Article Text

Abstract
Objectives Financial pressures and competing demands for limited resources highlight the importance of defining the unmet need for specialty inpatient palliative care (PC), demonstrating the value of the service line and making decisions about staffing. One measure of access to specialty PC is penetration, the percentage of hospitalised adults receiving PC consultations. Although useful, additional means of quantifying programme performance are required for evaluating access by patients who would benefit. The study sought to define a simplified method of calculating unmet need for inpatient PC.
Methods This retrospective observational study analysed electronic health records from six hospitals in one health system in Los Angeles County.
Unmet need for PC was defined by the number of hospitalised patients with four or more chronic serious comorbidities without a PC consultation divided by a denominator of all patients with one or more chronic serious conditions (CSCs) without a PC during the hospitalisation.
Results This calculation identified a subset of patients with four or more CSCs that accounts for 10.3% of the population of adults with one or more CSCs who did not receive PC services during a hospitalisation (unmet need). Monthly internal reporting of this metric led to significant PC programme expansion with an increase in average penetration for the six hospitals from 5.9% in 2017 to 11.2% in 2021.
Conclusions Health system leadership can benefit from quantifying the need for specialty PC among seriously ill inpatients. This anticipated measure of unmet need is a quality indicator that complements existing metrics.
- Chronic conditions
- Quality of life
- Supportive care
- Service evaluation
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Palliative care penetration based on all non-obstetrics adult admissions is a common measure of access to palliative care in hospitals. However, it is an imperfect method of estimating the need for palliative care services by seriously ill hospitalised patients.
WHAT THIS STUDY ADDS
Quantifying the number of patients with four or more serious medical conditions prior to an acute hospitalisation can support decisions impacting program staffing and deployment of palliative care services to patients with probable needs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study reports development of an easily adoptable method for healthcare system leaders to gauge current unmet patient needs for specialty palliative care. This new metric offers researchers a method for tracking unmet needs for palliative care by seriously ill hospitalised patients and measuring the impact of health service interventions on those needs.
Introduction
Specialty palliative care (PC) can improve quality of life for patients and their families by assessing and responding to their physical, psychosocial, social and spiritual needs through an interdisciplinary approach to care.1 Particularly when services are provided early and concurrent with disease treatments, PC is associated with more frequent advance care planning, better patient and caregiver satisfaction, less hospital days, improved quality of life and lower healthcare costs.2–6 Hospitalised patients with multiple or advanced serious illnesses can be expected to benefit from specialty PC services.7 8 In recent years, many healthcare systems have expanded their PC service lines and a large majority of hospitals with over 50 beds now have a PC programme.9 However, clinical capacity of specialty PC programmes remains insufficient to serve all patients who might benefit and may delay access to these valuable PC services.10 11
In response to a growing population of people living with serious illness, healthcare systems are expanding specialised inpatient and outpatient PC services.12 13 Hospitals have been encouraged to proactively identify patients who would benefit from specialised PC services and capture data about unmet needs.8 Within the USA, palliative medicine and nursing organisations have focused on identifying and evaluating potential benchmark indicators of access to and quality of PC services.14–16In the USA Australia and South Africa, methods of predicting death within 12 months have been evaluated as potential triggers for PC referral and access metrics.8 17 18Screening tools, such as the Supportive and Palliative Care Indicators Tool, have been developed to identify patients who might benefit from PC services.19 20The existing metrics evaluate overall performance of PC programmes and not the needs of individual patients for PC services. However, healthcare systems would benefit from system-level measures of the extent to which PC programmes are meeting the needs for the seriously ill population.21
PC penetration is a commonly used metric of access to hospital-based PC services. PC Penetration is calculated by the number of initial PC consults divided by the total number of non-obstetrical adult hospital admissions during a defined period of time.22 Reported rates for annual PC penetration in the USA range from 3.6% to 7.3%.23 When services are maximised, PC penetration rates could range from 17.6% to 26.4% of the total inpatient population.23 These findings are consistent with studies suggesting that prevailing PC penetration rates likely do not meet the actual need for PC services among hospitalised patients.23
Health systems administrators are understandably interested in focusing existing PC resources where they are needed most and, similarly, expanding PC services when and where there are unmet needs. Common methodologies for estimating the number of hospitalised patients who would benefit from specialty PC rely on broad generalisations that may not fit a specific hospital’s casemix. These limitations also make it difficult to monitor productivity and performance or calculate value. Existing metrics of access, such as penetration and timeliness of referrals and consultations, such as the proportion of PC consultations performed within the first hospital day, provide an incomplete picture of programmatic performance.
