Article Text

Abstract
The need to improve access to palliative care across many settings of care for patients with cancer and non-cancer illnesses is recognised. This requires primary-level palliative care capacity, but many healthcare professionals lack core competencies in this area. Pallium Canada, a non-profit organisation, has been building primary-level palliative care at a national level since 2000, largely through its Learning Essential Approaches to Palliative Care (LEAP) education programme and its compassionate communities efforts. From 2015 to 2019, 1603 LEAP course sessions were delivered across Canada, reaching 28 123 learners from different professions, including nurses, physicians, social workers and pharmacists. This paper describes the factors that have accelerated and impeded spread and scale-up of these programmes. The need for partnerships with local, provincial and federal governments and organisations is highlighted. A social enterprise model, that involves diversifying sources of revenue to augment government funding, enhances long-term sustainability. Barriers have included Canada’s geopolitical realities, including large geographical area and thirteen different healthcare systems. Some of the lessons learned and strategies that have evolved are potentially transferrable to other jurisdictions.
- education and training
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What was already known?
Primary-level and specialist-level palliative care services are needed to meet the palliative care needs of a population, but professionals across many settings of care lack core palliative care skills.
Pallium Canada, a non-profit organisation founded in 2000, builds primary palliative care capacity through education and compassionate communities.
What are the new findings?
The programme has spread across Canada; from 2015 to 2019 alone, 1603 courses were delivered and over 28 000 professionals trained.
Several factors have helped or impeded spread and scale-up; drivers include strategic partnerships and a social enterprise model.
What is their significance?
The lessons learned offer insights into large-scale, national-level deployment of palliative care continuing professional programmes.
Large-scale interprofessional continuing professional development is viable and impactful.
Introduction
Palliative care is needed across many settings of care and for patients with cancer and non-cancer illnesses.1–4 This includes initiating a palliative care approach earlier in the illness trajectory and integrating it in chronic disease management.5 6 Achieving universal access requires a multipronged approach that incorporates appropriate policies, services, funding and education.7
All the palliative care needs of a population cannot be met by palliative care specialists alone.8 If equipped with core palliative care skills and supported by specialist palliative care teams, providers across many care settings and specialty areas can provide what is referred to as the palliative care approach.9 10 However, many healthcare professionals lack the competencies and confidence to provide this approach.11–13 This calls for palliative care education, including undergraduate and postgraduate training, and continuing professional development (CPD) for those already in practice.
Achieving widespread uptake of a palliative care education programme involves ‘spread’ (replicating an initiative elsewhere) and ‘scale-up’.14 The latter requires infrastructures, processes and policies to support full-scale, system-wide implementation and sustainability.
Pallium Canada (Pallium) is a non-profit organisation founded in 2000 to build primary palliative care capacity nationally across Canada. This paper discusses Pallium’s evolution and the national spread and scale-up of its education and compassionate communities programmes and the factors that have facilitated and impeded their spread and scale-up.
Pallium Canada’s geopolitical context, approach and evolution
Canada has a diverse and multicultural population of 37.2 million and an area that equals Europe. Most of the population lives in urban areas close to its southern border, but up to 16% of the population lives in rural and remote communities. Canada is a confederation of thirteen provinces and territories, each with responsibility over its own publicly funded healthcare system. This creates 13 different healthcare systems, with variability in terms of funding and the delivery of palliative care.
Pallium’s approach is guided by several tenets. First, patients with palliative care needs and their families are found across many care settings. Second, care is provided across these settings by providers from various professions and specialty areas. Third, palliative care requires an interprofessional and multidisciplinary approach that is promoted through interprofessional education.14 Lastly, palliative care requires a public health approach that includes engaging communities.7 15
Pallium positions itself as a Knowledge-to-Action broker and a health system change agent.16 It brings together palliative care subject matter experts from across the country to identify best practices and evidence and synthesise and spread them to health professionals via its interprofessional Learning Essential Approaches to Palliative Care (LEAP) courses and complementary materials.17 The LEAP courses address core palliative care competencies. While most are 1-day to 2-day classroom events with a maximum of 30 learners, flipped, hybrid and entirely online virtual versions are also available.
