for all English and non-English language articles.
The following Medical Subject Heading (MeSH) terms and free text terms were used: (choice OR preference OR decision OR wish) AND (palliative OR terminal OR end-of-life OR hospice OR elderly OR aged) AND (care or death) AND (place OR location OR site). No search limits were used and further searches were performed to obtain articles from the bibliographical sections of the studies identified from the original search. The titles and/or abstracts of all identified studies were reviewed and full manuscripts obtained for those that appeared potentially relevant.
Selection criteria
Articles were included if they reported original data quantitatively comparing adult patients’ preferred place of death and actual place of death. These articles were included if they assessed cancer only groups, non-cancer only groups or mixed cancer and non-cancer populations where sufficient information was provided to determine congruence for both groups separately. All articles were included irrespective of whether congruence was the primary or secondary purpose of the study.
Articles that did not report either congruence, or both patients’ preferred place of death and actual place of death, were excluded. Studies eliciting preferred place of care rather than place of death were also excluded, as these have been shown to be different outcomes.7 Studies were, however, included if the studies assessed preferred place of final care, as this was felt to accurately reflect preferred place of death.
Studies focusing exclusively on nursing home patients and patients receiving non-uniformly available visiting nurse station support in their homes, were excluded. Studies exclusively examining children and those studies examining association of place of death with subsequent events (including bereavement problems) rather than pre-existing preference, reviews, duplicate data, comments, case histories, qualitative studies and unpublished material were also excluded.
Data extraction
Standardised forms were used for reviewing each article and the following data was extracted and systematically entered into a matrix table: source population, study design, patient diagnosis, grade of study, congruence by location, overall congruence and incongruence rates for cancer and/or non-cancer patient groups where applicable.
Overall congruence for each study and each cancer and non-cancer cohort was determined by dividing the number of subjects with met preferences for any location of death by the number of subjects with a recorded preferred place of death while incongruence was determined by dividing the number of subjects with unmet preferences for any location of death by the number of subjects with a recorded preferred place of death. This allowed for exclusion of those patients who were unwilling or unable to express a preference for place of death, resulting in potential alteration to the reported congruence values of the included studies. MJB extracted the data from the papers and SJB assessed a 35% random sample of papers to ensure an accurate data extraction process.
Quality assessment and grading of evidence
All studies included in the analysis were graded using quality measures defined previously.3 These criteria were as follows: grade A (strong evidence): longitudinal study with standardised systematic and pre-defined assessment of preference for place of terminal care or death, more than 80% response rate (if survey study), patients not limited to those within one service, (eg, one palliative care team); grade B (moderate evidence): longitudinal study that does not meet criteria for A, cross-sectional, observational, or retrospective study, more than 60% response rate (if survey study), standardised and systematic assessment of preference for place of terminal care or death; and grade C (weak evidence): response rate less than 60% or not given (if survey study), or inconsistent assessment of preferences.
Analysis
Meta-analysis was performed in line with recommendations from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses and Meta-analysis Of Observational Studies in Epidemiology (MOOSE) initiative guidelines.
Assessment for association
In order to analyse rates of incongruence for the cancer and non-cancer groups, statistical analysis was carried out using weighted risk ratio estimates, comparing the non-cancer group with the reference (cancer) group using a random effects model. A weighted risk ratio less than 1 was set to favour the non-cancer group while a weighted relative risk greater than 1 was set to favour the cancer group. The point estimate of the weighted relative risk estimate was considered statistically significant at the p<0.05 level if the 95% CI did not include the value 1. All statistical analysis was conducted with Review Manager V.5.1 (Cochrane Collaboration, Oxford, UK).
Heterogeneity
A measure of the extent of variation among the effects observed in different studies was incorporated to assess the generalisability of the combined results. Statistical quantification of inconsistency was performed using Cochran's Q and I2.
