Article Text

Abstract
Objective To investigate patterns of care during the last months of life of hospitalised patients who died from different haematological malignancies.
Methods Nationwide register-based study, including all hospitalised adults ≥20 years who died from haematological malignancies in France in 2010–2013. Outcomes included use of invasive cancer treatments and referral to palliative care. Percentages are adjusted for sex and age using direct standardisation.
Results Of 46 629 inpatients who died with haematological malignancies, 24.5% received chemotherapy during the last month before death, 48.5% received blood transfusion, 12.3% were under invasive ventilation and 18.1% died in intensive care units. We found important variations between haematological malignancies. The use of chemotherapy during the last month of life varied from 8.6% among patients with chronic myeloid leukaemia up to 30.1% among those with non-Hodgkin’s lymphoma (P<0.001). Invasive ventilation was used in 10.2% of patients with acute leukaemia but in 19.0% of patients with Hodgkin’s lymphoma (P<0.001). Palliative status was reported 30 days before death in only 14.8% of patients, and at time of death in 46.9% of cases. Overall, 5.5% of haematology patients died in palliative care units.
Conclusion A high proportion of patients who died from haematological malignancies receive specific treatments near the end of life. There is a need for a better and earlier integration of the palliative care approach in the standard practice of haematology. However, substantial variation according to the type of haematological malignancy suggests that the patients should not be considered as one homogeneous group. Implementation of palliative care should account for differences across haematological malignancies.
- end-of-life care
- hematologic neoplasms
- intensive care
- palliative care
Statistics from Altmetric.com
Introduction
The treatment of haematological malignancies has made considerable progress during the last two decades.1 2 Novel targeted therapies and enhanced haematopoietic stem cell transplantation procedures have significantly improved survival in patients with lymphoma, multiple myeloma and acute leukaemia.3 However, haematological malignancies remain incurable in most situations and are still associated with high mortality.4
The palliative care needs of patients with advanced haematological malignancies have been widely acknowledged.5 6 Decision-making and communication between physicians and patients also become more complex as the disease is progressing.7 Addressing the need for palliative and supportive care of patients with haematological malignancies could improve their quality of life and the quality of care received near the end of life.8 Yet, patients with haematological malignancies have been found to be less frequently referred to palliative care services and to receive more aggressive treatments near the end of life than patients with solid tumours.9–11 Some authors have however questioned the relevance and applicability of the quality criteria developed in the field of solid oncology for patients with haematological malignancies.12–15 These patients may indeed present specific needs that could require other standards to assess the quality of end-of-life care. Furthermore, most studies investigating the aggressiveness of end-of-life care considered solid tumours separately (ie, distinguishing between different location of histological types) but reported haematological malignancies as one homogeneous group of diseases even though haematological malignancies encompass a wide range of clinically different situations.10
This study aimed to compare the patterns of care over the course of the last 3 months of life of hospitalised patients who died from different haematological malignancies. We hypothesised that the provision of specific treatments and that the use of palliative care facilities varied significantly from one haematological malignancy to another.
Methods
Study design and population
Nationwide, mortality follow-back cohort using data from the French national hospital register. This register collects administrative and medical information for all inpatient admissions and outpatient visits in France. Diagnoses are coded according to the International Classification of Diseases, 10th revision (ICD-10). All hospitalised adults (≥20 years) who died from haematological malignancies (ICD-10 codes C81 to C95 and D46) in France between 1 January 2010 and 31 December 2013 were included. Patients were excluded from the study population if they had a concomitant solid malignancy, or had overlapping or unspecified haematological malignancies.
Care outcomes
Hospital admissions
Mean number of hospital admissions, mean number of days of hospitalisation, frequency of intensive care unit (ICU) admissions, proportion of patients who remained hospitalised continuously and number of emergency department (ED) visits were calculated for the 3-month period before death. We also examined the origin of the last hospital admission before death and the final place of death of haematology patients.