Pallium draws on Rogers’ diffusion of innovations model.18 Rogers posits that once a critical mass of innovators and early adopters—about 16% of the target audience—adopt a new approach, a tipping point is reached after which wider adoption accelerates.19
Pallium has evolved in phases.20 Activities and learnings from each phase have informed subsequent phases. The six phases from 2000 to date are summarised in online supplemental appendix A.
Supplemental material
Spread of Pallium Canada’s programmes and activities
The growth in number of LEAP course sessions delivered from 2001 to 2019 is shown in figure 1. In phase 1 (2001–2003), 17 LEAP courses were delivered, compared with 537 in 2019. The number of course sessions delivered from 2006 to 2014 was not tracked because of a decentralised distribution model with no course registration mechanism.

Number of Learning Essential Approaches to Palliative Care (LEAP) course sessions delivered across Canada from 2001 to 2019.
Prior to 2013, there was only one type (version) of the LEAP course, an interprofessional 2-day workshop for community-based primary care professionals. Since 2014, 1-day or 2-day versions have evolved or are being developed to target different settings and disease groups.17 These include versions for different settings (community, hospitals and long-term care (LTC)), services (paramedic services, emergency departments, paediatrics and healthcare leaders) and specific disease groups (cancer, renal, lung, heart and liver diseases).
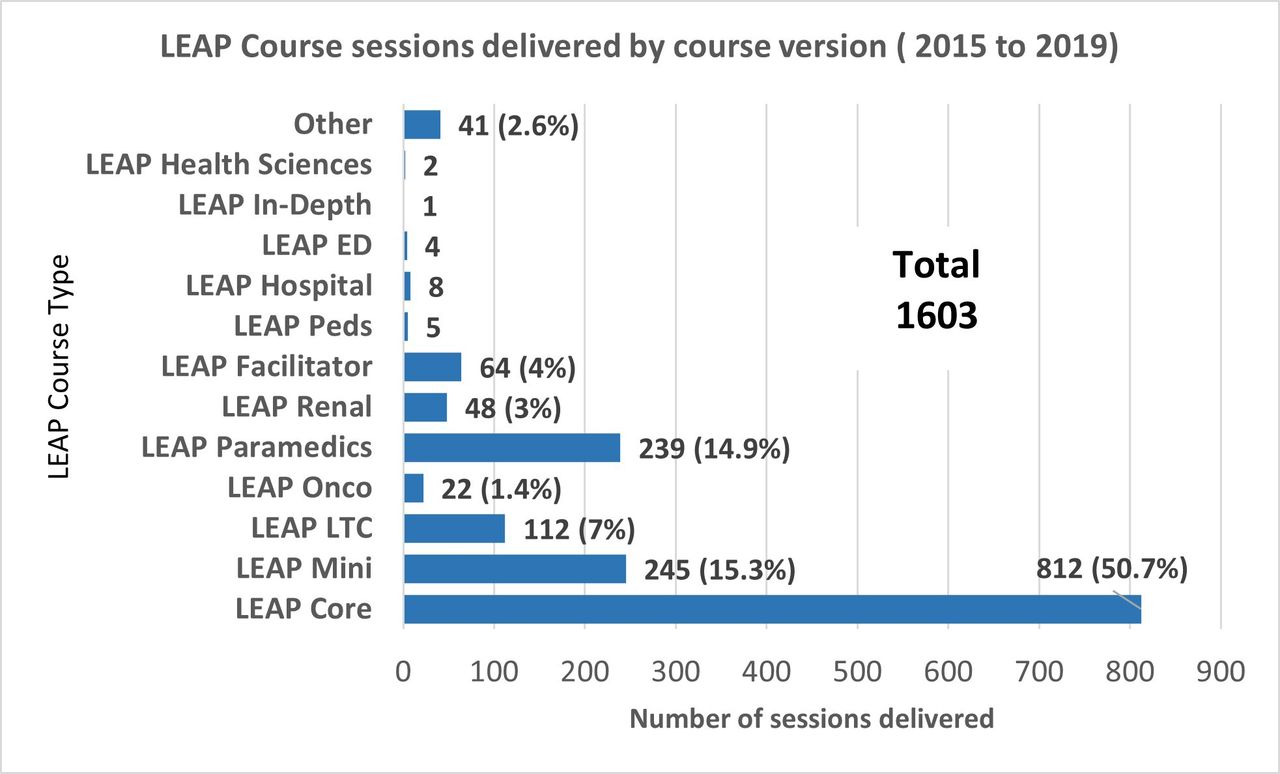
From 2015 to 2019, 1603 course sessions were delivered across Canada (figure 2). The course version most often delivered has been LEAP Core (50.7% of all sessions). To date, over 17 undergraduate and postgraduate programmes have adopted the courseware.