Results
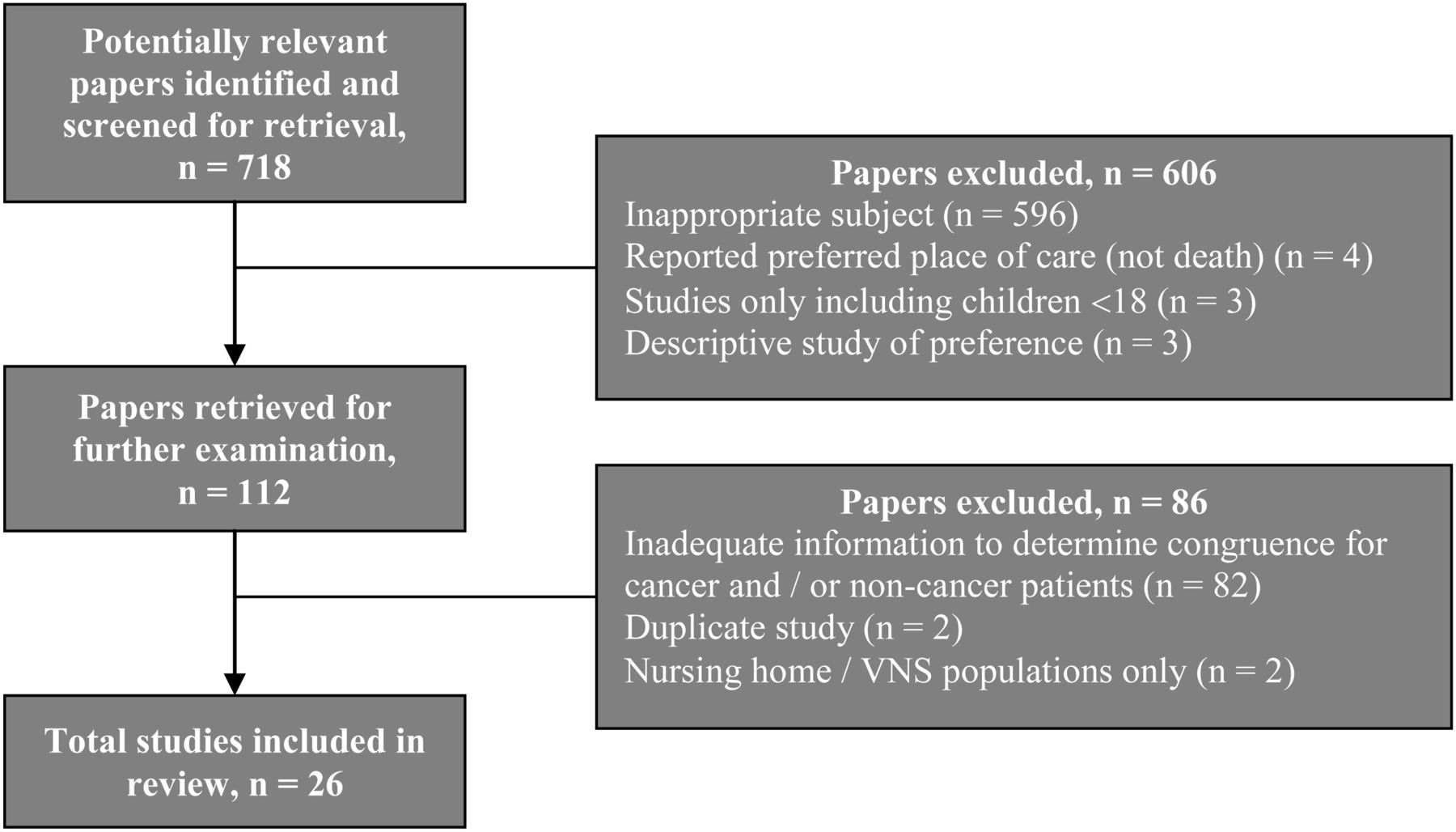
Overall, 718 unique citations were identified and a flow chart of the inclusion and exclusion of studies is shown in figure 1. Studies presenting inappropriate subject matter (n=596), reporting preferred place of care, not place of death (n=4), exclusively examining nursing home (n=1), home with visiting nurse station support (n=1), paediatric populations (n=3) and descriptive studies of preference (n=3) were excluded. Studies presenting duplicate data (n=2) and articles that did not report either congruence, or patients’ preferred place of death and actual place of death concurrently, for a cancer and/or a non-cancer cohort, were also excluded after close inspection of the full article (n=82).

