Article Text

Abstract
Background This study was conducted to systematically review the existing literature examining the prevalence of anxiety among hospital staff and identifying the contributing factors to address the complications of this disorder and develop effective programmes for reducing the complications of this mental health problem.
Methods We searched the electronic databases including PubMed, EMBASE, Scopus, Web of Science and Google Scholar from January 2020 to February 2021. To perform meta-analysis, the random effects model was used. To assess the statistical heterogeneity of the included studies, the I2 index was used, and 95% CI was estimated. Data analysis was performed by R software.
Results In the final analysis, 46 articles with the total sample size of 61 551 hospital staff members were included. Accordingly, anxiety prevalence among healthcare workers (HCWs) was 26.1% (95% CI 19% to 34.6%). The prevalence rates of anxiety in health technicians and medical students were 39% (95% CI 13% to 73%) and 36% (95% CI 15% to 65%), respectively, indicating a much higher prevalence than other hospital staff members. Furthermore, a positive significant relationship between prevalence of anxiety among HCWs and their age was approved (p<0.001). The prevalence rate of anxiety was higher among women 37.7% (95% CI 25.4% to 51.8%) than men 27.2% (95% CI 18.2% to 38.6%).
Conclusion The findings show a moderately high prevalence rate of anxiety in hospital staff. Due to the high prevalence of this mental health problem in health technicians, medical students and frontline health workers, it is highly suggested that healthcare institutions offer mental health programmes for these working groups in order to appropriately manage anxiety during the COVID-19 pandemic.
- COVID-19
- hospital care
- depression
- psychological care
Data availability statement
Available on request.
This article is made freely available for personal use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What was already known?
In order to effectively deal with long-term disasters such as pandemics, the success of health systems mainly depends on protecting health workers from physical and mental hazards to ensure the sustainability of health services delivered to patients.
What are the new findings?
Anxiety prevalence among healthcare workers was 26.1% (95% CI 19% to 34.6%). The prevalence rates of anxiety in health technicians and medical students were 39% (95% CI 13% to 73%) and 36% (95% CI 15% to 65%), respectively, showing a much higher level than other hospital staff members.
What is their significance?
Due to the high prevalence of this mental health problem in health technicians, medical students and frontline health workers, it is highly suggested that healthcare institutions offer mental health programmes for these working groups in order to appropriately manage anxiety during the COVID-19 pandemic.
Introduction
In December 2019, a novel type of coronavirus (COVID-19) emerged from Wuhan, China and spread across the world in a short period of time, leading to adverse health effects and several socioeconomic challenges.1 2 During the COVID-19 outbreak, concerns about mental health have increased dramatically and resulted in a growing level of psychological distress among populations particularly healthcare workers (HCWs).3 4 As mentioned in the literature, some of the main factors associated with psychological distress among HCWs are exposure to the virus, concerns about being infected and passing infection on to a vulnerable family member, shortage of personal protective equipment (PPE), heavy workload and the need to work with strict safety measures during the pandemic.5 6 Psychological distress is a common mental health problem linked to stressors that are challenging to deal with in everyday life and poses a direct physical or emotional harm to individuals. Inability to handle stressful situations could be noticed as a wide range of negative outcomes including depression, anxiety, stress, exhaustion and mental morbidity.7 8 Due to role-related stressors and pressures placed on HCWs at work, high levels of mental health problems are expected among these professional groups.3 4
In a study conducted by Vindegaard and Benros, HCWs were reported to have more anxiety, depression and insomnia compared with the general population.9 In a systematic review and meta-analysis by Pappa et al, the prevalence rate of anxiety was estimated to be 23.2% among HCWs during the COVID-19 pandemic.10 Another review which incorporated seven studies from China reported an increased risk of anxiety among health staff compared with other careers.11 In line with previous findings, Buselli et al 12 revealed that frontline HCWs experienced the highest level of anxiety, as they are responsible for providing healthcare services for patients with COVID-19.12 However, evidence has shown that even non-medical personnel working in healthcare institutions are at a high risk of psychological distress.13 14
To address this issue, the WHO emphasised on the necessity of immediate action to both prevent and treat mental health problems among HCWs.15 In fact, in order to effectively deal with long-term disasters such as pandemics, the success of health systems mainly depends on protecting health workers from physical and mental hazards to ensure the sustainability of health services delivered to patients.16 17 An effective strategy towards providing mental health services for HCWs starts with screening the mental well-being of the staff and identifying the sources of psychological distress among them in order to facilitate proper implementation of psychological interventions in the workplace.18 As the world continues to be confronted with the COVID-19 pandemic, mental health support is essentially needed to reduce the psychological issues among healthcare professionals.19 Despite the importance of the issue, there is limited research on anxiety among hospital staff during this pandemic. Furthermore, as anxiety is independent of whether staff are working as a frontline health worker or administrative and support staff in the hospital, we performed an updated systematic review to identify the anxiety prevalence among hospital staff of different professional categories. This systematic review and meta-analysis was conducted to determine the prevalence of anxiety among hospital staff and the impact of various factors contributing to its prevalence in different geographical locations, with a view of identifying possible interventions to address the complications of this disorder.