Medical interventions
We primarily investigated the administration of chemotherapy delivered in hospital (intravenously or orally), blood transfusion, invasive ventilation and haemodynamic support (ie, use of dopamine, dobutamine, dopexamine, epinephrine, norepinephrine or intravenous volume expander) within the last 3 months, 1 month and 2 weeks before death. We also reported five secondary outcomes: use of radiation therapy, artificial nutritional support (regardless of the route of administration), cardiopulmonary resuscitation, tracheal intubation and dialysis by either haemodialysis, peritoneal dialysis, hemofiltration or haemodiafiltration. These medical interventions were captured if they were performed during a hospitalisation, an outpatient visit or via a hospital-at-home service. Care outcomes were chosen based on previously published studies.16 17
Reporting of palliative status and palliative care referral
We first examined the reporting of the palliative status of patients during the last 3 months of life. This was defined as the period of time when the ICD-10 code Z51.5 ‘palliative care’ was first mentioned in the patients’ medical records (as either principal or associated diagnosis). In France, this diagnosis code is used to indicate the need for care and treatments directly related to the palliative nature of an advanced and potentially life-threatening health condition. Reporting of this diagnosis is required for activity-based payment of palliative care, and increases the value of diagnosis-related groups (DRG) used by the National Health Insurance to calculate the reimbursement of hospital stays. It is also used for enabling the patients to access certain community-based services. Therefore, the coding of palliative status is expected to be of high quality near the end of life. Second, we investigated the referral to palliative care inpatient units (ie, inpatient units entirely dedicated to the practice of specialist palliative care) or palliative care support beds (ie, beds typically grouped in two-bed to four-bed clusters and embedded in hospital departments whose medical specialty leads to caring for seriously ill patients).18 Referral to specialist palliative care was identified in hospital discharge reports, using both diagnosis-related groups and identification of medical units. Details are available from the authors on request.
Definition of covariates
Sex, age (categorised into 10-year groups in order to maintain anonymity) and number of other chronic conditions (derived from the list of chronic diseases included in the Charlson Comorbidity Index,19 and computed from inpatient diagnoses in the last 3 months of life) were extracted from the hospital register. Haematological conditions were categorised into ‘acute leukaemia’, ‘chronic lymphoid leukaemia’, ‘chronic myeloid leukaemia’, ‘Hodgkin’s lymphoma’, ‘multiple myeloma’, ‘myelodysplastic syndromes’ and ‘non-Hodgkin’s lymphoma’. Details about the corresponding ICD-10 codes are available in online supplementary table A1.
Supplementary file 1
Statistical analysis
Care outcomes of patients with different haematological malignancies were standardised for both sex and age, using direct standardisation method with the total population as reference. This allowed for removing the confounding effect of sex and age. Differences were tested with Pearson’s Χ2 test, Student’s t-test and Wilcoxon rank sum test when appropriate (two-sided P, with P<0.001). Multivariable logistic regression analyses were also performed to investigate the association between the type of haematological malignancy and the receipt of specific treatments while adjusting for sex, age, number of other chronic conditions and category of hospital were death occurred. Adjusted ORs were reported with their 95% CI. All statistical analyses were performed using SAS JMP V.12.1.0 (SAS Institute).