Study selection process.
Characteristics of studies
Twenty-six articles met the inclusion criteria.8–33 Only four studies provided comparative data for a cancer and non-cancer cohort with two studies focusing on congruence specifically for separate cancer and non-cancer cohorts13 ,33 and the remaining studies examining preferences as a factor associated with place of death.8 ,15 Seventeen studies provided non-comparative data for cancer patients only,9–12 ,14 ,16 ,18–20 ,23 ,25 ,26 ,28–32 while five studies analysed congruence for non-cancer patients exclusively.17 ,21 ,22 ,24 ,27
A κ statistic of 0.77 was noted between the study evaluations by MJB and SJB, indicating substantial interobserver agreement. Unfortunately, inadequate information was provided to determine κ statistics for agreement between preferred and actual death in 21 studies,8–18 20–27 ,32 ,33 precluding further use of the statistic for cross-study comparison in this review.
Of the included studies, twelve were from the UK,13–15 ,17 ,21–24 ,26 ,29 ,31 ,33 four were from the USA10 ,20 ,27 ,28 and two were from the Netherlands.8 ,32 Spain,9 Italy,11 Denmark,12 Japan,16 Sweden,18 Taiwan,19 Belgium25 and Ireland30 each had one study included. Overall, a non-European nationality was associated with a statistically significant increased risk of incongruence between preferred and actual place of death. The non-weighted risk ratio of incongruence for non-European patients (39.7%) compared with European patients (31.4%) was 1.26 (95% CI 1.19 to 1.34, p<0.0001).
Table 1 summarises the study descriptions, source populations, study design, patient diagnosis, the rates of incongruence of the cancer and non-cancer cohorts and grading of each study.
Characteristics of included studies
Four prospective studies were graded A level.28 ,29 ,31 ,33 Eleven studies were graded B level because of retrospective design, single-service populations, or response rates less than 80%.8 ,9 ,11 ,13 ,14 ,17 ,19 ,22 ,26 ,27 ,30 Eleven studies were also graded C level because of response rates less than 60% or inconsistent assessment of preferences.10 ,12 ,15 ,16 ,18 ,20 ,21 ,23–25 ,32
The grade B and C studies were noted to produce a significantly greater mean overall congruence (68.2% and 62.3% respectively) than the grade A studies (42.3%) with a wide range of overall congruence noted for each grade. Two grade C studies reported only home congruence.16 ,18 Seven studies—two grade A,28 ,33 three grade B8 ,19 ,30 and two grade C,12 ,24 reported less than 50% overall congruence.
Illness factors and congruence
Seventeen studies included cancer-only patients,9–12 ,14 ,16 ,18–20 ,23 ,25 ,26 ,28–32 while three mixed population studies included more than 85% of patients with cancer.13 ,15 ,33 These 20 studies noted a wide range of overall congruence of 30–89%. Five studies exclusively examined non-cancer patients,17 ,21 ,22 ,24 ,27 with one mixed-population study reporting on less than 40% of patients with cancer.8 These six studies also noted a wide range of overall congruence of 30–66%. There was no clear correlation between levels of overall congruence and the percentage of patients with cancer diagnoses (p=0.18).
Analysis of incongruence according to diagnosis group (cancer or non-cancer) was based on 5036 (64.0%) congruent and 2840 (36.0%) incongruent deaths in 7876 participants. Overall, 232 (45.3%) incongruent deaths occurred in 512 participants without cancer and 2608 (35.4%) incongruent deaths occurred in 7364 participants with a cancer diagnosis. Overall, a non-cancer diagnosis was associated with a greater risk of incongruence between preferred and actual place of death (figure 2). The weighted risk ratio for incongruence for non-cancer patients compared with cancer patients was 1.23 (95% CI 1.01 to 1.49, p=0.04). A moderate degree of heterogeneity was observed (I2=62%).

Incongruence risk ratio forest plot according to diagnosis.