Methods
Registration and reporting
This systematic review and meta-analysis was registered in PROSPERO database at the University of York (registration code: CRD42021236433; available at: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021236433).
Databases and search terms
In this study, we systematically searched the data resources of Web of Science, PubMed, EMBASE, Scopus and Google Scholar from the outset of 2020 to February 2021. The keywords anxiety, hospital staff, healthcare workers, 2019-nCoV, SARS-CoV-2, COVID-19, Coronavirus and all possible combinations of mentioned words extracted from medical subject headings were applied in the search strategy. The search strategy employed in PubMed was (((Healthcare provider[Title/Abstract] OR Health worker[Title/Abstract] OR Health personnel[Title/Abstract] OR Healthcare Worker[Title/Abstract] OR Health Staff[Title/Abstract] OR Healthcare professional[Title/Abstract]) OR medical staff[Title/Abstract] OR non-medical staff[Title/Abstract] OR hospital staff[Title/Abstract] OR hospital worker [Title/Abstract] OR hospital personnel[Title/Abstract]) AND (anxiety[Title/Abstract] OR anxiety Symptom [Title/Abstract]) OR anxiety disorder[Title/Abstract] AND (Coronavirus[Title/Abstract] OR COVID-19[Title/Abstract] OR COVID-19[Title/Abstract] OR SARS-CoV-2[Title/Abstract] OR 2019-nCoV[Title/Abstract] OR coronavirus disease 2019[Title/Abstract] OR 2019-nCoV[Title/Abstract]))). Through searching the electronic databases, 1298 articles were found which were reduced to 672 records after being imported to EndNote software and removing the duplicates. In the next step, title/abstracts of the remained articles were screened by two researchers independently. Then, the reference lists of selected articles were reviewed to ensure the comprehensive approach to identifying relevant studies.
Inclusion criteria
Different types of studies including cross-sectional, prospective, case–control, case series and cohort studies with the purpose of examining the prevalence of anxiety or determining its contributing factors among hospital staff during the COVID-19 pandemic were included. Furthermore, studies were eligible for inclusion if they were in English language and published between January 2020 and February 2021.
Exclusion criteria
Studies reporting clinical pathways, treatment approaches, medication and selection of an evidence-based set of clinical actions were excluded from the review. In addition, non-English records or papers published outside the time frame defined in the study were not included for further consideration. Finally, systematic reviews, narrative reviews, literature reviews, scoping reviews, rapid reviews, brief reports, expert opinions, letter to the editor, editorials, books, commentaries, thesis and randomised controlled trials were excluded.
Study selection
In the initial step of searching, 1298 records were retrieved from different electronic databases. After entering the articles into EndNote software V.626, studies repeated in various databases were removed. Subsequently, 672 records remained to be screened on the basis of their title/abstracts; of which 204 articles were published in PubMed, 279 in SCOPUS, 78 in Web of Science and 111 in EMBASE. Afterwards, according to inclusion criteria, the full text of remaining articles was evaluated and led to 46 relevant records. Both the processes of screening and data extraction were performed by two independent researchers. In case of any disagreement, the issue was resolved by a third evaluator (figure 1).