Learning Essential Approaches to Palliative Care (LEAP) course sessions delivered by course type from 2015 to 2019. ED, emergency department; LTC, long-term care; Onco, Oncology; Peds, paediatrics.
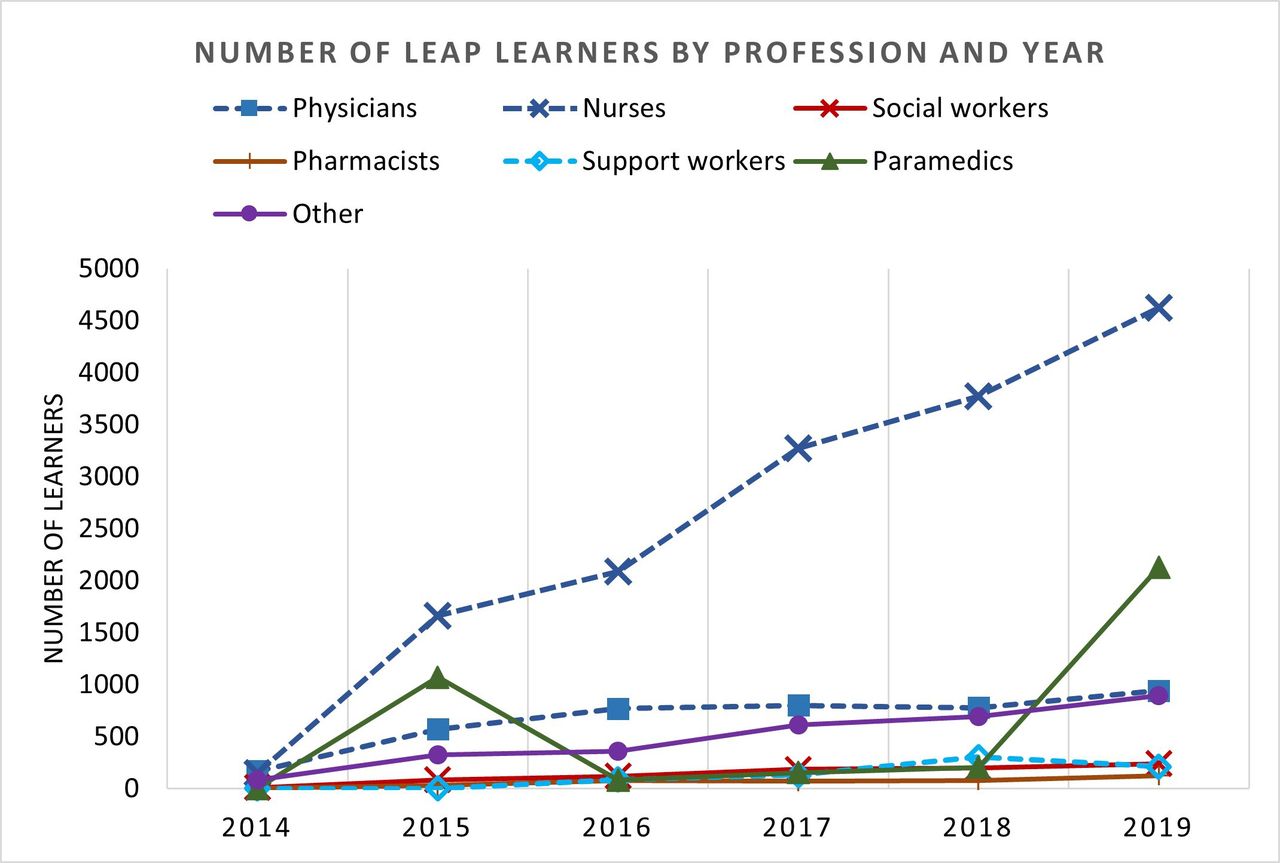
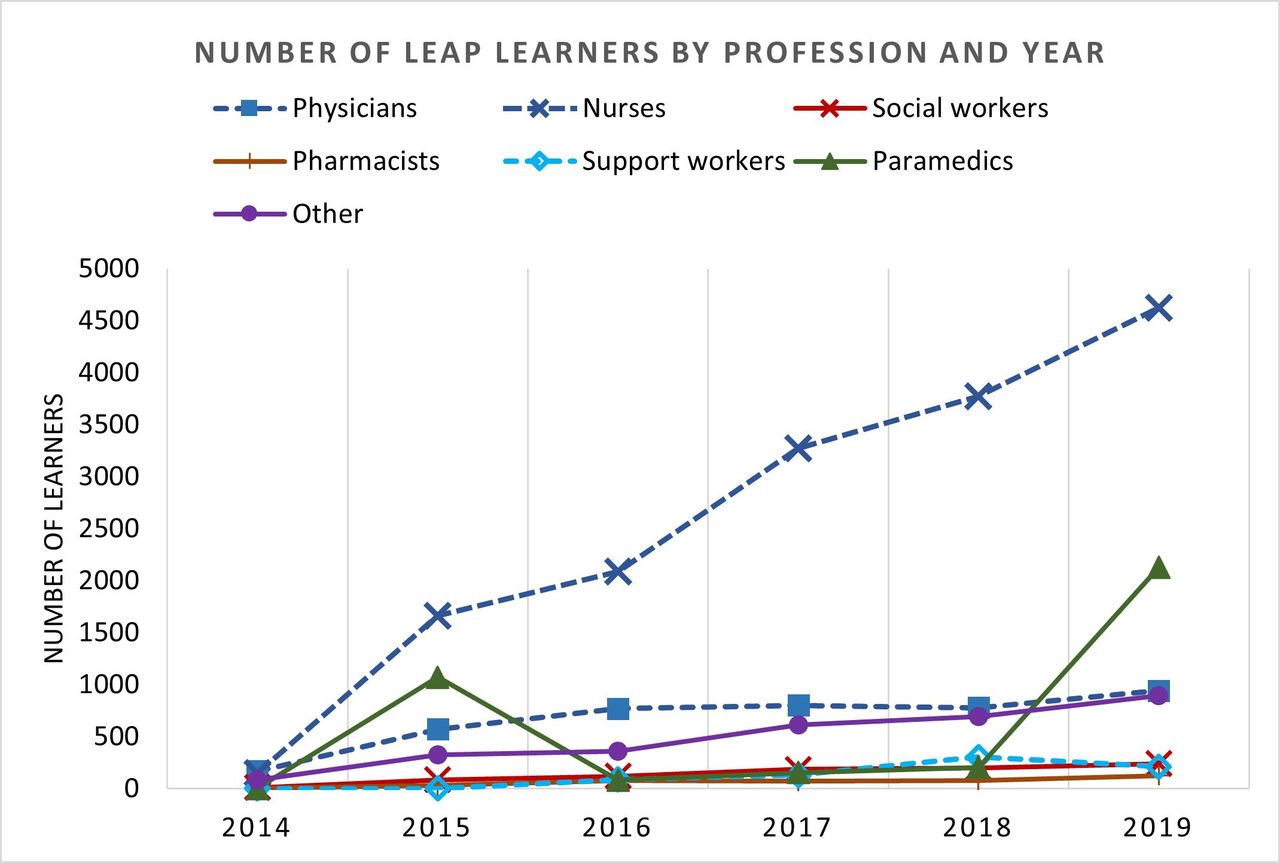
A total of 28 123 learners from different professions participated in LEAP courses from 2014 to 2019. Nurses make up the largest proportion of learners (15 560; 55.3%), followed by physicians (4023; 14.3%) and paramedics (3636; 12.9%). Social workers (835; 3%), pharmacists (380; 1.4%), support workers (730; 2.6%) and other professions (2959; 10.5%) have also participated. The latter includes physiotherapists, counsellors, dietitians, and clinical managers. The largest growth in terms of course participation has been with nurses (figure 3). Physician numbers, and those of the other professions, have seen more gradual increases.