Results
Patients characteristics
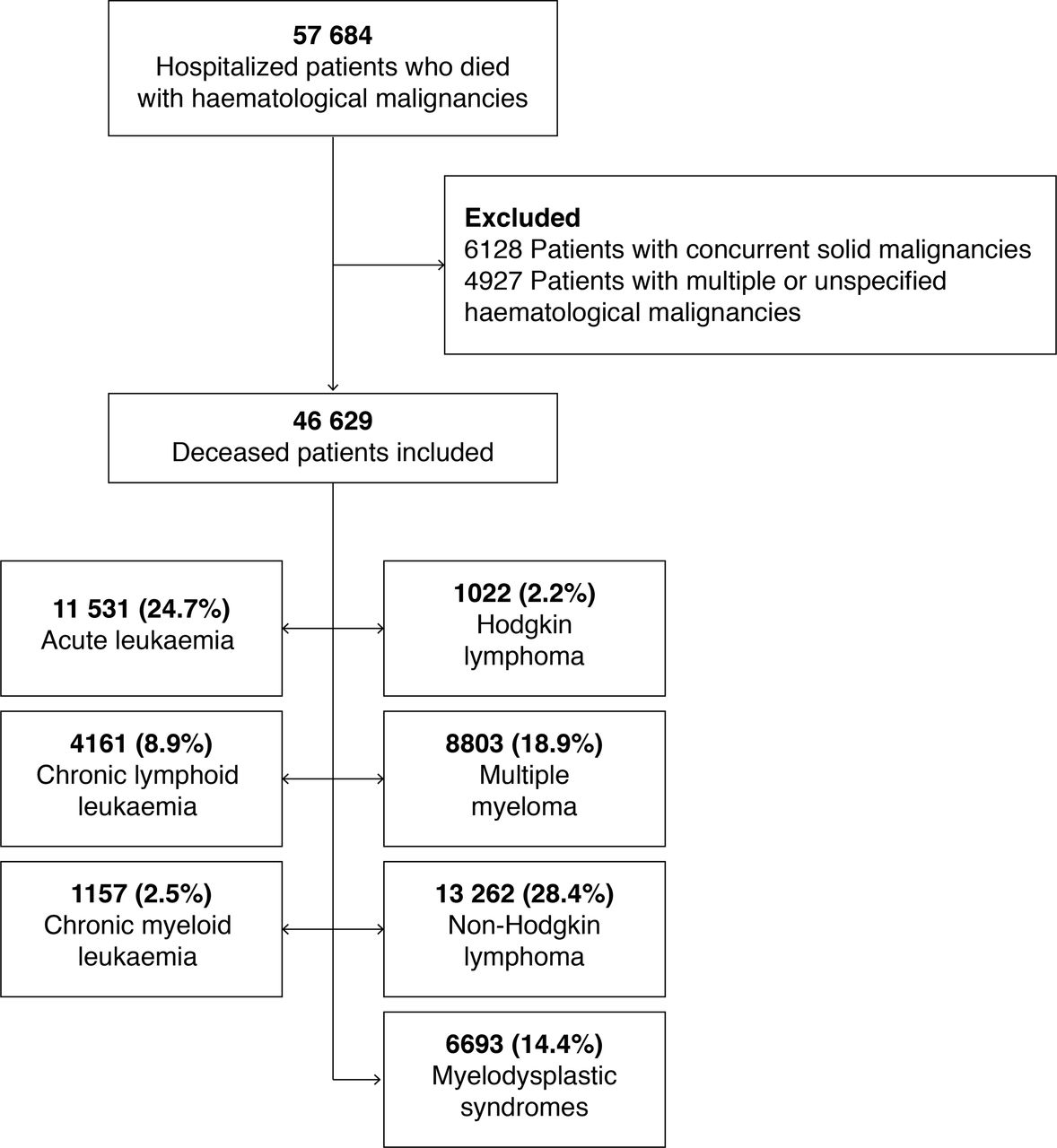
A total of 46 629 patients with haematological malignancies who died in hospitals between 2010 and 2013 met our inclusion criteria (figure 1). Most patients suffered from non-Hodgkin’s lymphoma (28.4%), acute leukaemia (24.7%) or multiple myeloma (18.9%). Overall, 74.3% of individuals were aged ≥70 years at time of death. This proportion, however, ranged from 50.5% in patients with Hodgkin’s lymphoma to 90.4% in those with myelodysplastic syndromes (table 1). Overall, 79.5% of patients died in public hospitals (including 28% in university hospitals), and 3.4% died in comprehensive cancer centres. The proportion of patients who had no other reported chronic condition varied from 24.0% in patients with myelodysplastic syndromes to 52.0% in those with acute leukaemia, with an average number of comorbidities ranging from 1.5 to 0.7, respectively (mean difference=−0.72, 95% CI −0.75 to −0.69). The most prevalent conditions were heart failure (25.8%), renal failure (16.2%) and diabetes (15.6%). Detailed information regarding the prevalence of comorbidities according to the type of haematological malignancy is available in online supplementary appendix table A2.