Flow diagram of our review process (PRISMA). PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Quality evaluation
Two independent evaluators assessed the methodological quality of selected articles through the use of Newcastle–Ottawa Scale (NOS). With this scale, each of the studies can attain a maximum of 9 points: 4 for exposure assessment of, 2 for comparability and 3 for the outcome assessment. In case of receiving a score of ≥7, the study is mentioned to have high-quality and lowest possible risk of bias. Unreported and referenced items were scored 0 and 1, respectively, and each paper’s total score of quality was estimated by the sum of the scores allocated to the reported items. In this respect, 0 and 10 (the lowest and the highest quality, respectively) were identified as the lowest and highest NOS scores for each paper. Thus, a score below 4 was considered a low-quality article.20
Data extraction
Using a checklist, two study members independently recorded the required data including author/authors’ name, country, sample size, publication date, study design, a summary of study results in terms of reported score of anxiety among hospital staff and quantitative data on determining factors of anxiety. The authors considered the prevalence of anxiety as ‘moderate’ and ‘severe’ rates as just these two groups are counted as mental health problems.21–23
Statistical analysis
To perform meta-analysis, the random effects model was used. The model generalises findings by assuming that included studies are randomly selected from a larger population.24 In order to assess the statistical heterogeneity of the included studies, the I2 index at 95% CI was estimated. To assess publication bias in the meta-analysis, funnel plot asymmetry Egger’s test was used to regress the effect sizes on their SEs. We also performed subgroup analyses to identify sources of heterogeneity in the areas of demographic characteristics and study setting. Data analysis was done in R software.
Results
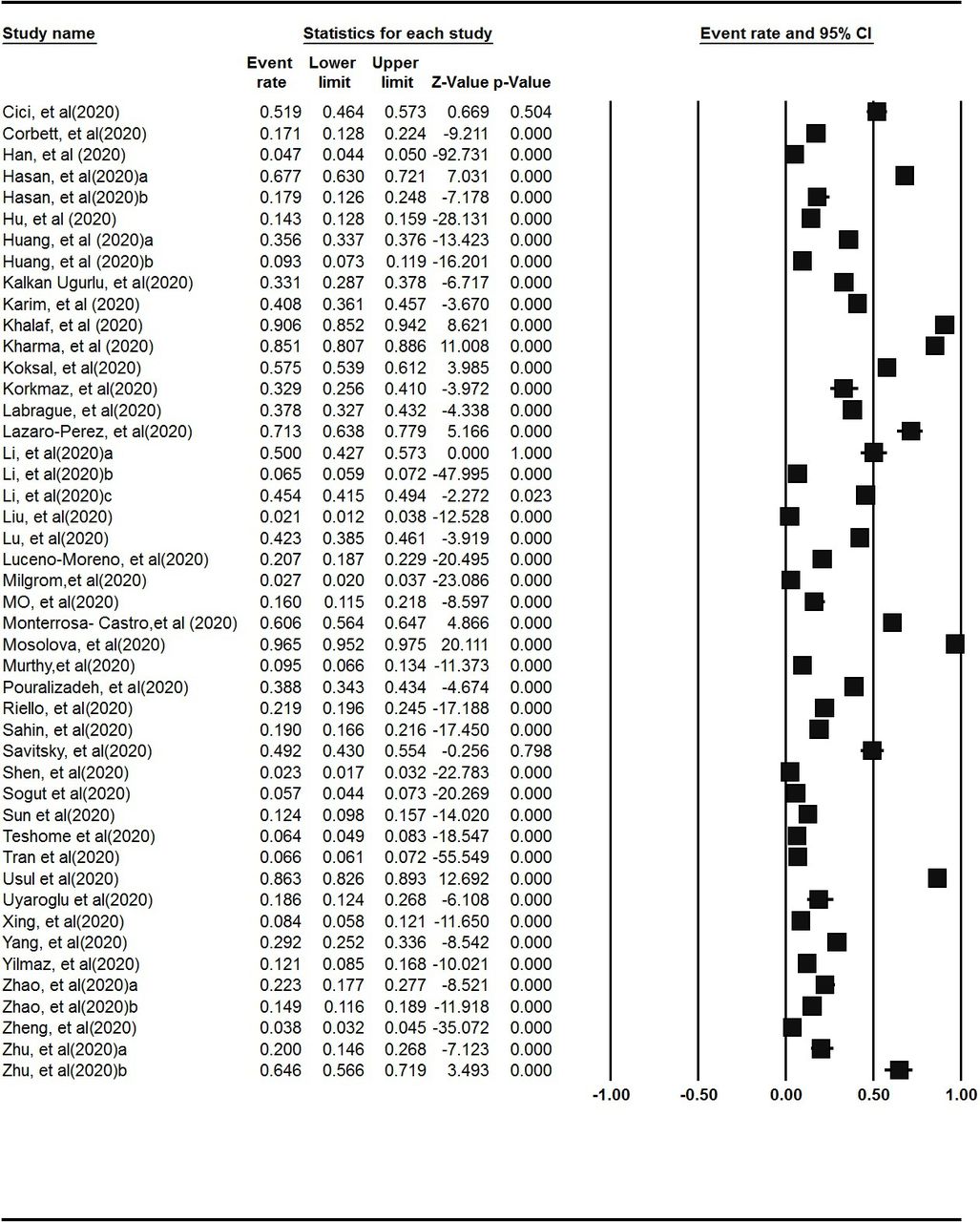
To conduct the systematic review and meta-analysis, Preferred Reporting Items for Systematic Reviews and Meta-Analyses was used.25 From the retrieved articles, 46 articles with the total sample size of 61 551 hospital staff members were included for the final analysis. The estimated overall prevalence of anxiety among HCWs was reported to be 26.1% (95% CI 19% to 34.6%) (figure 2).