{kind=link}
{kind=link}
{kind=link}
Number of Learning Essential Approaches to Palliative Care (LEAP) learners by year and profession (June 2014 to Dec 2019).
The geographical spread of the 537 LEAP course sessions delivered in 2019 is shown in online supplemental appendix B. Their distribution reflects Canada’s population distribution and includes large and small urban centres and rural and remote communities.
Supplemental material
In March 2020, in response to the COVID-19 pandemic, Pallium opened its suite of online self-learning modules for free access over 6 months; 11 672 healthcare professionals and students registered. In April 2020, Pallium launched a fully online version of its LEAP Core course, which complements the self-learning modules with live interprofessional, case-based webinars. As of February 2021, 103 courses were delivered to 1979 participants. Pallium also hosted a series of national webinars to address emergent pandemic-related topics. From April 2020 to February 2021, 25 webinars were delivered in English and French, with an average of 288 registrants per webinar (available at www.pallium.ca). The two with the most attendees were webinars in April 2020 on providing virtual palliative care and the dealing with the psychological impact of the pandemic on palliative care providers with 703 and 592 participants from across Canada and internationally respectively.
From 2001 to 2005, community town hall get-togethers on palliative and end-of-life care were organised to engage communities where LEAP course sessions were delivered. Our Compassionate Communities (CC) advocacy work was reactivated in 2015 with a national symposium and the development of a CC start-up toolkit in 2018 and online community of practice. From June 2018 to December 2020, Pallium’s CC start-up toolkit, which provides communities with information and links to useful resources, has been downloaded 3263 times (English and French versions) across all Canadian provinces and internationally.
Factors that have facilitated or impeded spread and scale-up
Success factors and spread accelerators
The factors that have contributed to the spread and scale-up of Pallium and its initiatives warrant discussion as some lessons learnt may be transferrable to other jurisdictions. The key factors are listed in box 1.
Factors that have facilitated spread and scale-up of Pallium Canada’s programmes
Products
Standardised, ready-to-use, competency-based courseware
Personnel and infrastructure
Large national multiprofessional community of practice
Interdisciplinary staff
Information technology ecosystem
Approaches and strategies
Train-the-Trainer model, facilitator programme and large facilitator pool
Curriculum development framework for large-scale development and deployment of multiple courses for different settings and disease groups
Strategic partnerships
Centralised course development but decentralised delivery
Continuous quality control and improvement and data-informed
Responsiveness, flexibility and adaptability while retaining clarity of mission…agility
Customer support programme
Persistent advocacy and resilience
A social enterprise model for self-reliance and sustainability
Governance and funding
Non-profit foundation with board of directors of community leaders
Social enterprise approach
Pallium has used a ‘3C’ approach: coordinating, collaborating and communicating across jurisdictions to maximise know-how and resources. The 3C approach involves bringing together educators, clinicians and stakeholders from across regions and provinces to work together and to leverage expertise and best practices with the goal of codeveloping high-quality standardised curricula. This has created an extensive national community of practice and network including clinicians, educators, policymakers, leaders and community champions. The collective expertise has promoted knowledge sharing and reduced duplication of effort.
The availability of standardised, credible, high-quality courseware has provided educators, who are often busy clinicians with few resources and time, with ready-made courseware. Many palliative care providers, particularly in rural regions, do not have academic affiliations and access to academic resources. The courseware helps them stay current with best practices and evidence. Online supplemental appendix C provides a summary of the courses, their instructional designs and examples of the course programmes. A full description of the courses and their design elements is provided elsewhere.17 21
Supplemental material
The curriculum development framework provides an economy of scale that accelerates the development of course versions.17 It does this by leveraging existing courseware to develop new courses for different settings and disease groups, thereby promoting common messages and approaches across care settings. Courseware credibility and quality are promoted through a quality-assurance process that includes extensive peer reviewing and periodic updates.