Secular trends and reversal of institutionalisation of death
Nine studies were published prior to 2004, including seven cancer-only,14 ,16 ,18 ,23 ,28 ,30 ,31 one non-cancer only17 and one mixed cancer and non-cancer populations,15 while 17 studies were released after the achievement of preferred place of death was brought to the forefront of the medical community.34 ,35 Ten of these studies included only cancer participants,9–12 ,19 ,20 ,25 ,26 ,29 ,32 four included only non-cancer participants21 ,22 ,24 ,27 and three included cancer and non-cancer cohorts.8 ,13 ,33
In line with the aforementioned reversal of secular trends, indicating greater emphasis on meeting terminally ill patient's wishes, there was a significant overall reduction of incongruence since 2004. This improvement was significantly more pronounced for cancer patients than non-cancer patients (p=0.0095) (table 2).
Temporal trends of overall incongruence and relative risk of incongruence
Preferred location of death
Only four studies reported preferences for every patient in the sample.17 ,19 ,28 ,33 In the remaining studies, 12–62% of patients did not express a preference for place of death.8–16 ,18 ,20–27 29–32 Twenty-one studies specifically identified rates of preference for home death. In sixteen of these studies more than 50% of participants preferred home deaths, after disregarding patients without an expressed preference,9 ,11–16 ,19 ,20 ,22–24 ,28 ,30 ,32 ,33 while five studies reported on less than 45% of patients expressing a wish to die at home.17 ,18 ,25 ,29 ,31 Overall, 79.5% of participants reporting a preference expressed a desire to die at home. Two studies reported only on 79%16 and 37%18 of their populations, who spontaneously expressed a preference for home death and did not elicit or report any other preference.
Analysis of incongruence according to preferred place of death (home or non-home) was based on 308 (31.0%) incongruent deaths in 995 participants preferring a non-home death and 2150 (37.6%) incongruent deaths, which occurred in 5721 participants preferring a home death.
Overall, a home preference was associated with a non-significantly increased risk of incongruence between preferred and actual place of death (figure 3). The weighted risk ratio for incongruence for individuals preferring a home death compared with individuals preferring a non-home death was 1.17 (95% CI 0.84 to 1.64, p=0.36). A substantial degree of heterogeneity was noted (I2=73%).

{kind=link}
{kind=link}
{kind=link}
Incongruence risk ratio forest plot by preferred place of death.
Overall, there was no significant difference between cancer (62.3%) and non-cancer patients (68.4%) in the rate of achievement of preference for those preferring a home death (p=0.095).
Discussion
Enabling a ‘good’ death is closely matched to meeting patients’ wishes. Although congruence has significantly improved since 2004, admissions relating to deficiencies in provision of choice at end-of-life have, sadly, become commonplace, especially in patients with non-malignant disease. In line with these admissions, this pooled analysis of 7876 participants from 26 observational studies has demonstrated that a non-cancer diagnosis is associated with a statistically significant 23% increase in the incidence of incongruence (p=0.04) and disconcertingly for non-cancer patients, this trend has become more pronounced since 2004.
Recent debate on the provision of palliative care as an international human right has included the assertion that there should be equity of access to services for all, without discrimination.36 Few can argue with the merit of this objective, yet as evident from the findings of this study few can deny the presence of serious inequalities according to patient diagnosis.
The first major challenge is to enhance recognition of terminal illness. The diagnosis of dying is often made too late, however, approximately two-thirds of all deaths are non-sudden and protracted and can be anticipated.37 Early recognition of impending death allows for better management of dying patients, although it is widely appreciated that this is more challenging for non-cancer patients, whose illness trajectories are relatively more complicated and less predictable.8 Development of simple, well-validated prognostic models with good calibration and reliability may aid this process.
The second major challenge is to enhance investigation of preference. The 56.5% completion rate of preference from the 26 studies is disconcerting. In part this may be due to patient unwillingness and inability to participate in discussion but may also indicate a lack of ascertainment of preference for a considerable willing and able proportion. Having cancer, as opposed to other diagnoses, has been positively associated with increased discussion of end-of-life issues38 and awareness of preferred place of death8 and it will come as no surprise that patients who receive more healthcare contact and have their preferences assessed tended to die more often in a preferred place.39 In non-malignant disease the lack of defined trajectories may leave those who believed they had more time to consider their options unable to express a preference, potentially escalated by healthcare staff insecurities in discussion and management of non-malignant disease.40
The third major challenge is to enhance provision of care. In recent general population studies of preference, 50–90% of respondents have expressed a preference to die at home.3 However, without assistance, the end-of-life stage is a crucial testing time, especially when the decedent is at home.41 If strong support is not readily available some caregivers will be unable to bear the strain and unplanned admission may be necessary. These crises can be successfully avoided if families are well prepared and support is readily available.41
Although the goal of reducing inequity and providing care for patients on the basis of need rather than diagnosis is widely acknowledged36 given the low proportion of non-cancer patients managed by palliative care teams in the UK, sufficient clinical exposure to bridge these deficiencies is unlikely to be rapidly forthcoming.