Additionally, while PC penetration is useful, it is a crude measure. The denominator encompasses all non-obstetric adult patients, many of whom do not require PC services. The metric is not responsive to a specific hospital’s casemix and acuity. These limitations reduce the utility of relying on PC penetration in determining the right size of an institution’s PC programme. These considerations also diminish the relevance and utility of national PC penetration rates as PC programme benchmarks and performance targets. Some researchers have suggested refining PC penetration using an algorithm that factors in serious diagnosis(es), hospital utilisation, functional status and uncontrolled symptoms.23 Additional meaningful ways of quantifying patient need for PC at individual hospitals would assist system leaders in knowing when and where to expand PC programmes and services and in optimally deploying existing clinical resources.
Aim
We explored a pragmatic approach to defining and calculating unmet need for PC services among hospitalised patients. We hypothesised that this unmet need for PC metric would provide a meaningful tool for PC programmes and healthcare system leaders to use in monitoring patient need, making decisions about PC programme staffing, scope of services, service hours and deployment, and tracking programmatic outcomes. We developed this metric in response to our system leaders’ request for ways to quantify patient need and justify investments to expand the PC service line.
Methods
Design
We employed a retrospective observational design to achieve study aims.
Setting/participants
The data source for this study was the electronic health record (EHR) of six hospitals within a non-profit healthcare system in Los Angeles County, California that uses a single instance of Epic EHR. The target sample for this study was non-obstetric adult patients having at least one illness within the nine Dartmouth Atlas categories of chronic illness: (1) malignant cancer ; (2) chronic pulmonary disease; (3) coronary artery disease; (4) congestive heart failure; (5) peripheral vascular disease; (6) severe chronic liver disease; (7) diabetes with end organ damage; (8) renal failure or (9) dementia.24 A 10th category for chronic, non-dementia-related neurological disease was defined in collaboration with the Dartmouth Atlas team and added to our analysis. For this study, we also converted 280 International Classification of Diseases (ICD)-9 codes included in the existing Dartmouth Atlas definitions to ICD-10 codes. With the added specificity to ICD-10 for severity of illness, we completed clinical review of the converted codes and removed ICD-10 diagnosis codes with less severity of illness, such as mild intermittent asthma or diabetes without end organ damage, which would be unlikely to indicate need for an inpatient specialty PC consultation. Online supplemental appendix one contains a full summary of modifications to the Dartmouth Atlas ICD-10 table.
Supplemental material
Data analysis
Hospitalised patients with ‘unmet need for PC’ were defined as those with four or more chronic illness diagnoses (from the 10th modified Dartmouth Atlas categories) on admission to an acute care hospital who were discharged alive without having received consultation by the hospital’s PC team. The numerator (number of patients with four or more diagnoses of chronic serious conditions (CSCs) who did not receive a PC consult) is divided by the denominator (total number of patients with one or more diagnoses of serious illness who did not receive a PC consult during the hospitalisation) to yield the ‘unmet need for PC’ (figure 1.) Hospitalised patients with observation status were not included. Patient-level data were extracted from inpatient encounters discharged within calendar years 2017 and 2018. Data included hospital location, admission details, PC consultations and ICD-10 billing codes. Only charts with complete datasets were used.
Data were extracted from a cloud data warehouse hosting copy of EHR database and analysed via Python programming language on a secure server to identify patients with billed ICD-10 codes for seriously ill diagnoses (see online supplemental appendix one) and stratified by the number of comorbidities. For example, a patient whose EHR contained ICD-10 codes for breast cancer, coronary artery disease and congestive heart failure would be categorised as having three CSCs.
This study meets all five of the CODE-EHR minimum framework standards for the use of structured healthcare data in clinical research; https://doi.org/10.1136/bmj-2021-069048.