A multifaceted information technology (IT) ecosystem with several interconnected software platforms has accelerated operational efficiencies and spread. This ecosystem includes a customised learning management system built with the open-source programme Moodle. It serves to distribute course materials, register courses and learners easily, collect precourse and postcourse data, deliver the online course versions or modules and manage course and facilitator evaluations. Financial programmes support registration-fee processing. Recent enhancements have included business intelligence software programmes that improve real-time data analysis and reporting and client support and management. The data in turn inform quality improvement and growth strategies. Facilitator feedback and the ability to push custom communications and announcements to different user groups have been boosted.
Strategic partnerships have been critical and have required sustained and deliberate efforts at all levels of government and service delivery. At local and regional levels, these have included hospitals, home care agencies, family health clinics, paramedic services, universities and colleges. Provincial partners have included palliative care associations, provincial service agencies and government ministries, while at a national level, these have included national organisations, professional societies and the federal health ministry. The successes of the paramedics programme prompted two national healthcare improvement organisations to fund spread across several other provinces.22
A decentralised course organisation and delivery approach have aided spread. A centralised distribution model was initially used (2001–2005); course sessions were organised by Pallium’s office and facilitators deployed to course venues. In 2006, a decentralised model was introduced in which LEAP courseware was made available for purchase using an end-user licensing model. Once purchased, educators could use the material as often as they wished; no registration fees were charged by Pallium, although course providers were able to charge a fee to cover costs.
Although this approach facilitated spread from 2006 to 2013, it had drawbacks. The quality of the courseware and the learning experience were compromised as some educators failed to apply optimal facilitation practices while others made unapproved modifications to the courses, bypassing peer review and other quality-assurance processes. It also significantly reduced revenue, challenging Pallium’s sustainability when government funding ended from 2008 to 2013.
The model was therefore modified in 2014. Courseware development and maintenance are now centralised (coordinated by Pallium’s office), but courses are organised by local or provincial groups and presented by local facilitators. All courses and learners are registered online, at which time course registration fees are collected. A portion of the fee is retained by Pallium and the remainder distributed to the organising group to cover expenses.
The large pool of over 900 trained and certified LEAP facilitators across the country is a key success factor. This has required intentional design, including a structured Train-the-Trainer Programme, facilitator support and facilitator criteria. Facilitators are required to be palliative care clinicians (doctors, nurses, social workers and pharmacists) with advanced palliative care training and experience. They also need to demonstrate ongoing facilitation proficiency as assessed by learner evaluations.
Registration of Pallium as a non-profit foundation with a board of directors made up of community leaders has promoted governance, transparency and accountability.
The main source of funding over the years has been from federal government through project contribution agreements, totalling $13.5 million over 20 years. This funding has been key to start the project, develop the courses and courseware, spread them across the country and implement the IT ecosystem. Some funding ($1.2 million) has also been received from philanthropic sources. Funding from the Canadian Medical Association and an unrestricted education grant from an industry partner have supported virtual programming during the COVID-19 pandemic.
A social enterprise model that involves diversifying sources of revenue to augment government funding has therefore evolved to support self-sufficiency and long-term viability. Reliance solely on government funding has become too tenuous for long-term sustainability.
Approaching scale and spread-up across three health system levels—namely, micro, meso and macro—has proven strategically useful. Micro here refers to small or local teams or services such as a family health clinic or hospital ward or service, while meso refers to a whole hospital, cancer centre or nursing home. Macro-level spread, on the other hand, is exemplified by dissemination of a course across a whole province or the country. See table 1 for examples of spread at these various levels. Multiple successes at a micro level within a province or region have helped reach meso or micro levels. However, in some cases, spread started at meso or even a macro levels, depending on the opportunity or partnership.
Examples of spread of Pallium Canada’s programmes across micro, meso and macro levels
Sustainability and spread have required resilience, patience, sustained advocacy, flexibility and agility to leverage new opportunities and emerging needs, without detracting from the mission. Customisation for special situations and needs is periodically required. For example, LEAP courses were rapidly transformed for full-online delivery in response to the COVID-19 pandemic.
Challenges and barriers
Several factors have impeded spread and scale-up including the need to engage 13 different healthcare systems and their multiple subregions individually.