The forest plots of prevalence of anxiety in health workers during the COVID-19 pandemic.
Subgroup analysis based on age
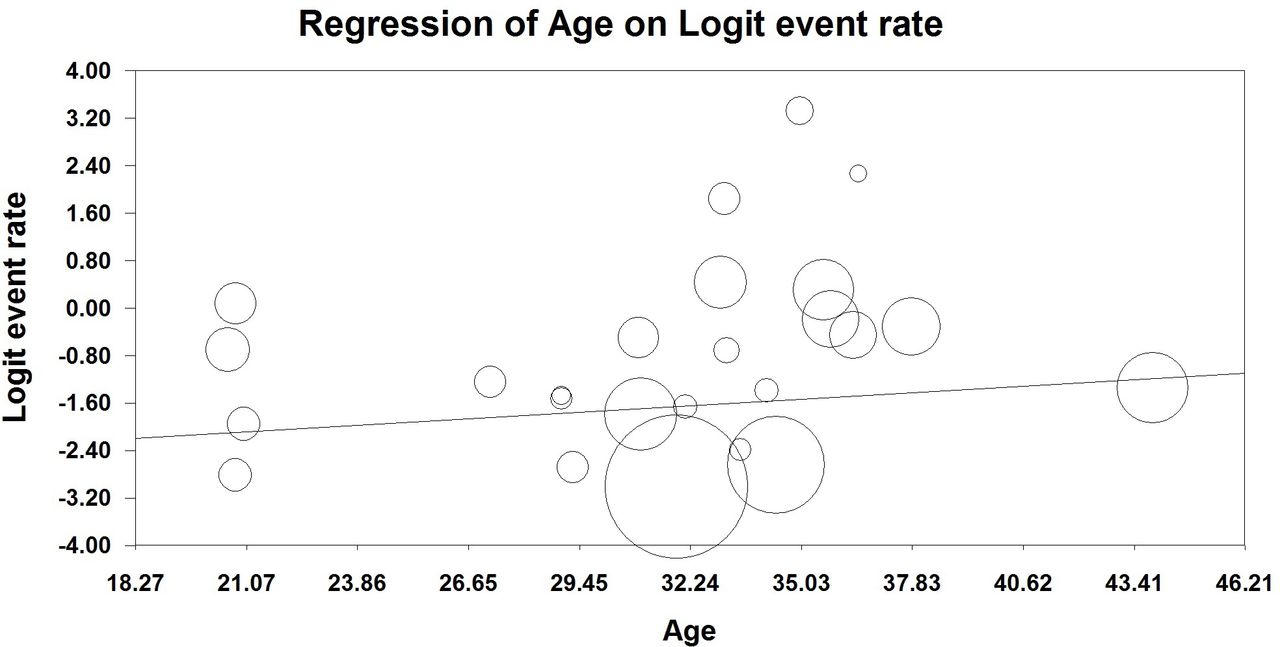
Considering the results shown in figure 3, a positive significant relationship between prevalence of anxiety and age among HCWs was approved. In fact, a year of increase in the age of hospital staff contributed to an increase in the anxiety prevalence by 0.03. The findings also revealed that the highest prevalence rate of anxiety was in the age group between 29 and 36 years old (figure 3).