Results
During 2017 and 2018, a total of 92 047 adult, non-obstetrical patients had 142 069 admissions to the 6 study hospitals. Patients were on average 64 years old and spent an average of 4.5 days in the hospital. During these 2 years, 5.1% (4729 patients) died in the hospital. More than half of hospitalisations (74 430) involved patients with one or more category of pre-existing CSC. PC consulted on 8544 admissions, yielding an annual PC penetration of 6.0%. As shown in online supplemental table 1, patients with four or more comorbidities were older and had more admissions, higher rates of in-hospital deaths (13.6%) and longer average length of stay (6.9 days) than the total population of hospitalised patients.
Supplemental material
During this 2-year period, 5246 patients with 4 or more qualifying diagnostic codes of CSC had 8245 hospitalisations. PC consultations were not performed for 4211 (80.3%) of these patients, corresponding to 6832 (82.8%) of these hospitalisations.
Unmet need for PC during this 2-year period was 10.3%, calculated by dividing the numerator of 6832 hospitalisations of those with four or more categories of CSC by the denominator of 66 592 hospitalisations of patients with one or more category of CSC who did not receive a PC consultation (figure 2). This population (included in the numerator) also represents 4.8% of all non-labour and delivery adult hospitalisations.
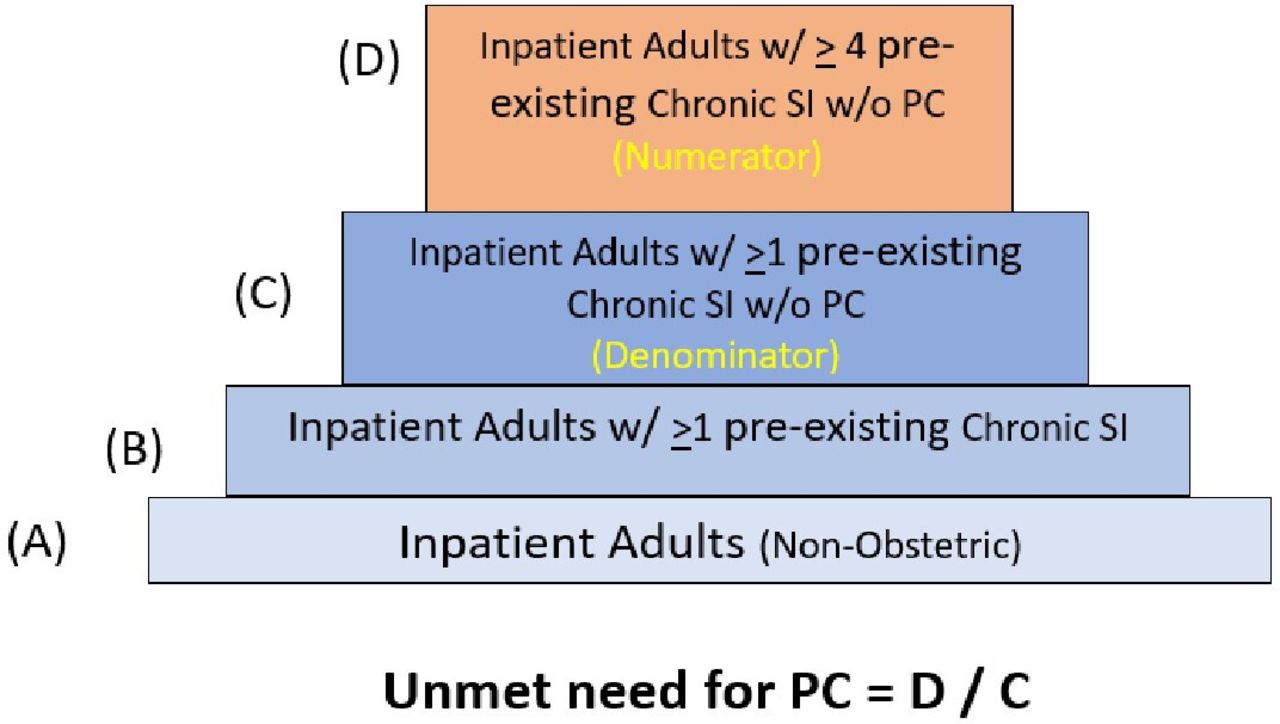
Unmet need calculation method. Unmet need for palliative care (PC) is calculated by dividing the number of hospitalised adult (non-obstetric) patients with one or more pre-existing serious chronic conditions (SI) who did not see palliative care (denominator) into the numerical subset those patients with four or more serious chronic conditions (numerator).