While funding has made the project possible, the lack of sustained funding, proportionate to the need at hand, has been challenging. Reaching the ‘tipping point’ in terms of workforce training has, with some exceptions, been elusive in many regions; on average, less than 5% of the Canadian healthcare workforce has been trained. On a meso level, the tipping point has been reached in some provinces with paramedic and home care training and on a micro level in services and clinics that have trained all their staff. Support by local and provincial healthcare service leaders and policymakers, who actively integrated palliative care education in their respective portfolios, has been a common success factor in all these cases.
Provincial and government funding remains critical. There are some activities that do not generate revenues, including developing and testing programmes directed at undergraduate and postgraduate education, compassionate communities, indigenous populations, refugees, vulnerably housed persons and rural and remote communities. Moreover, publicly funded organisations such as hospitals, home care services and LTC homes face ongoing financial constraints, reducing their ability to pay for large-scale training. Universities and colleges face similar challenges.
While change science learnings have been applied in Pallium’s spread and scale-up efforts,23 we have underestimated some insights. Moore, for example, argues that a messaging chasm exists at the tipping point, necessitating a change in strategy.24 Because the motives for adoption are different between the early adopters and the early majority, the messaging should change from ‘adopt and be a leader’ to ‘adopt and join the others’ at that critical juncture.
A culture that prevails in many universities that rewards new innovations over supporting spread and research of existing ones is another challenge. As Downar, with respect to palliative care education in Canada, explains, ‘a more efficient system would be to have one or two standardised curricula; this would allow academic physicians to put their efforts towards broad dissemination rather than duplication’.25 Moreover, fundraising is a necessity for many Canadian palliative care and hospice organisations, leading some to duplicate educational initiatives to generate revenue.
Programme evaluation and impact
In phase 2 (2003 to 2007), a multifaceted framework was used, drawing on Health Canada’s Participatory Evaluation Framework and Kirkpatrick’s Evaluation Model.24 The evaluation results are described elsewhere.26 27
The LEAP courseware evaluations have largely focused on Kirkpatrick’s levels 1 and 2 (learners’ experiences and changes in knowledge, attitudes and comfort). These have demonstrated positive learner and facilitator experiences and improvements in knowledge, attitudes and comfort levels across different professions and postgraduate learners.22 27–29 The largest study to date involved almost 7000 professionals who participated in LEAP courses from April 2015 to March 2017.30
Evidence of impact at level 3 (patient care) and level 4 (health system impact) was noted in the 2007 evaluation and continues to emerge. In the 2015–2017 study, analyses of the 4-month postcourse commitment-to-change reflections submitted by learners provide signals and examples that learners are implementing what they learnt.31 Evaluations of the INTEGRATE Project, a multipronged intervention that included training of staff at cancer centre programmes and family health clinics with LEAP courses, found improved earlier identification of patients with palliative care needs, increased use of palliative care services and improved professionals’ skills.29 32 In an evaluation of the ‘Paramedics Palliative Care’ Project in two provinces, in which LEAP Paramedic training was applied alongside policy and procedure changes, patients and families reported high degrees of satisfaction, particularly being able to be cared for at home.22 Paramedics reported increased comfort, confidence and joy providing palliative care, while patients and families reported better symptom control, quality of life and gratitude for being cared for in their homes. A return of investment assessment found net savings of $C2.5 million over an 18-month period; savings were largely attributed to avoided hospital transfers and reduced time spent by paramedics per patient.33
International context
Large national CPD-level programmes targeting primary-level or generalist-level palliative care skills exist in other countries.34–36 Each initiative has its respective strengths, limitations and challenges. Some similarities exist across the initiatives. The large geographical area covered, attention to Canadian geopolitical realities, the promotion of interprofessional learning, the availability of multiple course versions for different settings of care and diseases and a unique IT ecosystem are stand-out features of Pallium’s approach.
Future directions
Strategic partnerships with local, regional, provincial and federal partners and stakeholders will be critical in ongoing efforts to build primary palliative care capacity across different settings and professions and to foster compassionate communities. The structures and processes put in place, including the IT ecosystem and curricula development approaches, will allow more customisation of the products to address local, jurisdictional and specific professions’ needs. The respective roles of the various delivery methods, including their strengths and limitations, need to be better understood. While classroom learning will return post COVID-19 pandemic, virtual learning will likely be more widespread, through flipped or entirely online learning approaches.