{kind=link}
Selection of study population flow chart.
Characteristic of hospitalised patients with haematological malignancies who died between 2010 and 2013 in France
Hospitalisations in the last 3 months of life
During the last 3 months before death, patients had on average 2.1 hospitalisations (SD=1.6), and were hospitalised for 34.9 days (SD=25.5). Overall, 3.2% of all 46 629 patients remained hospitalised continuously. As shown in table 2, this proportion varied from 1.8% of patients with acute leukaemia to 5.2% of patients with chronic myeloid leukaemia. Moreover, 58.4% (n=27 231/46 629) of patients had at least one ED visit. While adjusting for possible confounders, patients with myelodysplastic syndromes were more likely to have multiple ED visits than patients with Hodgkin’s lymphoma (OR 1.45, 95% CI 1.19 to 1.78), multiple myeloma (OR 1.40, 95% CI 1.29 to 1.53) or non-Hodgkin’s lymphoma (OR 1.39, 95% CI 1.28 to 1.51). The place of death also varied according to the type of haematological malignancy (table 2). Compared with patients with acute leukaemia, those with Hodgkin’s lymphoma were more likely to have died in intensive care units (OR 1.85, 95% CI 1.59 to 2.15), and less likely to have died in palliative care units (OR 0.61; 95% CI 0.42 to 0.85).
Hospital admissions and use of hospital resources in the last 3 months before death of patients with different haematological malignancies
Treatment use over the course of the last 3 months of life
Overall, out of a total of 46 629 inpatients, 17 655 (37.9%) received chemotherapy over the course of the last 3 months before death, 26 701 (57.3%) received blood transfusion, 5970 (12.8%) received invasive ventilation and 7053 (15.1%) received haemodynamic support. We found considerable variation in the use of these treatments, both over time and between haematological malignancies (see online supplementary appendix figure A1 and table A3 and Table A3). During the last month before death, the use of chemotherapy varied from 8.6% of patients with chronic myeloid leukaemia to 30.1% of patients with non-Hodgkin’s lymphoma, while the use of invasive ventilation varied from 10.2% of patients with acute leukaemia to 19.0% of patients with Hodgkin’s lymphoma (table 3). Likewise, although 41.7% of all patients received blood transfusion within the last 2 weeks before death, this proportion ranged from 28.3% of patients with non-Hodgkin’s lymphoma to 59% of patients with acute leukaemia (P<0.001). These variations remained while adjusting for potential confounders (table 4). Although less frequent, artificial nutrition, tracheotomy and dialysis were still common during the last month of life.
Frequency of treatment use in hospitalised patients with different haematological malignancies
Adjusted likelihood for hospitalised patients with different haematological malignancies to receive specific treatments during the last month before death
Palliative care referral to in the last 3 months of life
The reporting of palliative status gradually increased over the last 3 months before death, from 14.8% of patients 30 days before death to 46.9% at time of death. However, 53.1% of patients died without any reporting of their palliative status. This proportion was especially high for patients with myelodysplastic syndromes, chronic lymphoid leukaemia and chronic myeloid leukaemia (64.4%, 63.5% and 61.4%, respectively). Also, 6% of patients were admitted in palliative care units during their last 3 months of life, and 5.5% eventually died in palliative care units. We found only little variation according to the type of haematological malignancy (table 5), but considerable discrepancies across hospital facilities. The proportion of deaths occurring in palliative care units ranged from 0% in comprehensive cancer centres (0/1559) to 32.5% (728/1502) in private-not-for-profit clinics.
Referral to palliative care services in the last 3 months of life of hospitalised patients with different haematological malignancies
Discussion
Our study shows high rates of treatment use in the last months of life of hospitalised patients with haematological malignancies. Overall, 25% of decedents received chemotherapy during the last month before death, 48% received blood transfusion, 12% had invasive ventilation and 18% died in ICUs. Furthermore, the use of invasive ventilation and haemodynamic support increased steadily during the last 3 months of life.