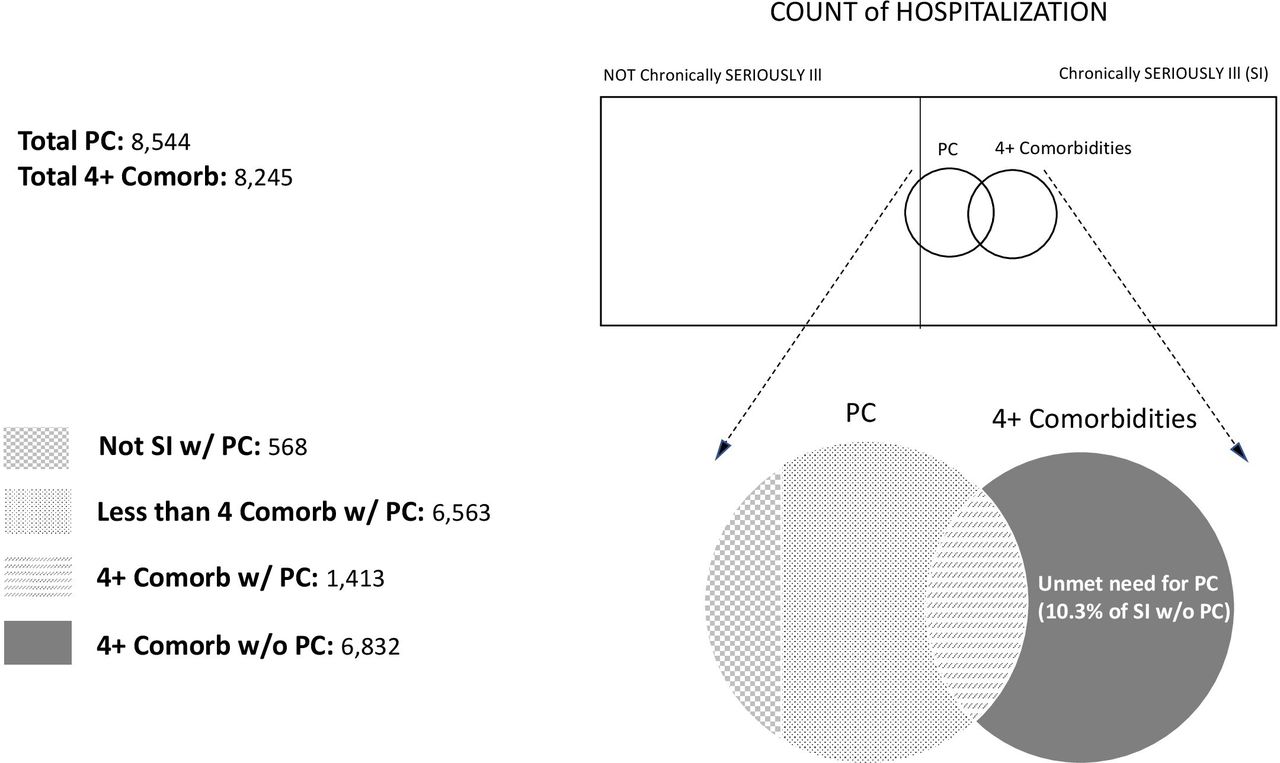
Inpatient patient distribution by serious illnesses and palliative care (PC) consultations.
A small number of patients (111 with 1 or more categories of CSC) were referred to PC but did not have a consultation completed prior to discharge or death. Reasons for not receiving the consultation included death prior to the consultation, and patient and/or family members not being able to meet with the PC team.