The LEAP courses will continue to be updated periodically based on ongoing learner and facilitator input and emerging evidence and best practices. Minor modifications are made annually, while each course undergoes a major overhaul every 3–4 years. A full description of the instructional design considerations and decisions of the LEAP courses, as well as future design modifications being planned, is provided elsewhere.21 To enhance interprofessional learning and increase efficiencies in this area, for example, Pallium Canada will develop self-learning online modules that are profession-specific or highlight the roles and contributions of various professions. This will allow learners to learn and acquire knowledge and concepts that are relevant to their professions or help them understand and value the contributions of other professions and then come together for live interprofessional learning in classroom or webinar sessions.
Additional strategies such as linking CPD with quality improvement in the workplace could enhance integration of the approach into daily practice.37 38 Finally, Pallium should incorporate emerging evaluation frameworks that help understand multipronged interventions within complex systems.39 40
Conclusion
Pallium Canada provides a case study on developing primary-level palliative care at a national level. It has developed infrastructure, processes, products, strategies and tools to advance the palliative care approach across different care settings, professions and communities. It has also championed interprofessional learning and the development of compassionate communities across Canada.
The work to date, while impactful at local and some provincial levels, still requires considerable spread and scale-up efforts if primary-level palliative care is to be fully integrated in the healthcare system. Education, while necessary, is alone insufficient. Multipronged approaches that combine education of healthcare professionals and the community, with other strategies such as policies, processes, funding and resources, are required. Linking education with quality improvement approaches holds potential.
Spread and scale-up of primary-level palliative care necessitate collaboration with local, provincial and federal governments and organisations. A social enterprise model that involves diversifying sources of revenue to augment government funding is evolving to support self-sufficiency and long-term viability. Some of the lessons learnt over Pallium’s twenty years may be transferrable to other jurisdictions engaged in, or considering, similar national education initiatives.
Ethics statements
Acknowledgments
Pallium Canada acknowledges and thanks the countless individuals and organisations for their contributions over the years to Pallium’s work. Pallium Canada is indebted to the LEAP facilitators across the country. Thank you to the current and past Pallium Canada Foundation board of directors and past leads. A very special thank you to all the past and present staff team members at Pallium Canada who have contributed to this work. Thank you to Dr Lamia Hayawi and Tammy Tsang for helping prepare the manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @jeffmoat
Presented at J Pereira. (Plenary). Building Primary-Level Palliative Care Capacity Through Education across Canada: The Pallium Canada Experience. 15th World Congress of the European Palliative Care Association. Madrid, Spain, 18 May 2017.
Contributors JP is the cofounder of Pallium Canada and has provided leadership as scientific lead and officer since its inception. This has included input on programme design, development, evaluation and deployment. JBM and JF have provided programme coleadership for the last three years and have contributed significantly to its operations, development and recent scale-up and spread, including its IT infrastructure and the development of the social enterprise model. SC has served as coclinical lead of the programme since 2007, is a member of the programme’s board of directors since 2010 and has provided input on various aspects of the programme’s deployment. BT has led the implementation and spread of Pallium’s compassionate communities initiatives. All authors contributed to this work, prepared this manuscript and approved the final draft.
Funding Pallium Canada is registered in Canada as a non-profit, charitable organisation. It has been funded mainly by contributions from Health Canada (the Canadian Federal Ministry of Health), through course registration fees and more recently through unrestricted grants from the Li Ka Shing Foundation, the Canadian Medical Association and Boehringer Ingelheim (the latter to support COVID-19 webinars that are referred to in this paper). From 2013 to 2016, this was enhanced by funding from a private benefactor, the estate of Mr Patrick Gillin of Ottawa, Canada. Smaller levels of funding have been received from some provincial government ministries to support provincial-level work, including the Ontario Renal Network, Cancer Care Ontario and the Government of New Brunswick. Supplementary revenues have come from Pallium Canada’s Palliative Pocketbook and from various organisations and service providers who have adopted the LEAP Programme to train their workforce.
Competing interests JLP (scientific officer), JF (vice president of operations) and JBM (CEO, Pallium) are all paid staff members of Pallium Canada. The other authors have, over the years, received stipends by Pallium Canada for their curriculum development and delivery contributions.
Provenance and peer review Not commissioned; externally peer reviewed.