Patients with Hodgkin’s lymphoma or acute leukaemia died younger and had less comorbidities than patients with other haematological malignancies. These patients were also more likely to die in tertiary hospitals than patients who died from chronic lymphoid leukaemia or myelodysplastic syndromes. This may be due to the necessity for patients with Hodgkin’s disease or acute leukaemia to have access to highly specialised physicians and treatments. In addition, the overall prevalence of chemotherapy administration during the last month before death varied from <10% in patients with chronic myeloid leukaemia or myelodysplastic syndromes up to 30% in patients who died from non-Hodgkin’s lymphoma. Clinical factors most likely explain a large share of this variation: haematological malignancies have different levels of chemosensitivity, are more or less likely to induce severe cytopenia, have different prognoses and shape different end-of-life trajectories in terms of functional decline and psychological distress. In our opinion, these variations could also explain the considerable heterogeneity in the findings reported in previous studies, with rates of chemotherapy use in the last month of life ranging from 14% to 43%.9 20
Studies investigating ICU admission of haematology patients also showed contrasted results, with 19%–33% of patients dying in ICU.21 Our results show important variations between the different haematological malignancies (from 15% to 27%), thus suggesting disease-specific patterns of ICU referral near the end of life. For instance, it could be hypothesised that because of their higher survival rates, patients with Hodgkin’s lymphoma or chronic myeloid leukaemia were more likely to benefit from ICU care than patients with other haematological malignancies. However, these high rates of patients who died in ICU are a matter of concern, given that patients who die in ICU often experience greater physical and emotional distress and worse quality of life than patients who die at home with hospice care, and that their caregivers may have a higher risk of prolonged grief.22 Decisions to transfer patients with advanced haematological malignancies to ICUs should therefore be anticipated and carefully examined.23 24
Blood transfusion near the end of life is a critical issue in haematology, and is frequently continued close to death even in palliative care services.25 Classifying it as an ‘aggressive’ treatment is debatable. Because bone marrow failure is frequent in haematological malignancies, blood transfusion represents an early life-supporting intervention, often associated with brisk clinical improvement. At the end of life, these treatments might have been considered as a tool to improve the quality of life.26 27 On the other hand, blood transfusion may hinder death at home or in hospice, and contribute to prolong patients’ lives beyond their wish.28 29 Thus, the decision to continue or discontinue blood transfusion near the end of life should take into account both the patient’s needs in terms of comfort, the effectiveness of such treatments and the existence of other possible alternatives.30
Palliative status of patients remained unreported for more than half of individuals who died from haematological malignancies, and was often reported late during the course of the disease: only 14.8% of patients had a palliative status identified 1 month before death. Surprisingly, patients with myelodysplastic syndromes and chronic lymphoid leukaemia— whose goals of care are mostly palliative—were the least likely to have a palliative status reported in their electronic medical records. This is consistent with recent findings from Odejide et al, who suggested a less frequent use of hospice among patients who died from indolent lymphomas compared with those who died from aggressive lymphomas.10 Other studies have highlighted variations in palliative care referrals depending on the type of haematological malignancy, with heterogeneous results.31 32 In France, 130 palliative care inpatient units are specifically dedicated to patients whose clinical, psychosocial and ethical situation are the most complex. Given the high physical and psychological burden of patients dying from haematological malignancies, the low rate of palliative care unit referral is unexpected and raises concern. Palliative care referral has indeed been found to be associated with a decreased aggressiveness of end-of-life care and with an increased quality of life and satisfaction with care.33 34 Our results are however consistent with previous studies, showing that referral to specialist palliative care services for haematology patients remains rare and late in the disease trajectory.35 Despite the unavoidable uncertainty attached to the prediction of the remaining life-expectancy, overall survival in refractory haematological malignancies rarely exceeds a few months. For these patients, palliative care referral should therefore occur even when further active treatments are considered.36
