Article Text

Abstract
Objectives Advance care planning (ACP) is essential for patient-centred care in the last phase of life. There is little evidence available on the safety of ACP. This study characterises and explores patient safety incidents arising from ACP processes in the last phase of life.
Methods The National Reporting and Learning System collates patient safety incident reports across England and Wales. We performed a keyword search and manual review to identify relevant reports, April 2005–December 2015. Mixed-methods, combining structured data coding, exploratory and thematic analyses were undertaken to describe incidents, underlying causes and outcomes, and identify areas for improvement.
Results We identified 70 reports in which ACP caused a patient safety incident across three error categories: (1) ACP not completed despite being appropriate (23%, n=16). (2) ACP completed but not accessible or miscommunicated between professionals (40%, n=28). (3) ACP completed and accessible but not followed (37%, n=26). Themes included staff lacking the knowledge, confidence, competence or belief in trustworthiness of prior documentation to create or enact ACP. Adverse outcomes included cardiopulmonary resuscitation attempts contrary to ACP, other inappropriate treatment and/or transfer or admission.
Conclusion This national analysis identifies priority concerns and questions whether it is possible to develop strong system interventions to ensure safety and quality in ACP without significant improvement in human-dependent issues in social programmes such as ACP. Human-dependent issues (ie, varying patient, carer and professional understanding, and confidence in enacting prior ACP when required) should be explored in local contexts alongside systems development for ACP documentation.
- Clinical decisions
- Communication
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Healthcare-associated harm poses a major threat to public health and well-being. Palliative care is not exempt from these risks. The World Health Organization (WHO) Universal Health Coverage draws attention to priorities for high-quality, safe palliative care in the last phase of life (ie, people in the last days, weeks or months of life).1 Discordance between patients’ preferences and care received in the last phase of life is common.2 3 Most people express preferences to die at home4 5 but in the UK, and many other countries, most die in hospital.6 Access to palliative care is not equitable. Patients receiving specialist care are more likely to die in their usual place of residence with lower symptom burden.7 Those not known to specialist services are more likely to die in acute hospitals. Numbers and proportion of deaths in hospitals are projected to rise.8 Ascertaining patients’ priorities to improve care and focus resources is paramount. Advance care planning (ACP) may help address these challenges.9 10
ACP is a process of enabling patients to discuss and record goals and preferences for future healthcare with family and healthcare providers.11 UK and international professional guidelines recommend ACP.12 13 ACP can improve outcomes for patients and relatives without causing psychological distress.9 10 14 However poor uptake,3 15 inaccurate or inaccessible documentation,3 16 and variable evidence of benefits are concerns.17 18 A fundamental challenge is that ACP is an intrinsically complex, human-dependent social programme, making it difficult to define and measure,19 compare studies or synthesise results.20 In this study we conceptualise this challenge by using the United States Department of Veterans Affairs (USDVA) Strength of Intervention scale term ‘human-dependent’ as our definition of processes which are necessarily reliant on the choices of individual people.21 22
There remains uncertainty around quality and efficacy of ACP. Little research has focused on patient safety issues within ACP. As ACP is increasingly undertaken, it is important to understand types of patient safety incidents occurring and the underlying factors. Many healthcare systems have committed to learning from patient safety incident reporting systems to improve patient care. The National Reporting and Learning System (NRLS) is the repository receiving such reports from healthcare organisations and members of the public in England and Wales. A patient safety incident is defined as ‘an event or circumstance that could have resulted, or did result, in unnecessary harm to a patient’.23 Reports are written mostly by healthcare professionals and collated via local risk management systems. Each contains structured information about location, patient demographics and reporter perception of harm severity plus free-text descriptions of the incident, most also outline contributory factors and planned actions to prevent reoccurrence. With all reporting systems, caution is required when interpreting data given uncertainties about reporting culture, such as under-reporting and reporter bias.24 25 However, value and utility of structured analysis of incident reports for the identification of improvement priorities, notably in under-researched areas of unsafe clinical practice, has been established.26 27
Policies promoting ACP over the last one to two decades have led to the design of multiple interventions seeking to target ACP. These include interventions to raise awareness,28 29 educate staff,30 31 employ dedicated staff32 33 and improve systems to share ACP.34–36 A significant evidence gap remains: we do not know if these solutions are targeting front-line experiences of process breakdowns or challenges, at all or in the most optimal way.