Instead, measures to improve recognition of the terminal phase, investigation of individual preferences and the provision of services should be opened up to non-palliative care specialist clinicians, groups currently caring for non-cancer patients and health service commissioners. These potential ‘agencies for change’ may possess important insights into patient needs, input into the management of experiences and deficiencies, and perhaps assist in the development of innovative services to preserve autonomy.
Limitations
Although the Cochran Q test does not demonstrate significant heterogeneity (p=0.11), the I2 value (62%) does suggest a moderate degree of inconsistency of individual study findings in relation to the primary outcome measure. A substantial degree of heterogeneity (I2=73%, p<0.00001) was also observed in relation to the differing incongruence rates according to preferred place of death.
Some of this inconsistency may be explained by the constitution of the cancer and non-cancer cohorts. Patients with haematological malignancy, for example, have been shown to be more likely to die in hospital than other cancer diagnoses,42 and patients with colorectal carcinoma have been shown to be more likely to die at home.43 Therefore, it is plausible that patients with certain types of cancer may be more or less likely to have their end-of-life preferences achieved and that if there are inter-study systematic differences of cancer type, this may be responsible for some of the heterogeneity observed.
No randomised controlled trials were available for inclusion and most studies included were small and observational, with incomplete assessment of preference within a majority of studies. Smaller studies are often conducted and analysed with less methodological rigour than larger studies and in observational studies confounding variables may negate the findings. This confounding effect is compounded by the more comprehensive approach used, which allowed for inclusion of non-comparative studies exclusively studying cancer or non-cancer participants. In addition, the range of nationality of the included studies, where differing end-of-life care provisions and policies exist, heightens this confounding effect.
Selection bias is also a significant drawback of the included studies and therefore this meta-analysis. Population studies have suggested that only a minority of all dying patients receive specialist palliative care management.44 Since involvement of these teams has been associated with increased congruence across many studies,3 ,28 ,45 given that most of the participants of the included studies were under the care of such specialists, this limits the generalisability. In addition, surveys have indicated that well over 95% of all patients seen within specialist palliative care services have cancer.5 In comparison, given that approximately 7% of all participants in the included studies had a non-cancer diagnosis, there is a substantial over-representation of these patients and it is plausible, therefore, that these findings are only a conservative estimate of the true effect.
Conclusion
In summary, this meta-analysis has demonstrated a significant association between a non-cancer diagnosis and increased incidence of incongruence between preferred and actual place of death and that this relationship is becoming more profound. Over the next decade this shift may become increasingly important, given that in Britain the overall numbers of deaths are expected to rise substantially in the near future4 and that the majority of these deaths are predicted to be attributable to a non-cancer diagnosis.46 With the resultant increase in end-of-life needs that is predicted, it is vital to develop investment plans and services that meet the requirements of ageing populations and ensure the best possible outcomes for terminally ill patients and their families wherever they wish to be and whatever their diagnosis.
Acknowledgments
The authors would like to thank the helpful and friendly staff of the Douglas Macmillan Hospice and the Health Library for North Staffordshire for their inspiration and assistance. We are also grateful to Dr MS Billingham and Mrs MR Billingham for their insightful review and guidance in the preparation of the final manuscript.
References
Footnotes
-
Contributors MJB and SJB were responsible for overall conceptualisation of the paper, contributed to the design and construction of the review, performed the literature review, analysed the extracted papers with particular reference to data and statistical analysis and produced draft versions and the final version of the document. Both authors have also reviewed the content of the final document and have approved this final manuscript.
-
Funding None.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.