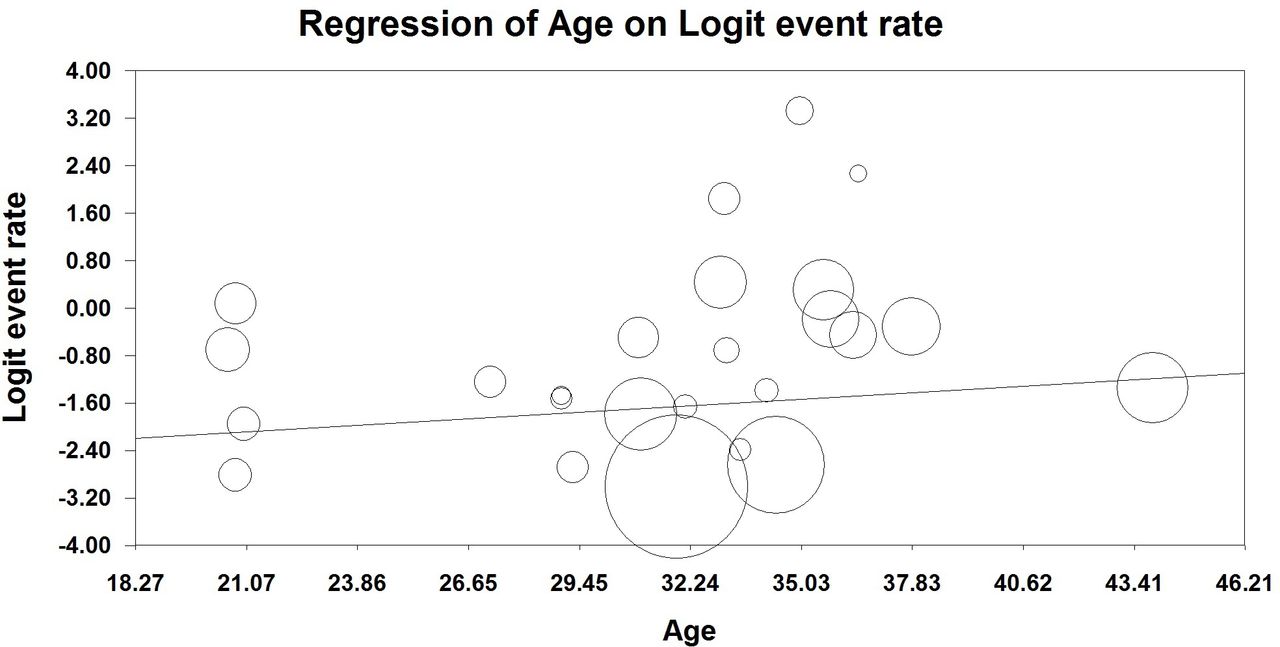
Meta-regression based on age.
Subgroup analysis based on gender
The prevalence of anxiety was higher among women (37.7% (95% CI 25.4% to 51.8%)) than men (27.2% (95% CI 18.2% to 38.6%)) (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-regression based on gender.
Subgroup analysis based on job type
Based on the analysis, the prevalence rates of anxiety among health technicians (39% (95% CI 13% to 73%)) and medical students (36% (95% CI 15% to 65%)) were much higher than other hospital staff members. Furthermore, the lowest prevalence of anxiety was observed to be 7% (95% CI 1% to 34%) among hospital managers. Accordingly, the prevalence rates of anxiety among nurses, doctors, support staff and other hospital workers were reported to be 24% (95% CI 17% to 33%), 24% (95% CI 12% to 40%), 21% (95% CI 0% to 90%) and 33% (95% CI 12% to 64%), respectively (see table 1).
Prevalence of anxiety among health workers during COVID-19 pandemic based on occupations
Meta-regression for continents
Our subgroup analysis revealed that the prevalence of anxiety was the highest (60% (95% CI 56% to 64%)) in the USA and lowest in Asia (19% (95% CI 13% to 28%)). Furthermore, the rates of anxiety in Africa and Europe were estimated to be at 44% (95% CI 39% to 51%) and 43.4% (95% CI 28% to 59%), respectively (table 2).
Prevalence of anxiety among health workers during COVID-19 pandemic based on continents and WHO regions
Meta-regression for WHO regions
Meta-regression based on WHO regions verified that the highest and lowest anxiety prevalence rates belonged to Pan American Health Organization (PAHO) (60.6% (95% CI 56% to 64%)) and African Region Organization (44% (95% CI 39% to 51%)). In addition, the anxiety rates in Western Pacific Region Organization, Eastern Mediterranean Region Organization, European Region Organization and South-East Asian Region Organization were 32% (95% CI 2% to 89%), 40.6% (95% CI 25% to 57%), 37.6% (95% CI 15% to 67%) and 15% (95% CI 1% to 23%), respectively (table 2).