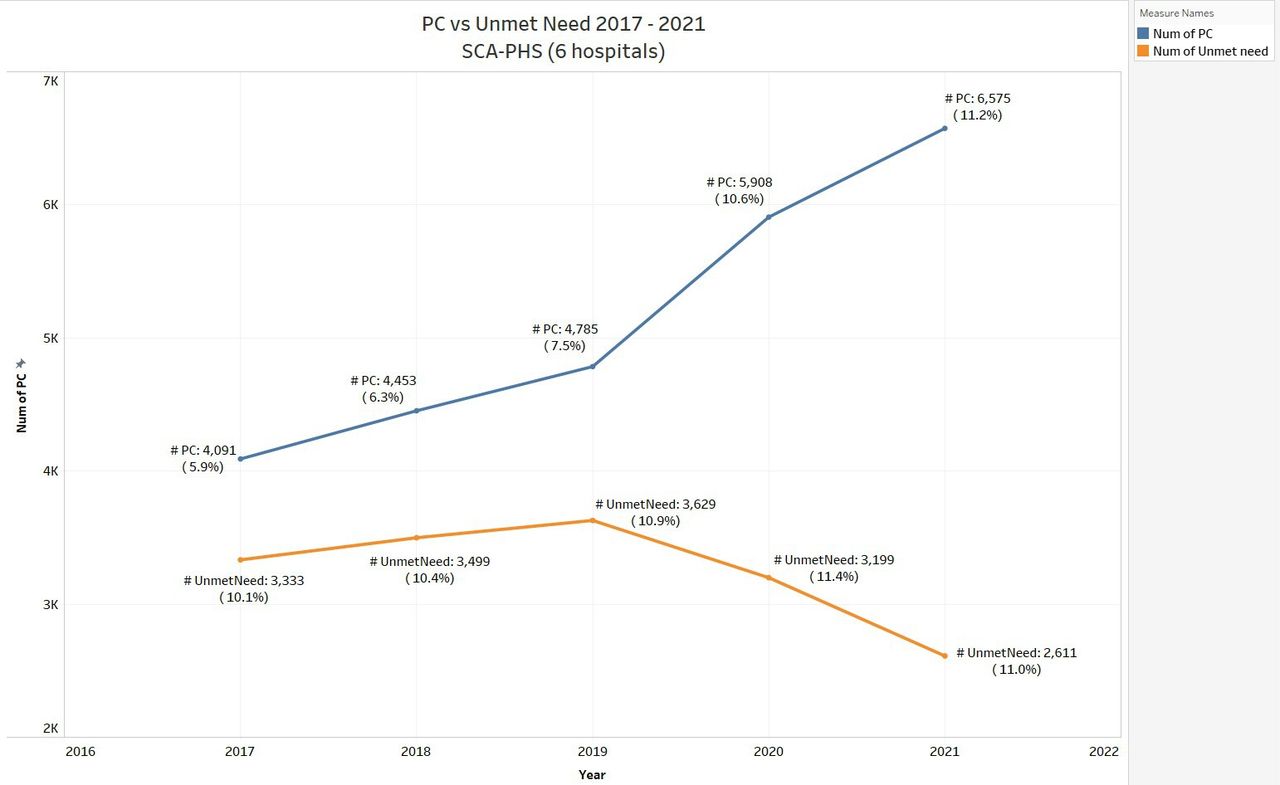
A review of PC penetration compared with PC unmet in the 5 years following integration of PC unmet need into each hospital’s monthly PC key operational dashboard shows improvement in access to specialty PC service by patients with four or more chronic conditions (figure 3). The number of PC consultations increased from 4091 in 2017 to 6575 in 2021. Unmet need decreased from 3333 patients in 2017 to 2611 in 2021.
{kind=link}
{kind=link}
{kind=link}
PC versus unmet need 2017–2021. Los Angeles County Six Hospitals. PC, palliative care.
The unmet need metric for PC has been embedded within monthly operational scorecards of specialty PC programmes, which are reviewed by senior leadership of hospitals at monthly operational meetings. As a result, PC programme leaders are equipped with timely data to participate in resource allocation deliberations that can support programme expansions. Drawing on data reported in these monthly dashboards, three of the hospitals included in this study approved staffing increases during their budget processes.
Discussion
This approach to quantifiably estimating unmet need for PC among hospitalised patients complements existing PC programme measures. It provides a readily calculable, meaningful and practical metric for PC programme development and performance monitoring.