Aim
To explore and understand patient safety incidents in which ACP, or its absence, contributed to unsafe patient care in the last phase of life.
Objectives
To:
Classify and quantify types of ACP-related patient safety incidents, and their underlying causes through application of a theoretically derived a priori coding framework.
Describe and interpret themes and meta-themes in reports and use this qualitative analysis to identify data-driven theories to focus future improvement work.
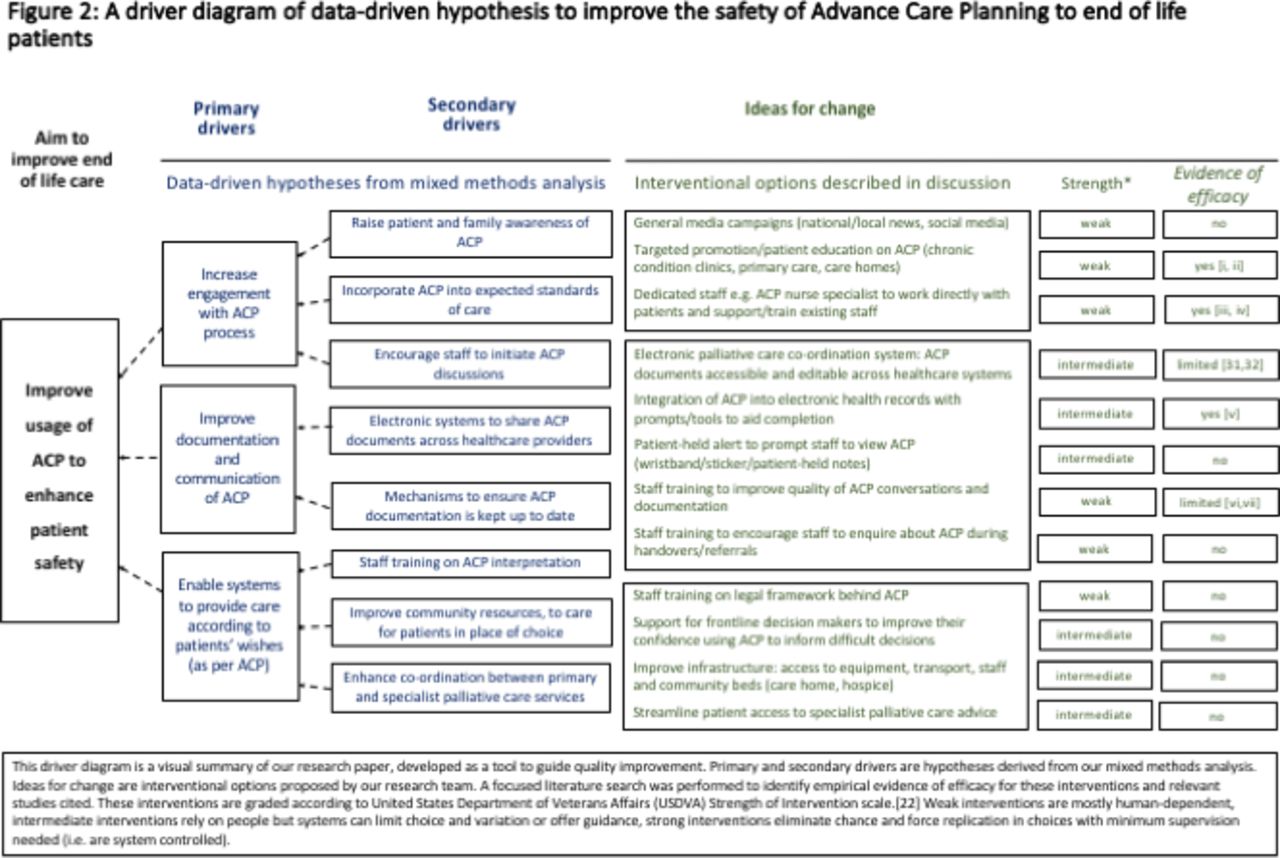
Construct a driver diagram mapping empirically identified ideas for systems improvement derived from objectives 1 and 2.