Meta-regression for questionnaires and quality assessment tool
Based on our results, all the included studies had used six valuable and reliable tools. Among these tools, the 21-Item Depression, Anxiety and Stress Scale DASS-21 showed the highest prevalence of anxiety among health workers (42.6% (95% CI 27% to 53%)), however, Hospital Anxiety and Depression Scale showed the lowest rate in this area (25.1% (95% CI 22% to 33%)) (table 3). On the other hand, the results based on the quality assessment showed that more than half of the included studies (n=27) had high quality and there was a higher rate of anxiety among health workers (30% (95% CI 25% to 36%)). In addition, 19 studies were determined to be medium-quality studies with the anxiety prevalence rate of 21% (95% CI 18% to 29%) (table 3).
Meta-regression based on questionnaires and quality assessment tools (NOS)
Discussion
This study is an up-to-date systematic review and meta-analysis reporting the anxiety prevalence and the impact of various contributing factors among hospital staff with a view of identifying possible interventions to address the complications of this disorder. There were 46 articles included in our review, and to the best of our knowledge, this is the first study examining anxiety prevalence in different job groups of hospital staff working in different geographical locations. Our results revealed that the overall estimated prevalence of anxiety among hospital staff in this review was 26.1%, which was higher than those reported by Santabarbara et al and Pappa et al.10 26 The difference might be due to the variability of sample size, data collection and analysis techniques. Another possible reason might be variation in infrastructure provided by different healthcare systems resulting in different levels of focus on mental well-being and psychological support of HCWs. Despite some differences in the value of anxiety prevalence reported in the literature, it is clear that a great number of HCWs worldwide suffer from moderate symptoms of anxiety. The literature has approved that the COVID-19 pandemic has caused serious mental, physical and emotional problems among hospital staff who are at a higher risk of contracting the infection or even passing on the disease to others.27–29 The other cause of anxiety among HCWs might be working in high-infectious work environments with inadequate access to PPE.30
A number of systematic reviews and meta-analyses have reported the prevalence of anxiety among HCWs. Santabarbara et al found that the prevalence rate of anxiety in HCWs was 25% with the highest proportion in doctors and nurses.26 Several studies have affirmed a high level of anxiety among health workers providing care for patients with COVID-19.12 31 32 Although our review showed a relatively high percentage of the prevalence of anxiety among frontline health workers, the highest prevalence rate was reported for health technicians and medical students. Similarly, Nishimura et al 33 remarked that the COVID-19 pandemic had a profound psychological challenge for medical students. Literature affirms that medical students are at the frontline of patient care in hospitals facing stressful work conditions which might place them at a high risk of anxiety. During the COVID-19 pandemic, such tension might be intensified due to the risk of occupational exposure to the virus, work pressures, concerns about PPE shortages and ineffective educational materials for the purpose of e-learning.34 Considering the high prevalence of anxiety in health technicians, Qi discussed that risk of being laid off from work due to economic downsides resulted from the COVID-19 pandemic besides the declining level of participation in social activities that could lead to severe mental health disorders among them.35 Furthermore, the risk of exposure to contaminated blood or infected samples was mentioned as a great concern among health technicians. Common concerns among different healthcare providers included being worried about carrying the virus home, unfamiliarity with the disease and lack of effective treatment approaches.36
Our review also revealed that being male and older in age contributed to higher risk of anxiety among HCWs. In a study conducted by Spoorthy et al,37 older staff members were reported to have higher level of mental distress due to frustration of longer working hours and lack of PPE in the workplace. The research added that health professionals aged 31–40 years were concerned about their family members contracting the virus, while those older than 50 years of age were more likely to report negative mental health effects resulting from anxiety related to exacerbated mortality rates during the COVID-19 crisis. Several studies considered gender as a contributing factor for the prevalence of certain psychiatric disorders including anxiety. Cotton et al stipulated that men had lower levels of knowledge about mental health problems compared with women and were less likely to obtain appropriate mental health services.38 39 Consequently, due to negative psychological health consequences, men might experience more severe symptoms.40 Contrary to our results, earlier studies found that female staff had more anxiety than male workers.17 41 They noticed that women experienced more loneliness during the COVID-19 crisis which might worsen their mental well-being.42 In fact, prior to the pandemic, female health workers used to develop more cooperative working relationships with their colleagues and experienced stronger social support networks while during the outbreak they have felt more loneliness and isolation.43