We recognise that many patients living with even a single CSC might benefit from specialty PC consultation and continuity of care during an acute care hospitalisation. However, individuals with multiple chronic conditions can be expected to encounter complex decisions regarding medical treatments, experience disease-related symptoms, require coordination of healthcare services and incur substantial costs from increased healthcare utilisation.25
For the foreseeable future, limitations of PC staffing and resources will require deploying PC services to patients who are likely to need them most. Our calculation provides a conservative estimate of unmet need for PC, identifying a subset of all hospitalised patients with serious illness who did not receive PC. This metric assumes that, categorically, patients with four or more chronic serious comorbidities are more likely to experience a higher burden of illness and complexities of care. When they become acutely ill and require inpatient care, they would likely benefit from a PC consultation.
Empiric data support this assumption. A published meta-analysis found important differences in the estimated effect of treatment for patients with four or more comorbidities compared with two or fewer if PC consult occurs within the first 3 days of admission.26 In poststudy follow-up, we found that 22% of the 4211 patients with four or more categorical serious illnesses hospitalised during 2017 and 2018 without receiving PC died within 2 years post hospitalisations. It is reasonable to assume that during many of the 6832 hospitalisations, of which 2621 were readmissions, these 4211 patients could have benefited from specialty PC services.
In designing this metric, we built from studies of PC need and consensus statement recommendations1 4 8 in developing an easily adaptable method for the healthcare system leadership to gauge the magnitude of needs of seriously ill patients that could benefit from expanding access to specialty PC. To enhance applicability and scalability, this metric was designed to be calculated from a few data elements readily extractable from the EHR.
This unmet need for PC metric can be used to support expansion of specialty PC services and programme staffing. Volumes and trends in admissions of seriously ill patients can guide decisions related to access to PC services by currently unserved patient populations, including operating hours and days of the week.
By elucidating patterns of care for seriously ill hospitalised patients, rational tactics can facilitate PC service line growth. Potential operational steps include routine participation of PC team members in hospital medicine and intensive care daily rounds, presence of PC team members in emergency departments, predetermined best practice alerts for PC consult referrals and review of seriously ill patients with each readmission.
Further analyses are planned to identify specific categories of chronic illness or disease clusters associated with not receiving PC services during hospitalisations.
Investments required to expand staffing and enhance access to PC specialty services can be evaluated by analysing outcomes of interest for the affected population. These include, but are not limited to, rates of hospital readmission, rates of ICU admission, lengths of stay in hospital and ICU, per cent of in-hospital deaths, timing of referral to hospice and hospice lengths of service.
The sickest patients in our hospitals can be expected to have complex needs and deserve the highly specialised level of care and support that PC teams can deliver. This new unmet need for PC metric can assist healthcare systems in directing limited investment dollars. The metric can also contribute to national efforts to monitor access to PC services by a category of patients likely to need them most.
Limitations
This method of calculating unmet need for PC is conservative by design. Actual unmet need sporadically exists among patients with fewer chronic conditions and is not captured by this metric. Future EHR functionality and enhanced information systems may encompass personalised medical needs and specific life situations that identify patients who would benefit from PC. Our approach offers a reasonable step towards quantifiably estimating patient needs for the purposes of enhancing a PC service line in response to the needs of patients that a hospital serves and monitoring performance programmatically.
ICD-10 coding as criteria for serious illness has inherent limitations and could be enhanced with measurement of function and quality of life.27
Conclusion
The ability to quantifiably estimate the need for specialty PC among hospitalised patients is essential to healthcare system leaders who are responsible for developing, managing and monitoring the performance of PC programmes. PC penetration remains a useful, but inexact and incomplete metric. Unmet need for PC metric, as defined here, complements PC access and operational metrics and can help in setting and monitoring PC programmatic targets.
Data availability statement
Data are available upon request.
Ethics statements
Patient consent for publication
Ethics approval
The study was granted exempt status (STUDY2019000605) by the Providence St. Joseph Health Institutional Review Board.
Acknowledgments
Special thanks to Mr Paul Park for assistance with data acquisition and validation.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MPL, SG, MG, IB and NS contributed to planning. IB, MG, SG and NS collaborated and designed, validated and socialised the new metric. MPL and NS worked on the outline of the manuscript. SG and NS designed the method of data analyses and identified relevant indicators. SG developed coding script to query data from cloud data warehouse and implemented calculation methods. All coauthors contributed to drafting and revisions of the manuscript. MPL, MG and IB reviewed and provided feedback on the methods of analyses and results of the study. NS is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.