Methods
Data
Data were taken from all NRLS incident reports that were reported to have occurred between 1 April 2005 and 31 December 2015.
Sample selection
Electronic searching of free-text descriptions was conducted using synonyms of ACP (see online supplementary appendix) identifying 976 reports. Two clinical academics (TD and HW) read and identified reports focused on the last phase of life in which there was a patient safety incident attributed either to ACP or lack of ACP by the reporter. Seventy reports met these inclusion criteria, 906 were excluded (see figure 1). We used consensus clinical judgement to ascertain whether the patient was in the last phase of life alongside proxy indicators including mention of progressive or life-limiting illnesses, a death occurring with a ‘do not attempt cardiopulmonary resuscitation order’ (DNACPR) in place and if the patient was in a nursing home.
Supplemental material

Flow chart of sample identification. ACP, advance care planning; NRLS, National Reporting and Learning System.
Analysis
The free text of each report was analysed by a clinician trained in root cause analysis (TD). An a priori coding framework was used to describe what happened (type of patient safety incident), reported reasons why the error occurred (contributory factors) and resultant harms (outcomes). The framework was theoretically derived previously by patient safety experts and clinicians and aligned to the WHO International Classification for Patient Safety.37 A random sample of 20% of reports was independently reviewed (HW) and inter-rater reliability was assessed. Any uncertainty was discussed with a third reviewer (AC-S). We undertook descriptive analysis of the coded data to assess the most frequent incident types, contributory factors and outcomes. We then grouped the reports according to which stage of the ACP process the incident occurred (i.e. during creation, communication or application of ACP).
All reports with sufficient detail in the free-text fields were also analysed qualitatively using thematic analysis which is a method for identifying anticipated and emergent themes from data.38 It was used to critically analyse each reporter’s stance towards the incident, recognising that reports are socially constructed through the perspective of the reporter. Data-derived emergent codes were identified in vivo from the reports by TD and independently by SY. These codes were then integrated into themes (collections of interrelated codes) through discussion (TD and SY). This iterative method and the evolving codes/themes developed and followed established qualitative research principles.39 40
Synthesis
The mixed-methods analysis was integrated and synthesised in a driver diagram, an established quality improvement tool used to highlight priority areas for change41 (Figure 2). We have contextualised our findings by conducting focused searches to identify existing ACP interventions and evidence of efficacy.
{kind=link}
{kind=link}
A driver diagram of data-driven hypotheses to improve the safety of advance care planning (ACP) to end-of-life patients22
Results
Seventy incident reports were included. Of these, 50% (n=35) were reported to have occurred in acute hospitals, 27% (n=19) in care homes, of which 20% were nursing (n=14) and 7% residential care (n=5). The remaining 23% (n=16) occurred in private homes. No reports described hospice incidents.
Three main types of incident were identified:
ACP not completed despite being appropriate (23%, n=16).
ACP completed but not accessible or miscommunicated between healthcare professionals (40%, n=28).
ACP completed and accessible but not followed (37%, n=26).
Intercoder agreement for coding incident type was high with a Cohen’s κ co-efficient=0.82.
Each report was numbered 1–70 and quotes have been drawn for illustrative purposes. Free-text reporting has been lightly edited (denoted by square brackets) for anonymity and comprehension.