Regarding the anxiety prevalence across different continents, our findings revealed the highest rate of psychological distress was among HCWs in the USA. Similarly Twenge and Joiner44 mentioned that anxiety symptoms dramatically rose from the onset of the COVID-19 pandemic. In fact, COVID-19 has had a considerable adverse impact on the mental health of the population, particularly those exposed to the virus in their daily work schedule. Thus, provision of mental health services was suggested and implemented in almost all healthcare institutions to help HCWs deal with negative mental health impacts. Furthermore, the highest number of infected HCWs in the PAHO region along with lack of PPE has seriously threatened the safety of staff and put mental pressure on them. To resolve these challenges, the PAHO/WHO has necessitated an improvement in the capacity of healthcare services, provision of appropriate PPE and training of health workers in order to ensure a timely response to the pandemic.45
In our review, the prevalence rates of anxiety in health workers based on NOS quality assessment were 30% in high-quality studies and 21% in medium-quality ones. The study of Kalkan Uğurlu et al, who worked on 411 Turkish hospital staff members, showed high quality based on NOS and reported the anxiety prevalence of about 33%.46 Huang et al, who worked on 2250 Chinese health workers, reported the prevalence of 35% among participants.47 However, in the study of Luceño-Moreno et al on 1422 health workers in Spain, the prevalence of anxiety was reported to be 20%, while we determined it as a medium-quality study.21 This fact indicates that articles with higher quality showed a higher prevalence of anxiety, so these types of articles are more reliable for decision-makers.
In our review, Africa ranked number two among regions of the world in terms of mental health problems, suggesting an immediate action to improve the mental health status of the population. The weakness of African health system has affected a greater number of HCWs to experience severe psychological symptoms.48 Due to the lack of protective equipment, healthcare staff have been at higher risk of being exposed to COVID-19. Shortage of medical devices, besides inadequate access to healthcare facilities, deteriorated the condition.49 Findings also revealed that Asian HCWs had the lowest level of anxiety. Some of the countries including Korea had the capacity to promptly control the COVID-19 crisis through improving their preparedness and timely response to the disease.50 In this country, the government widely tracked the adherence to health and safety protocols by the population and rigidly pursued contact-tracing activities. Increasing testing capacity and setting up comprehensive population testing were other key strategies which were applied by the country.51
Limitations
In the present review, we included a large body of literature and applied a rigorous approach to identify publication bias. However, there are some limitations regarding the study which should be considered while interpreting the results. First, we only incorporated the studies published in English which might result in language bias. Second, most of the included articles were from China which might negatively affect the generalisation of our findings. Finally, the non-uniformity of the data collection tools used to assess anxiety was another source of methodological heterogeneity. Also, there was scarcity of data in some countries and territories which can be explored in the future studies.
Conclusion
The findings show a moderately high prevalence rate of anxiety among hospital staff. This issue highlighted the importance of resolving psychological disorders and reducing their adverse effects through monitoring the anxiety-related symptoms in HCWs. Furthermore, as anxiety might stem from lack of knowledge about the disease and effective coping strategies, it is recommended offering training courses on anxiety and related mental health problems to hospital staff. On the other hand, due to the high prevalence of this mental health problem among health technicians, medical students and frontline health workers, it is suggested that healthcare institutions provide mental health services for these working groups in order to appropriately manage anxiety during the COVID-19 pandemic. The results of our study also affirm that being male and older in age contribute to having a higher risk of anxiety. Thus, paying special attention to these groups is helpful to properly mitigate mental health risk especially for vulnerable groups under pandemic conditions.
Data availability statement
Available on request.
Ethics statements
Patient consent for publication
References
Footnotes
Correction notice This article has been updated since it was first published. The article type has been changed to Systematic review.
Contributors Category 1: Conception and design of study—SR, AG and FPK. Acquisition of data—ZH, FPK, SR, SK, FT, NR, SAhmadi and SAghalou. Analysis and/or interpretation of data—HH, SR and FT. Category 2: Drafting the manuscript—SR, AG and AD. Revising the manuscript critically for important intellectual content—SR, AD, AG, FPK, MM and HS. Approval of the version of the manuscript to be published—SR, AG, SR and HH.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.