Several factors are likely to contribute to the aggressiveness of end-of-life care, including the overoptimism induced by the myriad of treatment options, the unpredictable trajectory of advanced haematological malignancies and the sense of failure often perceived by haematologists facing refractory diseases.37 38 These factors tend to meet patients’ need for hope as well as—in many instances—their desire for a passive role in the decision-making.39 Qualitative studies have described this phenomenon of patients and physicians mutually reinforcing attitudes of ‘not giving up’.7 40 The insufficient integration of a palliative care approach in the standard practice of haematology and the lack of timely end-of-life discussions with patients are also a major issue for improving quality of end-of-life care for patients dying from haematological malignancies.6 41 42
On the other hand, healthcare providers should better integrate the needs of haematology patients in the delivery of specialist and generalist palliative care. The various outcomes developed to assess the quality of end-of-life care in patients dying from solid cancer can not be transposed de facto to patients dying from haematological malignancies; and even less so when the latter are considered as a homogeneous whole. Haematology patients often experience bleeding episodes, severe or unusual infections and specific medications (eg, immunosuppressive drugs) that may lead GPs and other generalist physicians to request the transfer of these patients to specialised acute units. Clinical haematologists consulted in focus groups therefore stated that current quality measures were hardly acceptable for patients with haematological malignancies, and that other indicators would reflect more accurately the aggressiveness of care near the end of life.11 In a qualitative interview-based study of 45 British clinicians involved in end-of-life care for patients with haematological malignancies, researchers sought to understand the reasons that could explain the high proportion of patients dying in hospitals.43 Their findings suggest that prognostic uncertainty, unpredictable illness trajectories, and difficulties in identifying when to withdraw active treatments play an important role.
Our findings should be interpreted in light of several limitations. First, data collection was based on a national hospital register, and therefore gives access only to hospital records and not to community-based care providers or nursing home facilities data. Since in-hospital death is often considered as indicative of a form of aggressive care itself, our study focused on a selected population that was more likely to receive aggressive treatments. Nevertheless, in France about 75%–80% of patients with haematological malignancies die in hospitals, and these findings cover the entire country with no selection of the patients based on their healthcare insurance scheme or their affiliation to a specific care provider. It should also be noted that oral molecular targeted therapy or immunotherapy delivered in community pharmacies were not reported in our dataset, which may underestimate the actual use of chemotherapy near the end of life. Second, we relied on ICD-10 diagnosis codes to identify primary and secondary malignancies: since we could not confirm these diagnoses with histological or imaging-based data, we cannot exclude inaccuracies in the characterisation of cancers. Third, we had no access to the date of diagnosis, the disease status, the type and number of disease-directed agents or quality-of-life measures. Furthermore, we had no information regarding surgical procedures and haematopoietic stem cell transplant. Fourth, we based our assessment of the timing of palliative status reporting on ICD-10 coding (Z51.5). This could lead to under-reporting of the actual proportion of patients whose situation was in fact identified and managed as palliative. Finally, our findings may not be entirely generalisable to other healthcare systems or countries.
Conclusion
This article reports the first population-level study comparing the patterns of end-of-life care between different haematological malignancies. Consistently with previous reports, we found high rates of treatment use and low rates of palliative care referral. However, we also found substantial variation according to the type of haematological malignancy. Future studies should therefore differentiate haematological malignancies in the same manner as they differentiate solid tumours. These findings suggest the need for a better and earlier integration of the palliative care approach in the standard practice of haematology, while taking into account the specific needs of patients with advanced haematological malignancies.
Acknowledgments
The authors acknowledge the contribution of the French Technical Agency for Hospital Information (ATIH) during the extraction of the data presented in this article.
References
Footnotes
Contributors LM had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: LM, YB, AC, ED, PR. Acquisition of data: LM, RA, CT. Statistical analysis: LM. Interpretation of data: all authors. Drafting of manuscript or revision for important intellectual content: all authors.
Competing interests None declared.
Ethics approval This study was reviewed and approved by the French National Data protection Agency (CNIL, decision n°DE-2014–112) . In accordance with French regulation, additional ethical permit was not required because of the nature of the data collection (non-interventional study using irreversibly de-identified data related to deceased individuals).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Raw data cannot be made publicly available because of privacy issues. Additional tables can be provided by the authors on reasonable request.