ACP not completed despite being appropriate
In 16 reports (23%) the reporter believed ACP would have enhanced care and lack of ACP contributed to the incident. Most of these reports contained no evidence of ACP discussions or documents (14%, n=10). Several demonstrated conflicts felt by clinicians between allowing natural death and feeling obliged to sustain life at all costs:
ECP [Emergency care practitioner] asked to attend call to administer analgesia to anaemic patient complaining of abdominal pain. Patient had refused to attend hospital. On arrival, patient was Cheyne-Stoking with little cardiac output. Son and daughter were in attendance but refused to let ECP commence life-saving procedures or to phone for back up. They stated that the patient did not want any intervention. ECP asked whether there was a living will and was told there was not. ECP informed family that he had an obligation to commence CPR [Cardiopulmonary Resuscitation] if needed but family adamant that this should not be done. ECP also stated would not give any analgesia as it would kill the patient and this could be seen as homicide. (report 3)
In six reports ACP discussions had taken place but were not documented or up to date:
We rushed him onto the ambulance and onto the stretcher where CPR was started. The family expressed he had a living will that was due to be updated by the GP [general practitioner] with a DNACPR [Do not attempt cardiopulmonary resuscitation]. Until we could speak to GP we continued ALS [advanced life support]. GP clarified DNACPR had been discussed and that it would be 'grossly inappropriate' to continue. ROLE [Recognition of life extinct] performed. (report 45)
ACP completed but not accessible or miscommunicated between healthcare professionals
Twenty-eight reports (40%) described problems with effective communication. Most of these described documentation being lost, inaccurate or unavailable (27%, n=19). Transition of care was often a contributory factor. In 12 reports, ACP documents were unavailable following transfer of the patient as typified by the following example:
Patient with [neurodegenerative disorder] attended Accident & Emergency – DNACPR form and living will brought in from home but not returned when patient discharged, therefore when patient suffered cardiac arrest at home DNACPR paperwork not available and [ambulance service] forced to perform full ALS treatment. As a result patient suffered the indignity in death that he had taken every step to prevent. (report 10)
In several reports ACP documents could not be located quickly enough during an acute deterioration resulting in inappropriate intervention such as CPR:
After arriving and doing full CPR and ALS for 20 min the patient regained an output, no respiratory effort. The decision to move the patient to the ambulance was made at this point. After placing the patient in a chair to take downstairs the nurse in charge gave me a piece of paper and said I needed to read it, this was an advance decision to refuse treatment (ADRT). (report 22)
Five reports described breakdowns in verbal communication and two described problems with verbal communication and documentation. Poor handover between teams within a setting caused similar problems:
Living will not handed over by MAU [Medical Admissions Unit] staff nurse so cardiac arrest call done and resuscitation CPR commenced. (report 21)
ACP completed and accessible but not followed
In 26 reports (37%) ACP was completed, and documents accessible, but the ACP was not followed. In nine reports (13%) CPR, judged to be inappropriate by the reporter, was performed. In five reports the DNACPR decision was part of the ACP. In four reports the details of the DNACPR decision were not recorded:
She did not want to be resuscitated and indeed she did not want to go to hospital. I subsequently filled out the End-of-Life Care Pathway; a yellow End-of-Life Form was completed on [date] and faxed to the Ambulance Service […] For reasons I do not know, a second ambulance was called. The upshot of this is that a drip was inserted; she was taken into hospital with the family in hot pursuit clutching the yellow form with the DNR [Do Not Resuscitate] on it and they were explicit that she would not have wanted to go to hospital. (report 23)
Six reports described treatment other than CPR, occurring against the wishes expressed in the ACP. Treatment-related errors included delayed or inadequate treatment and overtreatment. These included placement of a nasogastric tube or reversal of hypoglycaemia with an intravenous infusion against the patient’s recorded wishes, which had been seen by the staff involved.
A further eight reports described failure to achieve preferred place of care. This was due to unavailability of hospice beds, community staff, medication or an inappropriate transfer to acute hospital for life-sustaining treatment:
Patient admitted for diamorphine and hyoscine pump as nursing home unable to obtain drugs. Patient has a living will specifying not for admission to hospital. (report 9)
Resource constraints only accounted for five reports in which ACP was not followed; staff perceptions and interpretation of ACP was a bigger factor in this data set. Misunderstanding about what constitutes a valid ACP and how mental capacity is defined and represented in law was an underlying theme in many reports:
I looked at the will noting that it was drawn up in [date: 1 year prior] and that it was not signed by a doctor or medical professional. I stated that the document was not binding and that it would be illegal for me not to treat the patient […] The daughter arrived and I was asked not to treat her mother. I informed her that I could not stop until the patient had the mental capacity to tell me to stop. (report 20)
Poor understanding of palliative care principles also caused some patient safety incidents. Here a misconception led to an inappropriate admission, despite the fact the patient had made plans to die at home with an ACP, equipment and medication arranged:
Patient commenced on a syringe driver [date] as terminally unwell. OOH [out of hours] GP called out around 18.00 on [date] which resulted in patient being admitted for rehydration (IV [intravenous] fluids) as the family reported that they were told he was in pain due to being dehydrated at this point the patient was unable to drink due to his deteriorating condition. Anticipatory medications were all available in the house. (report 27)
Cross-cutting themes and consequences—interpretative synthesis integrating mixed-methods findings
We identified some cross-cutting themes that were present across the reports, regardless of whether the patient safety incident was due to lack of ACP being completed, communicated or enacted when needed. Relatives commonly assumed they held authority to make decisions on behalf of someone who lacked capacity. This led to conflict with professionals whose fear of medicolegal consequences arising from withholding interventions was evident. Words such as ‘obligation’ and ‘forced’ were used in descriptions about life-sustaining treatment or CPR, suggesting staff felt pressure to provide treatments and lacked confidence in assessing if ACP was applicable, and if they were ‘allowed’ to make decisions to withhold interventions.
‘Decision-maker availability’ created challenges where front-line staff (mainly nurses and paramedics) did not feel able to choose a palliative approach over life-sustaining treatment (whether ACP was completed or not) and had difficulty contacting a senior decision-maker (usually a GP, or other senior doctor).
‘Conflict between staff’ as to what course of action should be taken was also present. This may reflect different levels of palliative care experience but is more likely to reflect the complexity of using ACP to guide decision-making. Differing terminology used to refer to ACP may have also contributed to ambiguity in interpretation. There was evidence of staff confusing ACP with DNACPR:
Ambulance crew misunderstood that presence of Advance Care Plan was not necessarily indicative of a DNACPR order. In fact child was for full resuscitation and this was documented on Advance Care Plan. (report 61)
Many incidents caused distress to patient, families and staff, with organisational consequences such as use of ambulances and inappropriate hospital admission causing pressures on resources. The untoward outcomes most commonly described were inappropriate CPR attempts present in 19 reports (27%). Together these are encapsulated in this example:
Resuscitated and return of spontaneous circulation after 15 min, intubated and ventilated and transferred up to critical care. Family very angry that despite highlighting medical alert bracelet that stated patient has a living will nothing done and patient ended up in a situation which they would not have wanted. (report 31)
Our overarching analysis is integrated and synthesised in a driver diagram (figure 2) mapping data-driven theories (primary and secondary drivers arising from our analysis) to change ideas with matched evidence-based interventions (when possible). The strength of interventions is graded using the USDVA classification.22
Discussion
ACP is advocated to align care with patients’ wishes and prior healthcare decisions. Our national-level analysis of patient safety incidents demonstrates deficits throughout ACP processes including problems with creation, communication and application of ACP to guide decision-making. This is the first analysis of patient safety incidents relating to ACP. The study provides empirical evidence of the suboptimal and unsafe care received by patients as a result of issues concerning ACP.
In around a quarter of incidents analysed, lack of ACP creation contributed to an incident. Low uptake of ACP is a well-described problem for which there are many postulated causes.42 Barriers include a perceived lack of skill by clinicians, fear of depriving patients of hope, confusion over responsibility, timing and initiation of discussions.43 Lack of public awareness and societal reluctance to talk about death could also be factors.42 Interventions aimed at increasing uptake of ACP can be effective, the most successful are complex interventions that address multiple barriers.10 Any initiative to improve ACP must ensure relevant staff have the confidence to initiate, create and enact ACP.
Lack of accurate and timely communication of ACP was the most commonly reported incident which is consistent with previous work.3 16 Patients in the last phase of life often have multiple pathologies and complex needs. They are likely to seek care from numerous healthcare providers. A reliable system for communicating ACP across services is key to providing safe, effective care. Electronic palliative care coordination systems (EPaCCS) have been advocated as a solution for this.44 There are many EPaCCS internationally34 35 45 varying considerably in format and scope. ‘Coordinate my Care’ in London reports a large majority of patients dying in their preferred place of care and suggests a reduction in hospital admissions.45 Studies show EPaCCS can improve data sharing34 and influence care decisions. However data sets are small and concerns remain about the lack of high-quality evidence for the efficacy of EPaCCS46 which can be burdensome to use with technical issues and duplication of work.47 48 Systems for communicating ACP information across providers should be robustly evaluated with the aim of developing systems that balance data security, accessibility and usability, and are integrated with existing systems.
Most existing studies focus on improving uptake and documentation of ACP, with a paucity of evidence looking at application and impact on clinical decision-making.18 ACPs may not be followed even when adequately communicated. From our analysis of incident reports, a lack of staff understanding of ACP is a key contributory factor affecting all stages of ACP. Previous studies have demonstrated a lack of confidence and knowledge about ACP among GPs affecting the initiation of ACP49 and among paramedics affecting interpretation of ACP.50 Our study adds further evidence demonstrating that lack of staff understanding of ACP can contribute to unsafe and inappropriate care. More research is needed to understand how to enable clinicians to create and use high-quality ACP to guide decision-making.18 Interpretation and application of ACP is complex and requires higher-level meta-cognitive skills, confidence, experience and emotional intelligence. Fear of medicolegal consequences of making the wrong decision regarding life-sustaining treatments is justified by high-profile cases in which healthcare professionals have been punished for not attempting CPR, which was felt to be futile.51 Improving timely access to advice in support of these complex decisions for staff is critical, but potentially a cultural shift is also required to empower staff to use their professional judgement and to protect them when they do so. ACP is an inherently human-dependent process, so it is critical that interventions tackle these human-dependent concerns as well as the systems involved.
Given the patient impact of ACP incidents the low volume of reports related to ACP does not necessarily indicate that ACP is a relatively safe process. Under-reporting is a recognised issue with safety incident reporting24 25 and thus these reports are likely to represent the tip of an iceberg. Most NRLS reports are received from acute/general hospitals which may have impacted on the population of incidents from which our sample was selected since we would expect most ACP incidents to occur in community settings. Another possibility is that ACP is not widely perceived as a patient safety issue. Patient safety in palliative care has had less scrutiny and is less clearly understood than in disciplines such as surgery or critical care.52 In the UK the National Institute for Health and Care Excellence first published guidance on ACP in 2004.53 The National End of Life Care strategy (2008, updated 2014) was a crucial policy publication increasing interest in ACP.44 Our study period covers 2005–2015. This study contributes an important analysis of incidents faced by vulnerable people at a time of evolving policy and increasing use of ACP, highlighting front-line challenges in ACP implementation and extending what is known by deepening understanding of how and why unsafe care is occurring. The full impact of continued publication of policies and guidance for ACP remains unknown especially as later policy documents appear to assume that ACP creation and communication have occurred effectively and focus on ensuring ACP is enacted.54
Our analysis has extracted valuable learning about how failures in ACP can cause harm and distress and identified principles that are generalisable. The methods used for this work further contribute to the literature by offering a replicable approach for analysis of other local or national databases. This evidence can be used to illuminate the design of solutions; drawing on our analysis in such designs will bring about a greater chance of success.
Conclusion
Breakdowns in ACP occur due to lack of completion, lack of communication or lack of trust at the moment the enactment is required. Incidents occur in all three of these sequential elements of ACP because of human-dependent issues impacting on the entire process; these issues relate to wider societal concerns, beliefs and misconceptions about medicolegal frameworks, organisation of services with front-line professionals lacking decision-making capacity and the complexities of actual processes in clinical situations which inevitably do not follow linear descriptions of intended processes in policy.
Further work should focus on measuring the impact of improvement activities targeting ACP human-dependent and systems elements to improve the safety of care for patients in the last phase of life. Our findings question whether it is possible to develop strong system interventions to ensure safety and quality in ACP without significant improvement in human-dependent concerns such as patient, carer and professional understanding of ACP and the trustworthiness of enacting prior ACP. Achieving this should be explored in local contexts alongside systems development for recording and accessing ACP documents so that quality as well as quantity of ACP usage improves. Rigorous evaluation of ACP initiatives is needed, with dissemination of results to ensure the safest, highest quality and most effective models can be replicated and adapted to local contexts.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
References
Footnotes
Funding This research was funded by Marie Curie and by the Scientific Foundation Board of the Royal College of General Practitioners (Grant No MC 2016-06). The funders had no involvement in the study design, data analysis, writing of the report or decision to publish.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.